The “sandwich” procedure for paracentral rheumatoid corneal perforation: a case report with 6-year follow-up and literature review
Yi Zhang, Hanjing Liu, Qing Li, Yan Zhu, Yu-guang Zhu

TL;DR
A new surgical procedure called the 'sandwich' method successfully treated a rare corneal perforation in a patient with rheumatoid arthritis, maintaining vision for six years.
Contribution
The paper introduces the novel 'sandwich' surgical procedure for treating paracentral rheumatoid corneal perforation.
Findings
The 'sandwich' procedure provided tectonic support and stabilized the corneal perforation.
The patient maintained 20/50 best-corrected visual acuity over a 6-year follow-up.
This is the first reported use of the 'sandwich' procedure for this specific condition.
Abstract
Rheumatoid arthritis (RA) is a chronic systemic autoimmune disease often associated with ocular manifestations. In rare cases of RA, paracentral rheumatoid corneal perforation may occur. We report the case of a 53-year-old monocular woman with a 20-year history of RA who presented to the clinic with a paracentral corneal perforation. Slit-lamp examination revealed a 2-mm diameter paracentral perforation with an iris plug. The patient was clinically diagnosed with sterile rheumatoid corneal perforation. We describe an innovative “sandwich” procedure developed for addressing the corneal perforation. Initially, a partial thickness limbal groove was created outside the perforation, followed by the formation of a semicircular intrastromal pocket extending approximately 2 mm inside the perforation edge. A lamellar graft was then fashioned and inserted into the intrastromal pocket.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
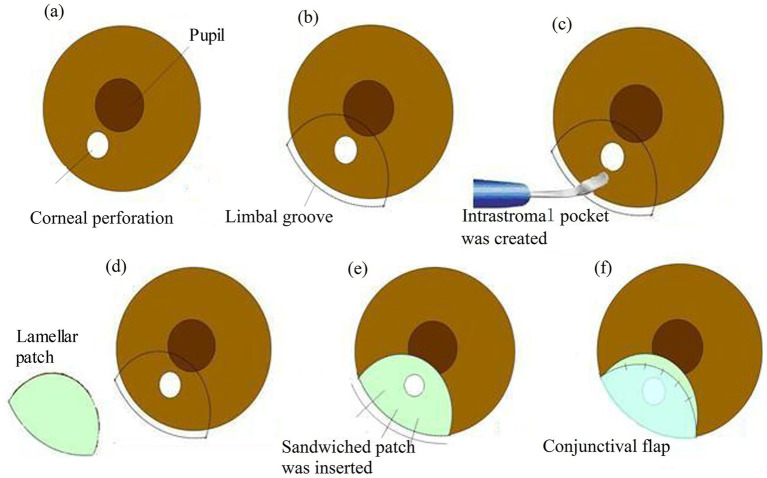 Figure 1
Figure 1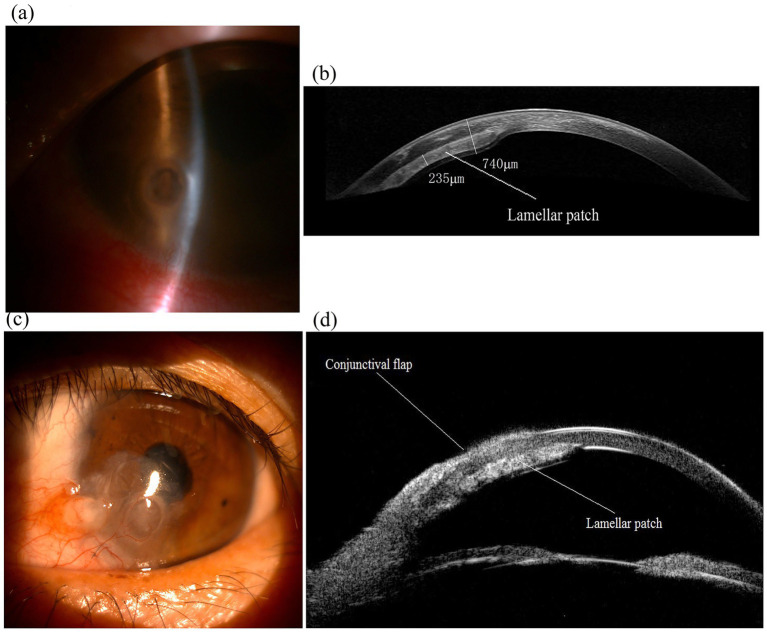 Figure 2
Figure 2- —Scientific Research Project of the Affiliated Hospital of Shandong Second Medical University
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCorneal surgery and disorders · Intraocular Surgery and Lenses · Corneal Surgery and Treatments
Introduction
1
Rheumatoid arthritis (RA) is a prevalent systemic autoimmune disorder, often associated with various ocular manifestations. These include severe dry eye syndrome (aqueous tear deficiency), Sjögren’s syndrome, peripheral ulcerative keratitis, scleritis, and corneal melting, all of which have been extensively documented (1).
Although paracentral rheumatoid corneal perforation is a rare complication in RA patients, it poses significant risks, including severe anatomical distortion of the eye and consequent visual impairment (2, 3). In the most severe cases, corneal perforation can lead to blindness. Prompt surgical intervention is crucial for managing corneal perforations (4). However, the scarcity of fresh corneal tissue presents a significant challenge in treatment (5).
In this report, we present a novel “sandwich” technique for addressing a paracentral corneal perforation (2 mm in diameter) in a monocular patient with rheumatoid arthritis. The procedure involved creating a semicircular intrastromal pocket and inserting a sandwiched patch into it. The technique was further reinforced with a conjunctival flap.
Case presentation
2
A 53-year-old monocular female with a 20-year RA history presented to the clinic with a paracentral corneal perforation. Her ophthalmic history indicated complaints of pain and a foreign body sensation in her left eye, with corneal ulceration developing 1 month ago. Despite ongoing treatment with topical 0.5% ofloxacin eyedrops administered six times daily, she was referred to the clinic due to a sudden vision decrease in her only eye. The best-corrected visual acuity (BCVA) was measured at 20/200 in the left eye, with the right eye having been enucleated. Slit-lamp examination identified a 2-mm diameter inferonasal paracentral perforation with an iris plug and a shallow anterior chamber was observed. The clinical diagnosis was sterile paracentral rheumatoid corneal perforation.
Subsequently, an intrastromal allograft keratoplasty combined with a conjunctival flap, referred to as the “sandwich” procedure, was performed on the affected eye the following day.
Surgical procedure
2.1
The “sandwich” procedure is detailedly shown in Figure 1.
The “sandwich” procedure. (a) A paracentral corneal perforation. (b) The demarcation of the perforated corneal area (ensure a margin of at least 2 mm from the inner edge of the perforation) in a semicircular configuration. (b) A partial thickness limbal groove (radius approx. 6.0 mm) was made outside the perforation. (c) The corneal intrastromal pocket was created using a crescent knife. (d) The lamellar graft (radius approx. 5.5 mm) was cut in a semicircular shape. (e) The sandwiched patch (thickness approx. 220–250 μm) was inserted into the designed intrastromal pocket and the groove was secured with 10-0 mono-filament nylon sutures. (f) Conjunctival flap covered the perforated area of the cornea.
Following the careful demarcation of the perforated corneal area to ensure a margin of at least 2 mm from the inner edge of the perforation in a semicircular configuration. A limbal groove with a thickness of 400 mm was created outside the perforation using a diamond knife.
Subsequently, a side incision was made with a stab knife. Sodium hyaluronate (15 mg/mL) was then injected into the anterior chamber to release the pluged iris.
A semicircular intrastromal pocket was fashioned, extending approximately 2 mm inside the perforation edge, using a crescent knife. A lamellar patch dissection of the donor tissue was performed to remove the epithelium, endothelium, and anterior stroma. The lamellar graft was shaped into a semicircular form, slightly smaller than the intrastromal pocket, and was gently inserted into the pocket. The groove was then securely closed with three interrupted 10-0 monofilament nylon sutures.
In this case, a conjunctival flap was necessary to cover the perforation area. This flap, away from the visual axis, was affixed to the healthy cornea with five interrupted 10-0 nylon sutures. The suture knots were buried.
Finally, the sodium hyaluronate was thoroughly washed out, and the side incision was checked for water tightness.
Postoperatively, the patient was prescribed topical 0.5% levofloxacin and 1% ciclosporin eyedrops four times daily for 1 month, followed by 1% ciclosporin eye drops four times daily for a further 2 months. The 1% ciclosporin was then gradually tapered to once daily over several months. Currently, maintenance therapy with topical 0.4% hyaluronic acid is being administered.
Follow-up included physical examinations, anterior segment optical coherence tomography (OCT), and ultrasound biomicroscopy (UBM) scans (Figure 2). No intraoperative or postoperative complications were observed, and the ocular surface remained stable. The postoperative corrected distance visual acuity (CDVA) was 20/50 in the only eye at 6 months and remained stable over a 6-year follow-up period.
Images of the only eye of an 53-year-old female patient with a paracentral corneal perforation and performed the “sandwich” procedure. (a) Preoperative slit-lamp photograph showed a 2-mm diameter inferonasal paracentral perforation and iris plug in the only eye. (b) Anterior segment OCT imaging of the eye 6 years after the “sandwich” procedure, displaying lamellar patch (sandwiched patch) remains in position (thickness approx. 220–250 μm). (c) Slit-lamp photograph of the eye 6 years after surgery, showing the eye maintains a stable ocular surface. (d) UBM imaging of the eye 6 years after surgery showed the “sandwich” configuration.
Discussion
3
Corneal perforations can result in various degrees of ocular tissue damage and visual impairment (2). The predominant cause of corneal perforation is microbial infection (3), which is responsible for most central corneal perforations. In contrast, peripheral corneal perforations are primarily secondary to degeneration, autoimmune diseases, and microbial infections. The topical application of certain medications, including antibiotics, corticosteroids, and nonsteroidal anti-inflammatory drugs (NSAIDs), may initiate or exacerbate corneal melting, potentially leading to corneal perforation (6).
This report described the case of paracentral corneal perforation in a RA patient. But unknown causes were responsible for the perforation without history of ocular infection or trauma in the only eye. Aqueous tear deficiency, severe dry eye, keratolysis, and superficial corneal ulceration associated with RA may have contributed to the corneal perforation (7, 8).
Management of corneal perforation necessitates a tailored approach based on the perforation’s status and the patient’s medical history. Bandage soft contact lenses, tissue glue (9), medication administration (10), amniotic membrane transplantation (AMT) (11), descemet stripping automated endothelial keratoplasty (DSAEK) (12), and conjunctival flaps (13) are not suitable for the large corneal perforations (≥2 mm diameter), which require therapeutic keratoplasty (1).
Penetrating keratoplasty (PKP) is a predominant surgical intervention for addressing corneal perforation, aimed at preserving the structural integrity of the globe and restoring visual function (14). However, the scarcity of donor corneas poses a significant challenge to the widespread implementation of PKP, particularly in developing countries such as China (15).
The shortage of fresh donor tissue has led to the utilization of cryopreserved corneas for treating corneal perforation. In emergency situations, lamellar keratoplasty (LKP) may serve as an effective procedure for peripheral corneal perforation (16). In cases of central corneal perforation, LKP is considered a temporary measure, with the expectation that subsequent transplantation with fresh donor tissue will yield superior visual outcomes.
Intralamellar autopatch was used for paracentral corneal perforation (17). The procedure was reported to avoid the central sutures into the visual axis. However, the larger surgical wound, graft-host junctional opacification and peripheral suture-induced astigmatism hinder substantial visual improvement.
As a lamellar graft, standard DSAEK was performed for corneal perforation (12). The technique avoided suture-related complications and encroachment of the graft-host junction. However, DSAEK remained limited in most cases of corneal perforation for endothelial immune rejection, corneal endothelium damage, and scarcity of fresh donor corneas.
Although intrastromal LKP has demonstrated potential efficacy in treating pellucid marginal degeneration (PMD) (18), its use in addressing corneal perforation has not been previously documented.
In this report, we introduce the “sandwich” procedure for managing paracentral corneal perforation (2 mm in diameter) using cryopreserved donor tissue. Intrastromal LKP provided sufficient tectonic support, suggesting its potential utility in treating corneal perforation, particularly in patients with severe ocular surface diseases such as RA, where therapeutic PKP often yields suboptimal outcomes. Additionally, a conjunctival flap was employed to facilitate corneal healing in this case.
The intrastromal lenticule obtained from small-incision lenticule extraction (SMILE) procedure was used as a patch graft in LKP to address corneal thinning and perforation (19, 20). This approach partially mitigates the scarcity of fresh donor corneas. Single-layer lenticule is insufficiently thick for use in the “sandwich” technique. However, double-layer lenticules may prevent bulging and protrusion of the patch graft within the lamellar plane with more complex procedure (19).
The procedure effectively preserved the transparency of the visual axis and improved visual acuity. This method provides a simple way to close sterile paracentral corneal perforations without requiring intraocular intervention. For peripheral corneal perforation, intrastromal tamponade using a lamellar allograft may be a viable option.
Imaging assessments, including anterior segment optical coherence tomography (OCT) and ultrasound biomicroscopy, showed that the globe was intact and that the donor graft was providing sufficient tectonic support after a 6-year postoperative follow-up.
The “sandwich” technique presents several limitations. Firstly, the overlap of the surgical area with the pupil and the thickening of the recipient cornea resulted in the irregular astigmatism, potentially limited visual improvement. Secondly, the “sandwich” technique may not be suitable for addressing central perforations or large paracentral perforations exceeding 3 mm in diameter. Thirdly, the conjunctival flap increases the risk of corneal vascularization (15), it may facilitate corneal healing and offer more advantages than disadvantages for this patient with a long history of rheumatoid arthritis.
Conclusion
4
We introduce an innovative “sandwich” technique for the management of paracentral corneal perforation utilizing cryopreserved donor tissue. This “sandwich” procedure successfully provided adequate tectonic support for the patient’s sole functional eye, leading to the stabilization of the ocular surface. This case indicates the potential applicability of this approach in the treatment of corneal perforation, especially in patients with severe ocular surface diseases, such as RA, where therapeutic PKP frequently results in suboptimal outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Artifoni M Rothschild PR Brézin A Guillevin L Puéchal X. Ocular inflammatory diseases associated with rheumatoid arthritis. Nat Rev Rheumatol. (2014) 10:108–16. doi: 10.1038/nrrheum.2013.185, PMID: 24323074 · doi ↗ · pubmed ↗
- 2Timlin HM Hall HN Foot B Koay P. Corneal perforation from peripheral ulcerative keratopathy in patients with rheumatoid arthritis: epidemiological findings of the British Ophthalmological Surveillance Unit. Br J Ophthalmol. (2018) 102:1298–302. doi: 10.1136/bjophthalmol-2017-310671, PMID: 29246891 · doi ↗ · pubmed ↗
- 3Abd Elaziz MS Zaky AG El Saebay Sarhan AR. Stromal lenticule transplantation for management of corneal perforations; one year results. Graefes Arch Clin Exp Ophthalmol. (2017) 255:1179–84. doi: 10.1007/s 00417-017-3645-628409225 · doi ↗ · pubmed ↗
- 4Jhanji V Young AL Mehta JS Sharma N Agarwal T Vajpayee RB. Management of corneal perforation. Surv Ophthalmol. (2011) 56:522–38. doi: 10.1016/j.survophthal.2011.06.003, PMID: 22117886 · doi ↗ · pubmed ↗
- 5Gain P Jullienne R He Z Aldossary M Acquart S Cognasse F. Global survey of corneal transplantation and eye banking. JAMA Ophthalmol. (2016) 134:167–73. doi: 10.1001/jamaophthalmol.2015.4776, PMID: 26633035 · doi ↗ · pubmed ↗
- 6Wolf EJ Kleiman LZ Schrier A. Nepafenac-associated corneal melt. J Cataract Refract Surg. (2007) 33:1974–5. doi: 10.1016/j.jcrs.2007.06.043, PMID: 17964407 · doi ↗ · pubmed ↗
- 7Wajnsztajn D Nche E Solomon A. Corneal complications of rheumatoid arthritis. Curr Opin Allergy Clin Immunol. (2022) 22:304–13. doi: 10.1097/ACI.0000000000000844, PMID: 35980013 · doi ↗ · pubmed ↗
- 8Shah R Amador C Tormanen K Ghiam S Saghizadeh M Arumugaswami V. Systemic diseases and the cornea. Exp Eye Res. (2021) 204:108455. doi: 10.1016/j.exer.2021.108455, PMID: 33485845 PMC 7946758 · doi ↗ · pubmed ↗