Rapid Progression of a CT-Defined Vulnerable Coronary Plaque: A Multimodality Imaging Case Report
B. S. H. Hagen, P. A. Diemen, M. J. Bom, S. P. Schumacher, A. C. van Rossum, A. Nap, M. P. Opolski, C. J. W. Verouden, I. Danad, P. Knaapen

TL;DR
This case report shows how a dangerous coronary plaque quickly worsened using CT and angiography.
Contribution
The study demonstrates rapid plaque progression using multimodal imaging in a single patient.
Findings
Intraplaque neovascularization and hemorrhage were observed in a rapidly progressive plaque.
Multimodal imaging confirmed the vulnerability and progression of the coronary plaque.
Serial imaging techniques effectively tracked plaque changes over time.
Abstract
Rapid progression of vulnerable plaques due to intraplaque neovascularization and hemorrhage is deemed as an important process preceding plaque rupture leading to myocardial infarction. We present a patient with a rapidly progressive vulnerable plaque assessed by means of coronary computed tomography angiography and serial invasive coronary angiography.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
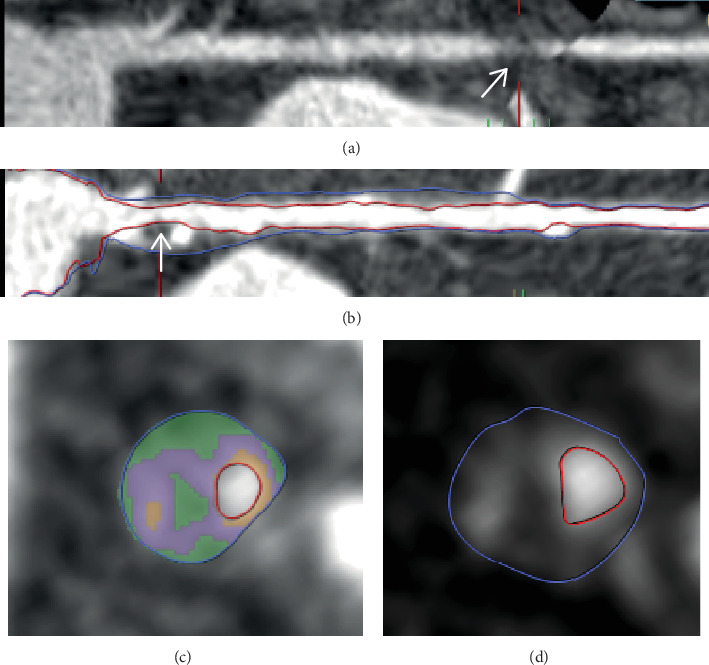 Figure 1
Figure 1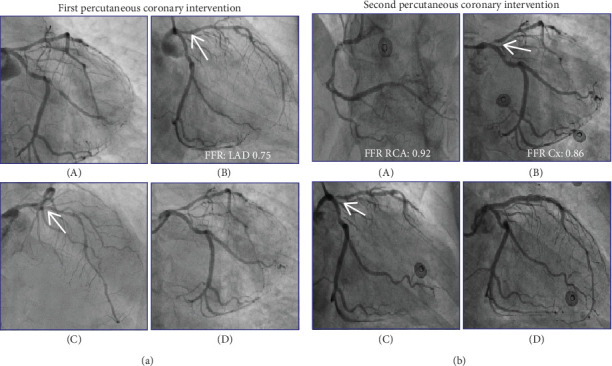 Figure 2
Figure 2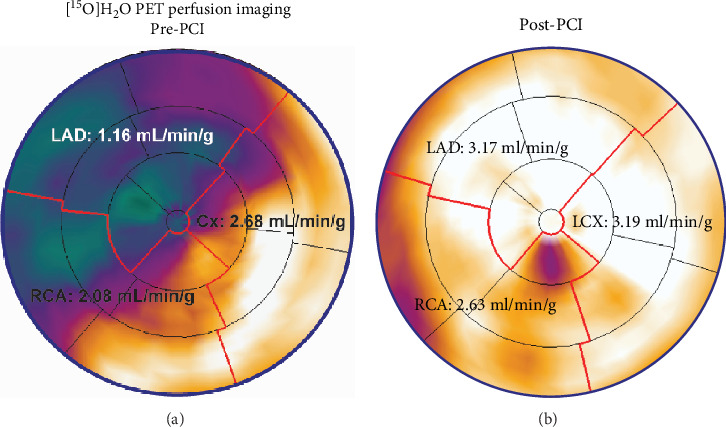 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCoronary Interventions and Diagnostics · Cardiac Imaging and Diagnostics · Aortic Thrombus and Embolism
Summary
- • It is important to be aware of rapid plaque progression among patients with a CT-defined vulnerable plaque and progressive symptoms.
- • Ongoing trials may help expand our treatment options in patients with a vulnerable plaque, potentially preventing adverse clinical outcomes.
1. Introduction
The present case report involves a patient with rapid progression of a coronary computed tomography angiography (CCTA)–derived vulnerable plaque leading to debilitating symptoms. This case report demonstrates one of the pathophysiological mechanisms underlying rapidly progressive angina pectoris.
2. Case Report
2.1. First Presentation
2.1.1. History of Presentation
An 80-year-old male, with a family history of cardiovascular events, presented at the outpatient clinic with new-onset exercise-induced angina pectoris and dyspnea for 3 months. His physical examination was unremarkable. The cardiovascular risk factors and medication at the initial presentation are presented in Table 1.
2.1.2. Past Medical History
Three years prior to presentation: Presentation at the emergency department with paroxysmal regular narrow complex tachycardia, with the following differential diagnoses: atrioventricular nodal reentrant tachycardia (AVNRT), atrioventricular reentrant tachycardia (AVRT), or atrial tachycardia.
One year prior to presentation: Echocardiography: normal left and right ventricular function and dimensions, normal atria, mild aortic valve insufficiency, and no significant valvular abnormalities.
2.1.3. Working Diagnosis
The diagnosis was angina pectoris due to obstructive coronary artery disease (CAD).
2.1.4. Investigations
The patient's resting electrocardiogram (ECG) was normal and he subsequently underwent CCTA. The right coronary artery (RCA) had mild irregularities. Regarding the left coronary system, the obtuse marginal (OM) had an obstructive noncalcified plaque that led to significant lumen narrowing (Figure 1a). Furthermore, the proximal left anterior descending artery (LAD) harbored a plaque of moderate severity (Figures 1b, 1c, and 1d). In-depth analysis of this proximal LAD plaque demonstrated an area of low attenuation, defined by < 30 Hounsfield units, indicative of a lipid core within the plaque. Furthermore, the region with high attenuation indicated the presence of fibrous tissue and spotty calcification. Lastly, the plaque demonstrated outward remodeling. Considering these plaque characteristics, the lesion was deemed a vulnerable plaque [1].
2.1.5. Management
The patient was prescribed an aspirin, a short- and long-acting working nitrate, a β-blocker, and a statin (Table 2). One month after CCTA, the patient underwent an invasive coronary angiography (ICA) that revealed a subtotal occlusion of the OM (Figure 2a (A)). The LAD was diffusely diseased and had a proximal stenosis of approximately 50% (Figure 2a (B,C)). Functional interrogation of the LAD revealed a gray-zone fractional flow reserve (FFR) of 0.75. An instantaneous wave-free ratio (iFR) pullback demonstrated a gradual decline in values from the ostium to the midsegment of the proximal LAD, without any distinct focal step-up. After careful consideration, the operator decided to defer percutaneous coronary intervention (PCI) of the LAD given the diffuse disease and subtotal occlusion of the OM which was deemed a likely cause of the patient's symptoms. Subsequently, a PCI of the OM was performed (Figure 2a (D)). Due to the tortuous anatomy of the target vessel, careful manipulation of the equipment was required. A drug-eluting stent (DES) with a diameter of 2.75 mm was deployed in the mid-OM segment with an excellent angiographic outcome, with good stent apposition and preserved flow. The LAD was treated conservatively given the diffuse disease and gray-zone FFR. After PCI, clopidogrel 75 mg once daily was prescribed for 1 year.
2.1.6. Follow-Up
Following PCI, the patient remained symptom-free and underwent an exercise stress test, which showed no signs of ischemia.
2.2. Second Presentation
2.2.1. History of Presentation
The patient had been free of symptoms for 1 month, after which exercise-induced angina (similar to the first presentation) reoccurred. Over the following months, symptoms progressively worsened, occurred at lower levels of exertion, and lasted longer before resolving.
2.2.2. Working Diagnosis
Diagnosis was progressive angina pectoris due to obstructive CAD.
2.2.3. Investigations
The patient underwent quantitative [^15^O]H_2_O positron emission tomography (PET) perfusion imaging to assess presence and location of ischemia (Figure 3a). A large perfusion defect in the LAD territory with a hyperemic myocardial blood flow of 1.16 mL/min/g (below the ischemic threshold of 2.3 mL/min/g) was observed [2]. At the time of the second presentation, C-reactive protein (CRP) was 2 mg/L, compared to 5 mg/L during the initial presentation.
2.2.4. Management
The patient was referred for ICA. The RCA and circumflex artery (Cx) had stenosis of intermediate severity that was functionally nonsignificant (FFR: 0.92 and 0.86, respectively) (Figure 2b (A,B)). Notably, the vulnerable plaque of the proximal LAD had progressed to a subtotal stenosis (Figure 2b (B,C)), for which a PCI was subsequently performed (Figure 2b (D)). Direct stenting was carried out using two DESs of 3.0 and 3.5-mm diameter, covering the lesion from the midsegment of the LAD to the ostial left main (LM). To ensure optimal stent expansion in the larger diameter of the LM, a proximal optimization technique (POT) was applied using a 5.0-mm noncompliant balloon inflated to 16 atm. The procedure resulted in an excellent angiographic outcome, with good stent apposition and preserved flow in both the diagonal (D) branch and the Cx (Figure 2b (D)). There was an interval of 4 months between the initial PCI and the second PCI.
2.2.5. Follow-Up
After his second PCI, the patient was free of symptoms. A follow-up [^15^O]H_2_O PET scan performed 2 months later revealed normalization of perfusion (Figure 3b). No follow-up lipid profile was obtained after the second PCI.
3. Discussion
This report underscores the pathophysiological mechanisms underlying rapid coronary plaque progression and illustrates how multimodality imaging can aid in the detection and characterization of vulnerable plaques. A coronary plaque that is prone to cause an acute thrombotic event leading to myocardial infarction (MI) is considered “vulnerable” [3]. These vulnerable plaques are thought to rapidly progress in size prior to rupturing [3]. The present case demonstrates rapid progression of conservatively treated CCTA-defined vulnerable plaque despite lipid-lowering medication. However, the subsequent reappearance of symptoms occurred swiftly, limiting a comprehensive assessment of the initiated medication regimen's effectiveness. The accelerated timeline between interventions may have influenced observed outcomes, posing a challenge in fully discerning the medical treatment's impact on vulnerable plaque progression. In addition, potential traumatic influence on the LAD ostial plaque during the initial intervention was considered. However, it is crucial to note the absence of procedural complications, such as dissections or hematomas, indicating minimal trauma. The plaque's stability postintervention, demonstrated by a symptom-free period and a normal stress test result, suggests immediate destabilization was not induced. However, the subsequent recurrence of anginal symptoms within 1 month, followed by gradual worsening, suggests progressive plaque destabilization rather than an acute thrombotic event. This delayed onset of symptoms may be explained by positive vascular remodeling, where the plaque initially expands outward, maintaining luminal patency before eventually encroaching on the vessel lumen as the disease progresses [3]. This progression of clinical symptoms, with worsening over a relatively short period, aligns with the spectrum of acute coronary syndrome (ACS) [4].
Inflammation plays a pivotal role in atherosclerosis [5]. Low-density lipoproteins are taken up by macrophages which become foam cells and when clustered together form lipid-rich necrotic cores [5]. Neovascularization of the necrotic core is an important contributor to rapid plaque progression. The newly formed vessels are fragile and prone to cause intraplaque hemorrhage [3]. Inflammatory mediators not only drive this angiogenic process but also promote vascular permeability, facilitating the infiltration of immune cells and accelerating plaque destabilization. Furthermore, silent plaque rupture and subsequent healing possibly play an additional role in rapid plaque progression [6].
Patients with vulnerable plaques are at an elevated risk of subsequent MI [3, 7]. However, current guidelines do not recommend pre-emptive stenting of functionally irrelevant vulnerable plaques nor serial testing for assessment of vulnerable plaque progression. This seems justified, as most patients with a vulnerable plaque will not suffer an acute thrombotic event [8].
Nonetheless, the search for optimal treatment of nonflow-limiting vulnerable plaques is ongoing. Recently, the PROSPECT II trial [9] demonstrated that nonculprit vulnerable plaques are prone to cause future events. The PROSPECT ABSORB study [10] was embedded within the PROSPECT II trial and randomized 182 patients with nonflow-limiting vulnerable plaques to treatment with a bioresorbable vascular scaffold (BVS) or optimal medical therapy. Prophylactic treatment by BVS implantation was safe and significantly enlarged the coronary lumen compared to a conservative strategy [10]. The trial was, however, not powered to assess clinical outcomes. The recently published PREVENT trial [11] provided more definitive insights. In this multicenter, open-label, randomized controlled trial, 1606 patients with nonflow-limiting vulnerable plaques were assigned to PCI plus optimal medical therapy or optimal medical therapy alone. At 2 years, the primary outcome—composite of cardiac death, target vessel MI, target vessel revascularization, or unplanned hospitalization for angina—occurred in 0.4% of the PCI group compared to 3.4% of the medical therapy group (p = 0.0003), demonstrating a significant reduction in major adverse cardiac events with PCI [11]. This trial underscores the potential benefit of PCI in reducing adverse cardiac events in patients with nonflow-limiting vulnerable plaques. So, while most vulnerable plaques do not lead to acute thrombotic events, certain high-risk plaques may warrant closer monitoring or even pre-emptive intervention. The characteristics of the plaque in this case meet all three criteria of a vulnerable plaque (Figure 1), namely, low attenuation, positive remodeling, and the ring-like sign [12]. A more refined risk stratification could help determine which plaques may benefit from pre-emptive stenting. CCTA can play a crucial role in risk stratification by identifying which plaques may benefit from pre-emptive stenting and which can be managed conservatively [13].
However, emerging local therapies such as drug-coated balloons may offer a novel approach to stabilizing high-risk plaques without leaving a permanent implant. The DEBuT-LRP study [14] demonstrated that pre-emptive treatment of nonflow-limiting lipid-rich plaques with a paclitaxel-coated balloon was safe and led to a significant reduction in lipid burden at 9-month follow-up, suggesting a potential role in selected patients.
Besides invasive treatment, novel medical treatments might prevent events in patients with a vulnerable plaque. The LoDoCO2 trial [15] demonstrated that an anti-inflammatory treatment in patients with chronic CAD led to a significant reduction of events compared to placebo. Furthermore, Budoff et al. [16] showed icosapent ethyl treatment to significantly reduce low-attenuation plaque volume compared to placebo. Although speculative, these types of treatments might be more beneficial among patients with vulnerable plaques by facilitating plaque stabilization and thereby possibly preventing rapid plaque progression.
3.1. Conclusion
CCTA-derived vulnerable plaques without significant lumen narrowing might progress in a relatively short period of time into flow-limiting stenoses with critical lumen narrowing.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bom M. J. van der Heijden D. J. Kedhi E. Early Detection and Treatment of the Vulnerable Coronary Plaque Circulation. Cardiovascular Imaging 201710510.1161/CIRCIMAGING.116.0059732-s 2.0-8501938924128483945 · doi ↗ · pubmed ↗
- 2Danad I. Uusitalo V. Kero T. Quantitative Assessment of Myocardial Perfusion in the Detection of Significant Coronary Artery Disease Journal of the American College of Cardiology 201464141464147510.1016/j.jacc.2014.05.0692-s 2.0-8490812058425277618 · doi ↗ · pubmed ↗
- 3Lu G. Ye W. Ou J. Coronary Computed Tomography Angiography Assessment of High-Risk Plaques in Predicting Acute Coronary Syndrome Frontiers in Cardiovascular Medicine 20218874353810.3389/fcvm.2021.743538 PMC 851713434660742 · doi ↗ · pubmed ↗
- 4ESC Scientific Document Group 2023 ESC Guidelines for the Management of Acute Coronary Syndromes European Heart Journal 202344383720382610.1093/eurheartj/ehad 19137622654 · doi ↗ · pubmed ↗
- 5Bäck M. Yurdagul A.Jr. Tabas I. Öörni K. Kovanen P. T. Inflammation and Its Resolution in Atherosclerosis: Mediators and Therapeutic Opportunities Nature Reviews. Cardiology 201916838940610.1038/s 41569-019-0169-22-s 2.0-8506264159730846875 PMC 6727648 · doi ↗ · pubmed ↗
- 6Araki M. Yonetsu T. Kurihara O. Predictors of Rapid Plaque Progression: An Optical Coherence Tomography Study JACC: Cardiovascular Imaging 20201481628163810.1016/j.jcmg.2020.08.01433011121 · doi ↗ · pubmed ↗
- 7Mol J. Q. Volleberg R. H. J. A. Belkacemi A. Fractional Flow Reserve-Negative High-Risk Plaques and Clinical Outcomes After Myocardial Infarction JAMA Cardiology 2023811 e 23291010.1001/jamacardio.2023.291037703036 PMC 10500430 · doi ↗ · pubmed ↗
- 8Arbab-Zadeh A. Fuster V. From Detecting the Vulnerable Plaque to Managing the Vulnerable Patient: JACC State-of-the-Art Review Journal of the American College of Cardiology 201974121582159310.1016/j.jacc.2019.07.0622-s 2.0-8507202564031537269 · doi ↗ · pubmed ↗