Imaging of concomitant pulmonary and hepatic hydatid cysts in a young Ethiopian farmer
Elias Belete, Francesco Capriotti, Carolina Vitale, Carlo Airola

TL;DR
A young Ethiopian farmer had both lung and liver hydatid cysts detected through imaging, emphasizing the importance of imaging and prevention in endemic areas.
Contribution
This case highlights the concurrent occurrence of pulmonary and hepatic cystic echinococcosis in an Ethiopian patient.
Findings
Imaging revealed calcified liver cysts with the classic cerebral gyri sign.
The patient had concomitant pulmonary and hepatic hydatid cysts.
Preventive education is needed in endemic regions for cystic echinococcosis.
Abstract
A 30-year-old female farmer from South-West Shewa, Ethiopia, presented with chest and abdominal pain. Imaging revealed concomitant pulmonary and hepatic cystic echinococcosis, with calcified liver cysts showing the classic cerebral gyri sign. According to WHO guidelines, pulmonary surgery was advised, while hepatic cysts warranted observation. Serology was unavailable, and the patient was lost to follow-up. This case highlights imaging as a key diagnostic tool and the need for preventive education in endemic settings.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
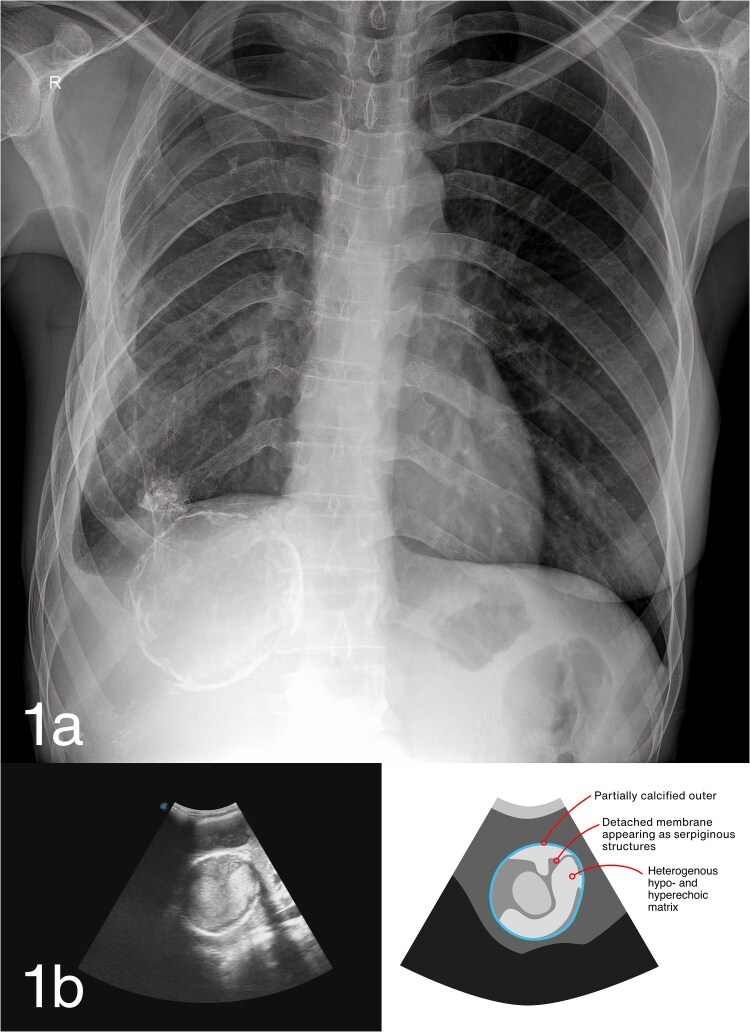 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsParasitic infections in humans and animals · Amoebic Infections and Treatments · Parasites and Host Interactions
A 30-year-old female farmer from South-West Shewa, Oromia, Ethiopia, presented with 3–4 weeks of dull right lower chest and upper abdominal pain. She reported no fever, cough, or systemic symptoms. The patient owns cattle and dogs, regularly handling livestock and dogs, including home slaughtering and feeding raw offal to dogs, common practices in her rural community [1, 2]. On medical evaluation, vital signs were normal and physical examination was unremarkable. Laboratory tests showed mild neutrophilic leukocytosis (WBC 13600/mm^3^; neutrophils 10 700/mm^3^); liver enzymes were normal. Echinococcus serology was unavailable, representing a limitation for the diagnosis.
Chest radiograph posteroanterior view (Fig. 1a) showed a well-circumscribed radio-opacity (approximately 2 cm) in the right lower lobe. A ring-calcified lesion (approximately 8 cm) was noted in the right upper abdominal quadrant. Abdominal ultrasound using a 3.7–4.5 MHz convex probe (Fig. 1b) identified two cystic lesions (6 cm and 8.5 cm) in hepatic segments VI and VII, respectively, with heterogeneous internal contents, partial wall calcification, and the classic ‘cerebral gyri’ sign.
Hepatic hydatid cysts (WHO CE4) with probable pulmonary involvement were diagnosed. Differential diagnoses included hepatic tumors or abscesses, but the characteristic ultrasound appearance was diagnostic. She was referred for thoracic surgery because, according to WHO guidelines, pulmonary cysts require surgery before albendazole administration [3]. Follow-up is recommended for CE4 hepatic cysts (‘watch and wait’), as they are unlikely to contain viable protoscoleces but carry a risk of reactivation. The patient was lost to follow-up due to financial constraints. Hydatid disease caused by Echinococcus granulosus is endemic in Ethiopia. While local prevalence data are lacking for South-West Shewa, cystic echinococcosis has been reported at around 30% in bovine, 7.4% and 16,6% in caprine and ovine respectively, and 37% in dogs in other districts of Oromia [4]. Humans are accidental intermediate hosts that ingest eggs shed from dog feces. The liver is the most frequently affected organ, followed by the lungs. Simultaneous hepatic and pulmonary involvement occurs in 4–25% of cases [5]. Imaging findings, including calcified cyst walls and cerebral gyri sign, can guide diagnosis in resource-limited settings. This case highlights the importance of community education on safe livestock practices, early detection, and structured follow-up. Limitations include absence of serological confirmation and loss to follow-up.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sendekie B, Gebeyehu B, Mihret A. et al. Epidemiological study on bovine cystic echinococcosis: abattoir survey, cyst characterization and its economic impact at Mekaneyesuse municipality abattoir, Northwest Ethiopia. Parasite Epidemiol Control 2024;25:e 00355. 10.1016/j.parepi.2024.e 0035538800636 PMC 11127200 · doi ↗ · pubmed ↗
- 2Mathewos M, Dawa D, Yirgalem M. et al. Cystic echinococcosis in cattle slaughtered at a slaughterhouse in Gessa, southern Ethiopia. Parasite Epidemiol Control 2022;18:e 00262. 10.1016/j.parepi.2022.e 0026235874493 PMC 9304873 · doi ↗ · pubmed ↗
- 3World Health Organization . WHO guidelines for the treatment of patients with cystic echinococcosis. World Health Organization: Geneva, 2025, Licence: CC BY-NC-SA 3.0 IGO.40690566 · pubmed ↗
- 4Shumuye NA, Ohiolei JA, Gebremedhin MB. et al. A systematic review and meta-analysis on prevalence and distribution of Taenia and Echinococcus infections in Ethiopia. Parasit Vectors 2021;14:447. 10.1186/s 13071-021-04925-w 34488862 PMC 8419976 · doi ↗ · pubmed ↗
- 5Aghajanzadeh M, Safarpoor F, Amani H. et al. One-stage procedure for lung and liver hydatid cysts. Asian Cardiovasc Thorac Ann 2008;16:392–5. 10.1177/02184923080160051018812348 · doi ↗ · pubmed ↗