Serological Response to COVID-19 Vaccination in Saudi Arabia: A Comparative Study of IgG and Neutralising Antibodies Across Vaccine Platforms
Mariam M. AlEissa, Ahdab A. Alsaieedi, Reema Alduaiji, Fahad Almsned, Yousif AlDossary, Nada Saleh, Raghad A. AlQurashi, Esraa A. Hawsa, Muath b Ben Shaded, Amer M. Alshehri, Osamah T. Khojah, Eyad Y. Abu Sarhan, Hamad H. Alonazi, Walid A. Nouh, Khalid H. AlAnazi

TL;DR
This study compares how well different COVID-19 vaccines boost antibody levels in Saudi Arabia, finding mRNA vaccines like Pfizer and Moderna are most effective.
Contribution
The study provides region-specific real-world data on vaccine immunogenicity in Saudi Arabia, including insights into heterologous vaccination schedules.
Findings
Pfizer and Moderna vaccines induced stronger antibody responses compared to AstraZeneca.
Heterologous vaccine schedules showed comparable or enhanced immunogenicity compared to homologous schedules.
High prior SARS-CoV-2 exposure was indicated by 75.4% IgG positivity at baseline.
Abstract
Background: In the Kingdom of Saudi Arabia, various COVID-19 vaccines were administered during the pandemic. However, region-specific real-word comparative data on their immunogenicity remain limited. This study aimed to assess the serological responses to Pfizer-BioNTech (BNT162b2), Moderna (mRNA-1273), and AstraZeneca (ChAdOx1 nCoV-19) vaccines in a diverse population living in KSA. Methods: This observational study included 236 adults recruited from vaccination sites in Riyadh. Participants provided serum samples at predefined intervals: before the first dose, after the first dose, after the second dose, and post-vaccination infection (if applicable). IgG and neutralising antibodies were quantified using ELISA assays. Demographic and vaccination data, and their associations with antibody responses, were evaluated. Results: At baseline, 75.4% of participants were positive for…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
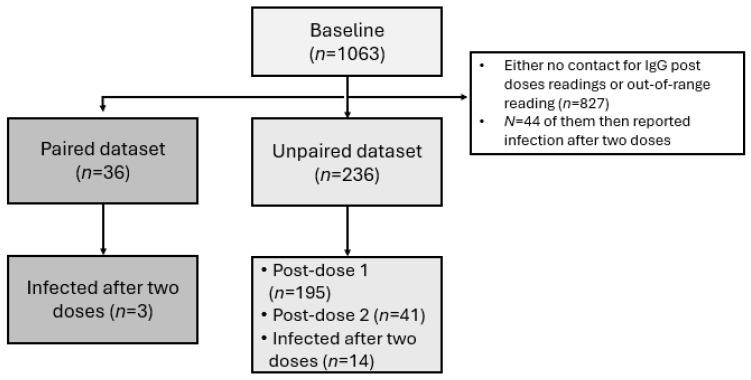 Figure 1
Figure 1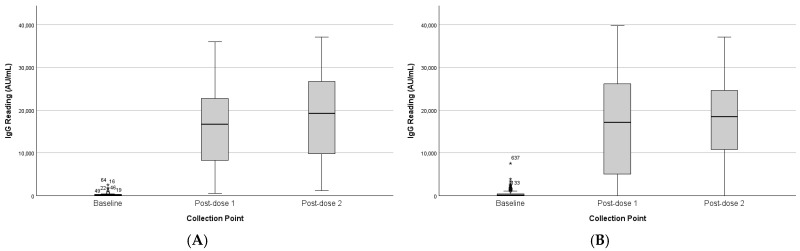 Figure 2
Figure 2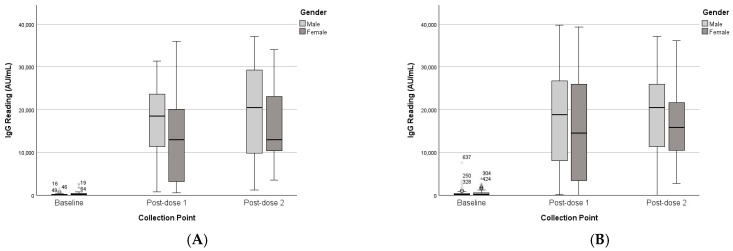 Figure 3
Figure 3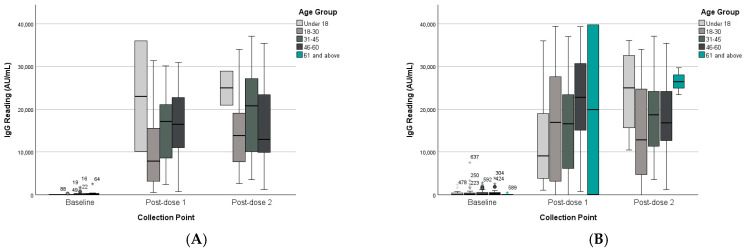 Figure 4
Figure 4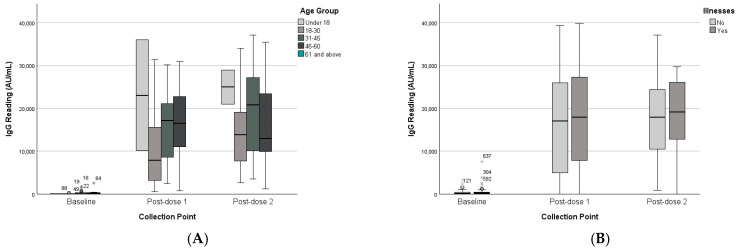 Figure 5
Figure 5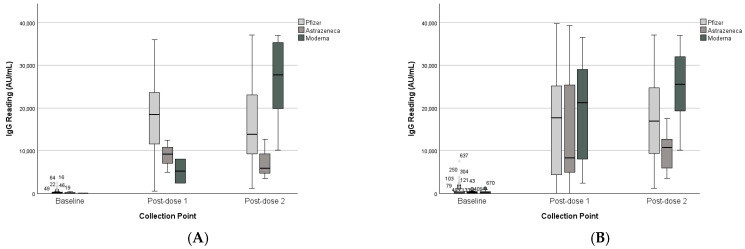 Figure 6
Figure 6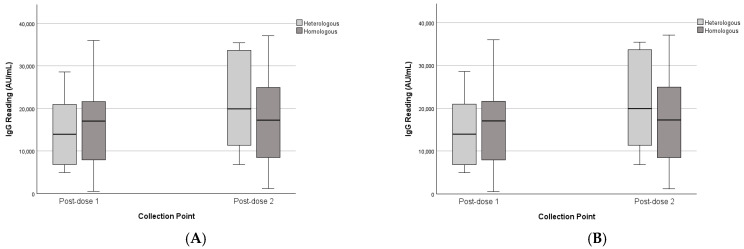 Figure 7
Figure 7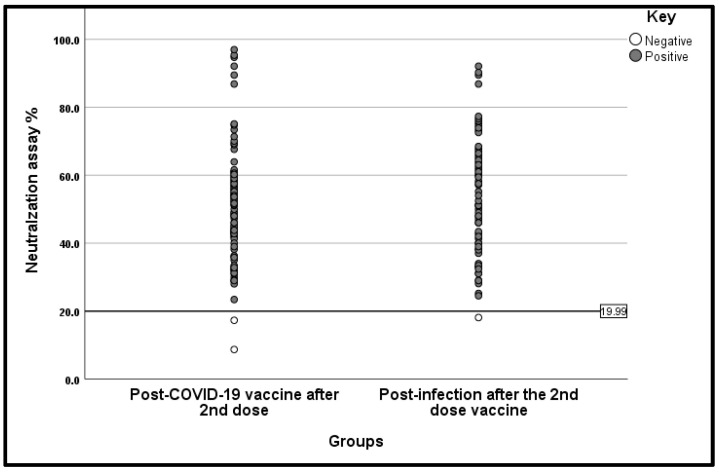 Figure 8
Figure 8Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSARS-CoV-2 and COVID-19 Research · Vaccine Coverage and Hesitancy · COVID-19 epidemiological studies
1. Introduction
An unknown respiratory disease was documented in December 2019 in Wuhan, the province of Hubei, China [1]. Next-generation sequence (NGS) was performed on samples obtained from infected patients, and the results identified the etiological agent as a novel betacoronavirus [2]. Scientists were subsequently able to isolate and characterise the pathogen, now known as Severe Acute Respiratory Syndrome coronavirus 2 (SARS-CoV-2) [3]. The World Health Organisation (WHO) named the diseases coronavirus disease 2019 (COVID-19) [4,5].
The U.S. Food and Drug Administration (FDA) issued an Emergency Use Authorisation (EUA) for the Pfizer-BioNTech COVID-19 vaccine [6]. The Saudi FDA registered the vaccine and approved its importation and use in the Kingdom of Saudi Arabia [7]. The vaccine is indicated for active immunisation to prevent COVID-19 in individuals 12 years of age and older. Its mRNA, encapsulated in lipid nanoparticles, enables delivery into host cells for expression of SARS-CoV-2 spike (S) antigen, thereby triggering an immune response [6]. Subsequently, the European Medicines Agency granted conditional marketing authorisation for the AstraZeneca ChAdOx1 nCoV-19 (AZD1222) vaccine [8], which was also approved for importation and use by the Saudi FDA [9]. Since then, multiple vaccines have been developed and released, with updated regulations for age-specific eligibility and booster dose recommendations [10]. Several studies worldwide have assessed vaccine efficacy [11,12], including some research conducted in Saudi Arabia. However, our study aims to evaluate the immunological profile and validate the efficacy of COVID-19 vaccines (BNT162b2 Pfizer-BioNTech, and ChAdOx1 nCoV-19 (AZD1222) AstraZeneca) in the Saudi population.
2. Methodology
2.1. Ethical Approval
The ethical approval was obtained from the Central Institutional Review Board at the Ministry of Health Ethics Committee, Saudi Arabia (approval number IRB-21-55M; National Registry Number NCBE-KACST, KSA(H-01-r-009)). The SFDA approved the application (application number 21061802).
2.2. Participant Recruitment and Sample Collection
The samples were collected from participants visiting vaccination sites in the Riyadh region between October 2021 and July 2022. Recruitment was conducted collaboratively between the Public Health Authority (PHA) and the Ministry of Health (MOH). The study included Saudis and non-Saudis, healthy males and females aged 16 years and older, who were vaccinated with one of the following vaccines: Moderna (mRNA-1273) from ModernaTX, Inc., (Cambridge, MA, USA), Johnson & Johnson (JNJ-78436735) from Janssen Biotech, Inc. (a Johnson & Johnson company), (Horsham, PA, USA), Pfizer BioNTech (BNT162b2)from Pfizer Inc., (New York, NY, USA), and BioNTech SE, Mainz, Germany, or AstraZeneca (ChAdOx1 nCoV-19) from AstraZeneca, (Cambridge, United Kingdom). Pregnant women and individuals with prior viral infection were excluded. Samples were collected at three time points: baseline, post-dose 1, and post-dose 2. A fourth group included participants with confirmed COVID-19 infection despite vaccination. All participants provided informed consent to participate in this study and for follow-up sample collection. A sample of 4–5 mL of blood was collected in a plain tube from each participant and left for 30 min to clot. Then, the samples were transported to the PHA laboratory at 2–8 °C and received on the same day. Each participant was assigned an identifier number. The samples were subsequently centrifuged at 1000–1300× g for 10 min.
2.3. IgG & Neutralising Antibody Assays
The serum was isolated in a separate tube and stored at −80 °C. IgG levels were measured using Abbot’s SARS-CoV-2 IgG enzyme-linked immunosorbent assay (ELISA) kit (Abbott Laboratories, Abbott Park, IL, USA). The neutralisation assay on serum samples was conducted using the Invitrogen competitive SARS-CoV-2 Neutralising Antibody ELISA Kit, following the manufacturer’s instructions. Prior to the assay, the serum samples were diluted 1:50 with 1× Assay Buffer. The neutralisation percentage (%) was determined using the formula:
The methodology, as described previously by Bhadauria et al. and Choe et al. [13,14], involved reporting the mean inhibition percentages observed in duplicate wells. To determine the presence of neutralising antibodies against the SARS-CoV-2-RBD antigen, a positivity cutoff of ≥20.0% was established. Percentages below 20% were considered negative, based on the set criteria [13,14].
2.4. Statistical Analysis
Statistical analyses were conducted using IBM SPSS Statistics version 30.0. This was a longitudinal study with a high dropout rate, which resulted in substantial missing data; therefore, imputation techniques were considered inappropriate. Cases with only a single data point were excluded. The remaining cases were classified into two analytical datasets: a paired and an unpaired dataset.
The paired dataset included participants with complete IgG recordings across all three time points and was analysed to assess within- and between-subject effects using repeated-measures ANOVA. The unpaired dataset comprised both the paired participants and those with one missing time point, with each data point treated as a separate observation. This approach provided a confirmatory analysis of the between-group differences identified in the paired dataset, using the Mann–Whitney U test and the Kruskal–Wallis test.
3. Results
After applying exclusion criteria and accounting for missing data, the study included a total of 236 participants, of whom only 36 (15.25%) were paired participants. The participants were 110 females (46.6%) and 126 males (53.4%). Most participants were aged 31–45 years (45.3%), followed by 18–30 years (29.7%), while only 2.1% were above 60 years. Chronic illness was reported by 19.1% of participants, most commonly hypertension (4.2%), diabetes (3.4%), asthma (1.7%), and cancer (1.7%).
The majority received the Pfizer vaccine as the first dose (83.9%), while 7.2% received AstraZeneca and 8.9% Moderna. For the second dose, Pfizer remained the most frequent (43.6%), followed by Moderna (19.9%) and AstraZeneca (2.5%), though one-third had unknown records. Only a small subset (3.4%) received heterologous schedules, while 10.2% received homologous schedules, with the remainder undocumented. At baseline, 75.4% were IgG positive, indicating previous infection with COVID-19. A total of 5.9% of the participants were infected after two doses; all of these were female (Table 1, Figure 1).
3.1. Overall IgG Response Across Time Points
Analysis of the paired sample showed a significant effect of collection point on IgG levels (F(2,34) = 75.36, p < 0.001). IgG increased sharply from baseline (M = 350 AU/mL) to post-first dose (M = 16,350 AU/mL) and post-second dose (M = 18,605 AU/mL). Pairwise comparisons revealed significant increases from baseline to both post-dose points (p < 0.001), with no difference between the two post-dose measures (p = 0.818). (Table 2 and Table 3). The findings were consistent with those of the unpaired group, as shown in Figure 2.
3.2. Impact of Demographic Factors (Co-Variates)
3.2.1. Gender
While males’ IgG readings were higher than those of females, the analysis of the paired dataset revealed that gender did not significantly moderate changes in IgG levels over time (F(2,33) = 1.26, p = 0.297), nor was there a significant main effect of gender on IgG levels (F(1,34) = 2.10, p = 0.157). See Table 2 and Table 3. The unpaired dataset analysis was consistent with the paired dataset findings, confirming that gender was not a significant between-subject factor and that immune responses were comparable across genders, as shown in Figure 3.
3.2.2. Age Groups
The results of age group analysis indicated no significant interaction between collection point and age group (F(6,60) = 0.54, p = 0.774), and age group did not significantly affect overall IgG levels (F(3,31) = 0.88, p = 0.463). See Table 2 and Table 3. The analysis of the unpaired dataset for age as a between-subject factor was consistent with the paired dataset findings., as shown in (Figure 4).
3.2.3. Chronic Disease Status
Chronic illness status was also tested as a within- and between-subjects factor, and neither significantly moderated changes over time (F(2,33) = 0.10, p = 0.905) nor had a main effect on IgG levels (F(1,34) = 0.20, p = 0.654). See Table 2 and Table 3. The findings were aligned with the unpaired dataset analysis, as shown in Figure 5.
3.3. Vaccine Platform Comparison
The analysis for the paired group revealed no significant interaction between collection point and first-dose vaccine type (F(2,33) = 2.60, p = 0.090), though Pfizer recipients exhibited higher mean IgG levels compared to AstraZeneca and Moderna at both time points. For the second dose, there was a significant interaction between collection point and second-dose vaccine type (F(2,29) = 5.67, p = 0.008), See Table 2 and Table 3. For both first and second doses, vaccine type was not statistically significant as a between-subject factor in the paired group, as illustrated in Figure 6.
In the unpaired group, second-dose vaccine type was a significant between-subject factor (p = 0.030). Pairwise comparisons revealed a statistically significant difference between Moderna and AstraZeneca (p = 0.012), while the difference between Moderna and Pfizer approached significance but did not reach the threshold (p = 0.056).
3.4. Heterologous vs. Homologous Schedules
The heterologous and homologous schedules were tested as a between-subjects factor. There was no significant interaction between collection point and vaccination schedule (F(1,30) = 1.36, p = 0.252), nor a significant main effect of schedule (F(1,30) = 0.15, p = 0.703). This was consistent with the unpaired dataset analysis.
As shown in Figure 7, both heterologous and homologous recipients exhibited similar IgG distributions, with a trend toward higher median levels in the heterologous group at post-second dose, though differences were not significant.
We also investigated the serum neutralising activity of 162 participants who had previously tested positive for SARS-CoV-2 IgG antibodies, with a median IgG titre exceeding 6620.35 AU/mL. Among these participants, 159 of 162 (98.1%) exhibited positive neutralising activity within the two groups (Figure 8). Our findings indicated a slight, non-significant increase in serum neutralising activity in patients who were previously infected after receiving the second dose, compared with non-infected participants who had received the COVID-19 vaccination after the second dose (53.3% and 50.6%, respectively) (p value = 0.343).
4. Discussion
This study provides insight into the serological response to the Pfizer-BioNTech (BNT162b2), Moderna (mRNA-1273), and AstraZeneca (ChAdOx1 nCoV-19) vaccines administered in Saudi Arabia in 2021. Participants showed high baseline IgG positivity prior to vaccination, with 73.1% positivity, suggesting significant undocumented or asymptomatic SARS-CoV-2 exposure. This level of positivity does not result from prior exposure to other endemic human coronaviruses due to the high specificity of the detection method employed. However, these figures are considerably greater than post-vaccine levels measured in this study, indicating waning IgG levels in line with the decline observed after months of infection [15]. This reinforces the likelihood that undocumented previous infections contributed to our cohort’s relatively high seroprevalence. This baseline finding also aligns with previous seroprevalence studies conducted in Saudi Arabia, which reported exposure within the community during the early stages of the pandemic [16,17].
The significant rise in IgG levels following administration of the first dose, especially with the Pfizer vaccine, is consistent with many studies demonstrating the strong immunogenicity of mRNA platforms [18]. Pfizer’s strategy of utilising a nucleoside-modified mRNA encoding the spike protein of SARS-CoV-2, delivered via lipid nanoparticles, effectively promotes dendritic cell presentation and elicits a rapid antibody response [19]. AstraZeneca’s more conservative response to the first dose may be explained by pre-existing immunity to the adenoviral vector, which reduces the effectiveness of this vaccine [20].
Following the second dose, we noted the greatest increase in IgG levels in individuals who received the Moderna vaccine. This is consistent with similar studies of immunogenicity conducted in the U.S. and Europe, which showed that Moderna’s vaccines elicited higher peak antibody titres compared with Pfizer’s [21]. The disparities might be partially explained by the greater mRNA content of Moderna’s vaccine (100 µg vs. 30 µg for Pfizer) and the longer interval between doses (28 days vs. 21 days). Our results align with recent international reports, such as Barros-Martins et al. (2021) and Pozzetto et al. (2021) [11,22], which demonstrated that heterologous vaccine regimens, especially combinations of vector priming and mRNA boosting, appear to enhance immunogenicity. In our study, heterologous vector-mRNA schedules elicited comparable or superior IgG responses relative to homologous regimens, particularly when mRNA platforms were included. Similarly, durable IgG responses have been observed in regional studies from Saudi Arabia [23]. However, unlike those studies, our study directly assessed both binding (IgG) and functional neutralising antibodies across multiple two-dose platforms within the Saudi population. This provides important, region-specific evidence that complements the global literature and addresses the limited data available from the Middle East. These findings also contribute to the expanding evidence from other countries and reinforce the need for flexible vaccination planning in response to changing epidemiological conditions [24].
The results regarding neutralising antibodies from our study confirm the findings related to IgG, as 98.1% of those who tested positive for IgG also had neutralising activity. Such a high agreement reinforces the conclusion that anti-spike IgG titres can serve as proxies for functional protection. Many researchers have reported high IgG levels and neutralisation capacity, alongside expected protective clinical outcomes against symptomatic COVID-19 and hospitalisation [25]. This concordance also adds confidence that our serological findings are meaningful proxies of protective immunity, as highlighted in multiple reviews [25,26]. These results further strengthen WHO and local policy recommendations regarding prioritisation of second-dose completion and support the use of antibody monitoring in evaluating vaccination strategies.
In our study, we found no significant differences in IgG titres by age or gender. This was expected, given that our study population was relatively young and therefore unlikely to demonstrate age-related differences due to immunosenescence [27]. Although some literature indicates that females tend to have stronger antibody responses to vaccination [28,29], this pattern may not have been captured in our dataset due to insufficient statistical power. Further Saudi-based age-stratified studies are needed to explore the impact of these variables, particularly in elderly and immunocompromised populations.
One of the strengths of our study is the assessment of vaccine combinations and their immune responses in a Middle Eastern population, which has been underrepresented in vaccine research. This region-specific evidence strengthens the contribution of our study, since regional data on COVID-19 vaccine immunogenicity remain sparse compared with Western cohorts, yet are essential for shaping public health policies tailored to Saudi Arabia. Nonetheless, it is important to consider some limitations. Primarily, a significant part of our study population lacked follow-up data beyond the second vaccine dose. This was due to challenges in data collection during an active public health crisis, especially during rapidly evolving vaccination campaigns and shifting public health strategies. These gaps limited our ability to analyse antibody decline or medium-term responses beyond the early post-vaccination phase.
In addition, while the serological data presented here are essential for understanding levels of humoral immunity, we did not assess T-cell responses or the activation of memory B-cells. The ability to mount long-term protection, especially against newly emerging variants, depends significantly on cellular immunity. With the continuous emergence of new variants, there is a need for future longitudinal research focused on vaccine efficacy that integrates cellular immunity data.
As for other limitations, although neutralising antibodies were detected using an ELISA-based competition inhibition method, we did not conduct live-virus or pseudovirus neutralisation assays, which could shed light on variant-specific protection. These approaches are especially important in light of newer subvariants such as Omicron BA.5, XBB, and others that test the limits of vaccine-induced immunity [30]. This limitation is particularly relevant given published evidence that first-generation Wu-1-based vaccines elicit little or no neutralising activity against newer Omicron NB sublineages, underscoring the importance of updated vaccine formulations [29,30,31]. Recent studies have shown that bivalent and updated mRNA vaccines targeting Omicron sublineages elicit broader neutralisation profiles, reflecting the continual evolution of vaccine strategies in response to emerging variants [31,32].
Regardless of the constraints, our study has important implications for public health policy in Saudi Arabia and comparable regions. First, it confirms that all licensed COVID-19 vaccines elicit robust immune responses, particularly when full vaccination courses are completed. Second, the finding that Moderna’s mRNA vaccine achieved higher efficacy further supports its prioritisation in booster campaigns among high-risk groups or its long-term use in vulnerable populations. Lastly, the demonstrated potential for a platform-agnostic approach could help guide national policy strategies, especially during vaccine shortages.
Nonetheless, sustained surveillance of population-level antibody dynamics can help track community/herd immunity thresholds and inform strategic preparedness for pandemics. Surveillance is particularly valuable for distinguishing between immunity induced by vaccine and infection in populations such as Saudi Arabia’s, where mixed immunity patterns exist. Our results should encourage public health officials in Saudi Arabia to incorporate immune response data into vaccine policy planning. This further highlights the importance of developing national immunological surveillance programs, as emphasised in Saudi Vision 2030 health security initiatives.
5. Conclusion
The response to COVID-19 vaccination in Saudi Arabia showed strong IgG and neutralising antibody responses, particularly with mRNA vaccines. Pfizer generated the strongest early IgG response, while Moderna achieved the highest titres after the second dose. Most participants with positive IgG also demonstrated neutralising activity. These findings support ongoing vaccine deployment and the adoption of flexible vaccination strategies, such as heterologous boosting, to enhance population immunity. Taken together, our results not only confirm global trends but also provide valuable regional-specific evidence that can inform Saudi vaccination policy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1WHO COVID-19 Public Health Emergency of International Concern (PHEIC)2020 Available online: https://www.who.int/publications/m/item/covid-19-public-health-emergency-of-international-concern-(pheic)-global-research-and-innovation-forum(accessed on 1 November 2024)
- 2Cucinotta D. Vanelli M. WHO declares COVID-19 a pandemic Acta Biomed. Atenei Parm.20209115710.23750/abm.v 91i 1.9397 PMC 756957332191675 · doi ↗ · pubmed ↗
- 3Guan W.J. Ni Z.Y. Hu Y. Liang W.H. Ou C.Q. He J.X. Liu L. Shan H. Lei C.L. Hui D.S. Clinical Characteristics of Coronavirus Disease 2019 in China N. Engl. J. Med.20203821708172010.1056/NEJ Moa 200203232109013 PMC 7092819 · doi ↗ · pubmed ↗
- 4Al Eissa M.M. Almsned F. Al Qurashi R. Alsanosi S.M. Alshanberi A.M. A Alsaieedi A. Alkharji R.R. Halawani A.J. Alsaieedi A.A. Saleh N.M. Perceptions of Saudis Toward Participating in the COVID-19 Convalescent Plasma Clinical Trial Cureus 202315 e 4887910.7759/cureus.4887938106720 PMC 10724773 · doi ↗ · pubmed ↗
- 5WHO Naming the Coronavirus Disease (COVID-19) and the Virus That Causes It 2019 Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance/naming-the-coronavirus-disease-(covid-2019)-and-the-virus-that-causes-it(accessed on 26 November 2023)
- 6U.S Food & Drug Pfizer-Bio N Tech COVID-19 Vaccines 2021 Available online: https://www.fda.gov/emergency-preparedness-and-response/coronavirus-disease-2019-covid-19/pfizer-biontech-covid-19-vaccines(accessed on 14 September 2023)
- 7SPA SFDA Approves Registration of Pfizer-Bio N Tech COVID-19 Vaccine The official Saudi Press Agency 2020 Available online: https://www.sfda.gov.sa/en/released-vaccines(accessed on 22 July 2023)
- 8Astra Zeneca Astra Zeneca Welcomes Court Ruling on Supply of Its COVID-19 Vaccine to Europe Astra Zeneca Cambridge, UK 2021