First Described Case of Infective Endocarditis Involving the Pulmonary Valve Caused by Moraxella catarrhalis
P. Karamani, E. Christopoulou, A. Negash, C. Charalambous, G. M. Georgiou, I. Tzanavaros, G. Miltiadous

TL;DR
A rare case of infective endocarditis caused by Moraxella catarrhalis at the pulmonary valve is described, highlighting diagnostic challenges and the role of cardiac CT.
Contribution
First described case of M. catarrhalis causing prosthetic pulmonary valve infective endocarditis.
Findings
M. catarrhalis can cause prosthetic pulmonary valve infective endocarditis.
Cardiac CT is essential for diagnosing IE when TOE results are negative.
Right-sided IE may be missed by TOE, especially with prosthetic valves.
Abstract
Moraxella catarrhalis, once considered a component of the normal human flora of the upper respiratory tract, is now recognized as a true pathogen and, rarely, a cause of infective endocarditis (IE). We describe a rare case of a 36-year-old woman who presented with respiratory symptoms and was initially misdiagnosed with pneumonia and M. catarrhalis bacteremia. No vegetations were seen on transesophageal echocardiogram (TOE) imaging. However, further investigation with cardiac computed tomography (CT) revealed prosthetic pulmonary valve IE caused by M. catarrhalis, which also resulted in pulmonary abscesses. This case highlights the importance of considering M. catarrhalis as a true pathogen in invasive disease, including prosthetic pulmonary valve IE. It also demonstrates the limitations of negative TOE findings in the evaluation of right-sided IE, particularly when prosthetic valves…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
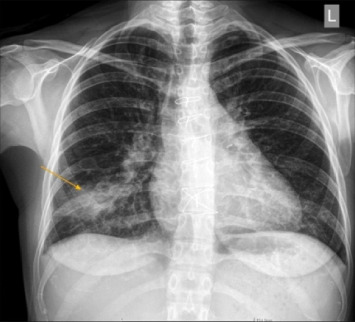 Figure 1
Figure 1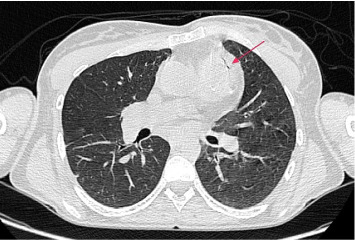 Figure 2
Figure 2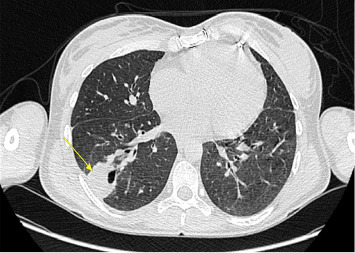 Figure 3
Figure 3 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfective Endocarditis Diagnosis and Management · Cardiac Valve Diseases and Treatments · Antimicrobial Resistance in Staphylococcus
Summary
- • Moraxella catarrhalis can cause prosthetic pulmonary valve infective endocarditis (IE).
- • Pulmonary valve endocarditis is rare and may present atypically with recurrent respiratory symptoms.
- • TOE has limitations in detecting prosthetic pulmonary valve endocarditis and its complications.
- • Cardiac computed tomography (CT) is an essential complementary diagnostic tool in these cases.
1. Introduction
Moraxella catarrhalis is a Gram-negativediplococcus belonging to the family Moraxellaceae. It is an exclusively human commensal and mucosal pathogen. Colonization of infants by M. catarrhalis is common, with rates approaching 100%, and is associated with otitis media. In contrast, only up to 5% of adults are colonized, though colonization rates are higher among individuals with chronic obstructive pulmonary disease (COPD) or other underlying respiratory conditions.
Clinically, M. catarrhalis most commonly causes lower respiratory tract infections in patients with COPD, pneumonia in older adults, sinusitis, and, more rarely, bacteremia, osteomyelitis, and infective endocarditis (IE) [1, 2].
A systematic review by Ioannou et al. described 31 reported cases of IE caused by Moraxella species, comprising 25 case reports and 2 case series. The mitral valve was the most commonly affected site. A prosthetic cardiac valve was present in 25.8% (8 of 31) of the patients [3]. Since that review, two additional cases have been published [4, 5]. Notably, no previous cases of pulmonary valve IE caused by Moraxella species have been reported.
Pulmonary valve IE is rare, accounting for only 1.5%–2% of all IE cases, with isolated pulmonary valve involvement being even less common. Risk factors include intravenous drug use, congenital heart disease, healthcare-associated invasive procedures, and, occasionally, immunosuppression [6].
Here, we report the first case of prosthetic pulmonary valve IE caused by M. catarrhalis, presenting primarily with recurrent respiratory infections due to septic pulmonary emboli.
2. Case Report
A 36-year-old woman, a former smoker, presented to the emergency department with fever, chills, and a productive cough that had persisted for three months. She had a history of Tetralogy of Fallot and had undergone pulmonary valve and root pulmonary artery replacement twice—first in infancy and again 5 years prior.
Following her most recent surgery, she experienced recurrent episodes of fever and chills over 4 years, sometimes self-resolving and sometimes requiring antibiotic therapy.
One month before admission, she had been hospitalized with right lower lobe pneumonia and M. catarrhalis bacteremia. She was treated with intravenous cefuroxime for 20 days, resulting in normalization of inflammatory markers. A transesophageal echocardiogram (TOE) performed at that time revealed no vegetations or perivalvular abscesses.
Upon the current presentation, her vital signs were as follows: temperature 38.6°C, heart rate 115 bpm, blood pressure 136/82 mmHg, respiratory rate 22 breaths/min, and oxygen saturation 96% on room air. Cardiovascular examination revealed a systolic murmur over the pulmonary valve area. Crackles were auscultated in the right lower lung zone. Chest x-ray showed right lower lobe consolidation (Figure 1).
Laboratory tests demonstrated the following:
-
- Microcytic hypochromic anemia: hemoglobin 9.8 g/dL, mean corpuscular volume 72 fL, and mean corpuscular hemoglobin 23 pg/cell
-
- Elevated white blood cell count: 13,430 cells/mm^3^
-
- Elevated C-reactive protein: 209 mg/L
-
- Elevated erythrocyte sedimentation rate (ESR): 48 mm/hr
-
- Elevated rheumatoid factor: 279 U/mL
Given the high suspicion of IE, a repeat TOE was performed but again showed no vegetations or other abnormalities. Subsequent cardiac computed tomography (CT) revealed a perivalvular abscess (Figure 2), while chest CT identified two pulmonary abscesses consistent with septic emboli (Figure 3).
Blood cultures obtained on admission later grew Gram-negative diplococci, identified as M. catarrhalis using Matrix-Assisted Laser Desorption/Ionization Time-of-Flight (MALDI-TOF) testing.
The diagnosis of prosthetic valve IE was confirmed using the 2023 modified Duke criteria based on the following [7]:
- • One major criterion: imaging evidence of IE (perivalvular abscess on cardiac CT)
- • Four minor criteria: predisposing condition (prosthetic pulmonary valve), fever > 38°C, pulmonary abscesses, positive rheumatoid factor, and positive blood cultures that do not meet as a major criterion.
The patient was started on intravenous meropenem and gentamycin. After 2 weeks of therapy, she underwent repeat pulmonary valve and root pulmonary artery replacement (Figure 4). Cultures of excised valve tissue were negative.
A follow-up chest CT showed significant improvement in the pulmonary abscesses. Based on microbiological findings, moxifloxacin was continued until normalization of inflammatory markers and resolution of radiographic abnormalities.
3. Discussion
This is the first reported case of prosthetic pulmonary valve IE caused by M. catarrhalis. The patient's recurrent episodes of pneumonia were, in retrospect, caused by septic pulmonary emboli originating from right-sided IE. Septic emboli are a common complication of right-sided IE, occurring in up to 82% of the cases [8]. As a result, Bamford et al. suggested that clinicians should consider chest CT routinely as part of right-sided IE follow-up [9]. Indeed, repeated CT chest in our patient had showed resolution of lung abscesses in full accordance with the normalization of the inflammatory blood parameters.
Beta-lactam antibiotics are known as first-line empirical therapy for M. Catarrhalis infections, including IE [10]. In our patient, initial treatment with beta and third-generation cephalosporins likely controlled the pneumonia episodes but was insufficient for eradication of IE, as treatment durations were inadequate for endocarditis. This explains the recurrence of septic emboli and persistent pulmonary complications. The cultures of excised valve tissue were negative likely due to prior 2 weeks of successful antibiotic treatment.
Echocardiography is the first-line imaging modality for suspected IE. TOE is recommended when transthoracic echocardiogram (TTE) findings are inconclusive, especially in patients with prosthetic valves [11]. However, TOE is less effective for evaluating the pulmonary valve due to its anatomical location and, in case of prosthetic valve, due to acoustic shadowing caused by prosthetic components [12].
Cardiac CT has proven superior to TOE in detecting perivalvular and periprosthetic complications such as abscesses, pseudoaneurysms, and fistulas. In one study of 115 patients with surgically confirmed IE, TOE missed 52% of perivalvular abscesses [13]. Cardiac CT and MRI are also increasingly used for detailed anatomical evaluation of pulmonary valves and surrounding structures [11].
In this case, the negative TOE results delayed diagnosis, whereas cardiac CT provided the definitive evidence needed to guide diagnosis, treatment, and surgical intervention.
4. Conclusions
This case underscores several critical points as follows:
- - Moraxella catarrhalis should be recognized as a true pathogen capable of causing invasive disease, including prosthetic pulmonary valve IE.
-
- Right-sided IE can present atypically with recurrent respiratory symptoms such as pneumonia.
-
- When TOE is negative but clinical suspicion remains high, cardiac CT should be performed to evaluate for prosthetic pulmonary valve involvement and associated complications.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Yao K. Liu D. Tang Y.-W. Hindiyeh M. Y. Liu D. Sails A. Spearman P. Zhang J.-R. Chapter 74-Moraxella catarrhalis Molecular Medical Microbiology 20243 rd Academic Press 1503151710.1016/B 978-0-12-818619-0.00057-5 · doi ↗
- 2Aebi C. Moraxella catarrhalis-Pathogen or Commensal? Advances in Experimental Medicine and Biology 201169710711610.1007/978-1-4419-7185-2_92-s 2.0-7995227766121120723 · doi ↗ · pubmed ↗
- 3Ioannou P. Alexakis K. Baliou S. Kofteridis D. P. Infective Endocarditis by Moraxella Species: A Systematic Review Journal of Clinical Medicine 2022117 p. 185410.3390/jcm 11071854 PMC 899971435407461 · doi ↗ · pubmed ↗
- 4Yoshitake S. Kusama Y. Shiomi F. First Pediatric Case of Endocarditis Caused by Moraxella Nonliquefaciens: Importance of Molecular Diagnosis The Pediatric Infectious Disease Journal 2024438 p. e 28910.1097/INF.000000000000433938534791 · doi ↗ · pubmed ↗
- 5Ardiana M. Mahmudah T. R. A. Herwanto B. Sufiyah I. M. Venous Thromboembolism, an Unusual Complication of Infective Endocarditis Caused by Moraxella Species: A Case Report Cor et Vasa 202466337037410.33678/cor.2024.009 · doi ↗
- 6Zhang M. X. Zhang W. M. Yu C. Isolated Pulmonary Valve Endocarditis With Rapid Progression: A Case Report and Literature Review Journal of Cardiothoracic Surgery 2021161 p. 1610.1186/s 13019-020-01375-w PMC 784188833509229 · doi ↗ · pubmed ↗
- 7Delgado V. Ajmone Marsan N. de Waha S. 2023 ESC Guidelines for the Management of Endocarditis European Heart Journal 202344393948404210.1093/eurheartj/ehad 19337622656 · doi ↗ · pubmed ↗
- 8Ye X. T. Buratto E. Dimitriou J. Right-Sided Infective Endocarditis: the Importance of Vegetation Size Heart Lung & Circulation 2021 May 30574175010.1016/j.hlc.2020.09.92733526363 · doi ↗ · pubmed ↗