Solitary Testicular Metastasis From Prostate Cancer Treated With Orchiectomy: A Rare Case of Isolated Recurrence After Salvage Radiotherapy
Moritz Gutjahr-Holland, Shreya Armstrong

TL;DR
A rare case of prostate cancer spreading to one testicle was successfully treated with surgery after radiation therapy.
Contribution
This case report highlights a rare metastasis pattern and treatment response in prostate cancer.
Findings
Prostate cancer metastasized to a single testicle after salvage radiation therapy.
Orchiectomy led to a rapid decrease in PSA levels in the patient.
Abstract
Prostate cancer (PCa) is the most commonly diagnosed cancer in Australia with almost 25,000 cases being diagnosed each year. Treatment for PCa varies depending on stage, patient preferences and the general health of the patient. PCa most commonly spreads to lymph nodes and bones. We present a case of a 66-year-old male who presented with PSA elevation post salvage radiation and was diagnosed with oligometastatic PCa to the right testis. This patient subsequently underwent a right orchidectomy resulting in a rapid fall in PSA.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
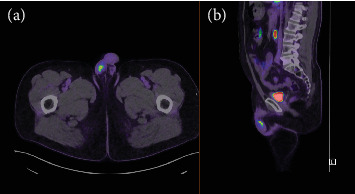 Figure 1
Figure 1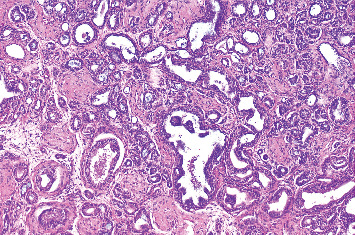 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTesticular diseases and treatments · Prostate Cancer Treatment and Research · Genital Health and Disease
1. Introduction
In Australia, prostate cancer is the most commonly diagnosed cancer [1] and is the cause of death of approximately 3700 men every year [2]. Risk factors for prostate cancer include advancing age; a positive family history; certain inherited genetic variants such as BRCA1/2, CHEK2 and HOXB13 [3] and ethnicity. Prostate cancer can be localised or metastatic at diagnosis. Approximately 10% of patients have metastatic prostate cancer at diagnosis [4] with the most common metastases found in the bones, lymph nodes, liver and lungs. Rarely does prostate cancer metastasise to the testis [5]. Rarer still do testicular metastases from prostate cancer occur in an oligometastatic fashion. We present a case of an elderly male who was diagnosed with oligometastatic prostate cancer to the right testis after salvage radiotherapy and subsequently underwent a right orchidectomy. Informed consent was obtained from the patient for publication of this case report.
2. Case Presentation
A 66-year-old male with a history of treated prostate cancer was being followed up in the radiation oncology outpatients clinic. He had been first diagnosed with prostate cancer in 2020 after presenting with lower urinary tract symptoms (LUTSs). An elevated PSA to 5.6 μg/L was identified, and the patient underwent a PSMA PET at the time, which demonstrated intense PSMA activity in the left peripheral zone of the prostate from base to mid gland, and a separate moderately PSMA avid focus in the right mid zone of the prostate. The patient proceeded to a laparoscopic prostatectomy in early 2021. Intraoperative findings demonstrated a large left posterior cancer. Histopathology demonstrated a Gleason 3 + 4 = 7 prostate cancer with a tumour volume of 9.05 cm^3^. There was lymphovascular invasion present, intraductal carcinoma present and established extra prostatic extension. The surgical margins were involved. There was carcinomatous involvement of the left and right neurovascular bundles and bilaterally extensive involvement of the seminal vesicles. Postoperatively, the PSA fell to 0.28 at 6 weeks but began climbing to 0.35 μg/L (24/6/2021) at 3 months, giving an estimated PSA doubling time of approximately 5 months. A repeat PSMA PET was undertaken in July 2021, which demonstrated no abnormal PSMA uptake. After ongoing PSA rise to 0.5 μg/L (14/10/2021) the patient commenced salvage radiation in late 2021 (64Gy in 32#) with 6 months of androgen deprivation therapy (ADT). PSA was suppressed on ADT with a nadir of 0.01 μg/L.
Unfortunately, in early 2023, this patient's PSA began to rise and reached 0.77 μg/L (19/1/2024). A further PSMA PET was performed which demonstrated a single hotspot in the right testis (Figure 1). Consistent with this, a clinical examination demonstrated a tender and swollen right testis. His case was discussed at a multidisciplinary team with a recommendation for a referral for consideration of orchidectomy. The patient underwent a right radical orchiectomy on 12/02/2024. The operation was completed without complication and the patient was discharged from hospital the day of surgery. Histopathology of the orchiectomy specimen demonstrated nodules of metastatic prostatic adenocarcinoma in the right testis (Figure 2) with lymphovascular invasion. The tumour was graded as Gleason 4 + 3 = 7. This was excised clear of margins. Postoperatively, PSA fell to 0.19 μg/L on 26/02/2024 and further to 0.12 μg/L on 11/4/2024, approximately 2.5 months after surgery. Subsequently, the PSA demonstrates an upwards trend to 0.29 μg/L (31/03/25) and most recently to 0.38 μg/L (08/07/25). The patient is well and continues on regular 3 monthly PSA surveillance with a plan to repeat PSMA PET imaging if the PSA reaches 0.5 μg/L.
3. Discussion
It is well known that prostate cancer typically metastasises to bones, lymph nodes, liver and lungs [6]. However, metastatic disease to the testis is rare. The earliest published report of secondary metastasis to the testicle from another primary site was described by Semans in 1938 [7]. Large autopsy reviews have since confirmed its rarity; one study of 24,000 autopsies demonstrated only 15 cases of testicular metastases with an incidence of 0.06% [8]. The primary sources of testicular secondaries are the prostate, colon, kidney, stomach, pancreas and melanoma [9]. Reports of oligometastatic prostate cancer to the testis in the literature are limited to case reports, the first of which was published in 1984 [10]. Testicular metastases have been associated with a poor prognosis; a Taiwanese series of seven cases demonstrated survival around 12 months [11]. Possible pathways of spread of PCa to the testis have been speculated to include haematogenous spread, including arterial embolism, lymphatic spread or endocanalicular spread [12]. Patients with secondaries in the testis may present with a testicular mass, testicular swelling or testicular pain [13] but may also be asymptomatic [12]. However, it is important to keep in mind that in younger men, the main oncological differential for a testicular mass would be primary testicular cancer, as it is the most common tumour in the 15–34 year age group [14]. The most common testicular cancer is a germ cell tumour.
Although the precise route of spread in our patient cannot be confirmed, it is worth considering whether the prior laparoscopic prostatectomy might have played a role. Surgical manipulation, particularly when the neurovascular bundles and seminal vesicles are extensively involved by tumour, could theoretically facilitate the dissemination of malignant cells. Mechanisms could include tumour cell spillage into lymphatic, vascular or endocanalicular channels (vas deferens) during the dissection, or microscopic seeding along surgical pathways. However, such events remain highly speculative and there is currently no direct evidence linking laparoscopic radical prostatectomy to testicular metastases. In this context, it is the opinion of the authors that the most likely route of metastasis is via haematogenous spread.
Prostate cancer is highly survivable, with a survival rate of 95% at 5 years [2]. However, the presence of metastasis reduces this significantly. According to data from the American Cancer Society, metastatic prostate cancer carries a 34% 5-year survival. Despite this, metastatic prostate cancer has a number of treatment options. These include watchful waiting, radiation therapy, hormone therapy, chemotherapy and radioisotope therapy. As the next paragraph will discuss, treatments for metastatic prostate cancer have improved in recent years. Thus, men being diagnosed with prostate cancer currently could be expected to have a better survival than the aforementioned numbers would indicate.
Patients with metastatic cancer that is confined to a limited number of sites (oligometastasis), such as our patient, may have the unique opportunity of metastasis-directed therapy (MDT). The theory behind MDT is to eliminate the limited metastatic disease before the tumour cells can select for aggressive clonagens that have the ability and propensity to metastasise to further distant sites [15]. In selected patients, the MDT approach can potentially be curable. The optimal treatment approach for MDT is debated and includes ablative radiotherapy (SABR/SBRT), metastatectomy (as occurred here), radioligand therapy and observation. Evidence supporting MDT includes the phase II ORIOLE trial, which randomised 54 men to either SBRT or observation. Treated patients had significantly lower rates of disease progression compared with controls (61% vs. 19%) [16]. The benefit, however, relies heavily on accurate detection of all metastatic sites. The presence of even a single untreated metastasis was associated with worse median distant metastasis-free survival (6 months vs. 29 months) [16]. Further evidence for the durability of MDT is provided by a retrospective study by Milenkovic et al. of 211 patients with oligorecurrent PCa after radical prostatectomy, whereupon delivery of MDT, 23% of patients in this study remained free of a second recurrence at 5 years [17]
Fortunately, modern molecular imaging techniques such as PSMA-PET have significantly improved the detection of metastasis with high sensitivity and specificity [18]. This imaging technique was used in our patient to detect the solitary testicular metastasis. The main weakness of this technique is the sensitivity, with studies reporting 75%–85% sensitivity [18, 19].
Another benefit of MDT is that it may enable men to avoid or delay the use of ADT [16, 17, 20, 21]. ADT carries a broad side effect profile, particularly in younger men, and carries long-term adverse health effects including reduction in bone density, decrease in muscle mass and weight gain which may predispose to metabolic syndrome. Many patients would be interested in avoiding these side effects. The main limitation of the MDT approach would be the potential for acute toxicities from the local therapy. Fortunately, unilateral orchiectomy is generally well tolerated, and indeed, our patient was discharged home the day of surgery.
4. Conclusion
Metastatic prostate cancer to the testis is a rare diagnosis, especially so when it occurs in an isolated and oligometastatic fashion. Despite this, in oncological patients with testicular masses or pain, the possibility of testicular secondaries must be considered. The pathways for this form of metastatic spread remain uncertain. Our patient underwent a unilateral orchidectomy with rapid response in serum PSA. This is a pleasing result, and it is hoped that this will prevent progression of metastatic disease and may also allow our patient to delay the introduction of ADT. Our patient is undergoing ongoing PSA surveillance to assess if further treatments or investigations are required.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Cancer in Australia Statistics Cancer Australia [cited 2024 Apr 12]. Available from: https://www.canceraustralia.gov.au/impacted-cancer/what-cancer/cancer-australia-statistics
- 2PCFA Prostate Cancer a Guide for Newly-Diagnosed Men 2023[cited 2024 Apr 12]. Available from: https://www.pcfa.org.au/media/u 2kmu 0wv/pcf 13457-prostate-cancer-a-guide-for-newly-diagnosed-men-56-pg-booklet_9-pdf.pdf
- 3Raghallaigh H. N. Bott S. R. Barber N. Ali A. The Role of Family History and Germline Genetics in Prostate Cancer Disease Profile and Screening Urologic Cancers [Internet] 2022 Brisbane (AU)Exon Publications[cited 2025 Aug 10]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK 585972/36343130 · pubmed ↗
- 4Juan G. R. Laura F. H. Javier P. V. Where Do We Stand in the Management of Oligometastatic Prostate Cancer? A Comprehensive Review Cancers 2022148 p. 201710.3390/cancers 1408201735454924 PMC 9029666 · doi ↗ · pubmed ↗
- 5Ahmed S. A. Nawaz M. M. Masood Y. Maqbool H. Mir K. Metastatic Prostate Tumor to Testes: Sign of Advance Disease Urology Case Reports 20235010241010.1016/j.eucr.2023.102410 PMC 1032051737416751 · doi ↗ · pubmed ↗
- 6Gandaglia G. Abdollah F. Schiffmann J. Distribution of Metastatic Sites in Patients With Prostate Cancer: A Population-Based Analysis Prostate 201474221021610.1002/pros.227422-s 2.0-8489115660324132735 · doi ↗ · pubmed ↗
- 7Semans J. H. Carcinoma of the Prostate With Metastasis in the Testis Journal of Urology 193840452452910.1016/S 0022-5347(17)71794-6 · doi ↗
- 8Pienkos E. J. Jablokow V. R. Secondary Testicular Tumors Cancer 197230248148510.1002/1097-0142(197208)30:2<481::AID-CNCR 2820300228>3.0.CO;2-X 5051673 · doi ↗ · pubmed ↗