A Case Report and Global Perspective on Fusarium Superficial Keratitis in the Pediatric Population
S Avinash, Rajesh Kanna Kannabiran, Rahul Garg, Pravalika Rebbala, Sree Ranjani S, Siddharam S Janti, Shalam Nikhat Sheerin, Rahul Narang

TL;DR
A 9-year-old boy developed Fusarium keratitis after eye trauma and steroid use, successfully treated with antifungal drugs.
Contribution
Highlights the importance of rapid diagnosis and treatment in pediatric Fusarium keratitis cases.
Findings
Fusarium solani was identified using mass spectrometry in a pediatric keratitis case.
Topical natamycin and voriconazole healed the infection without surgery.
Unsupervised corticosteroid use increases risk in endemic regions.
Abstract
Fungal keratitis is a major cause of corneal blindness in tropical regions, with Fusarium species predominating. Pediatric cases, though less common, carry a greater risk of amblyopia and long-term disability. We report a nine-year-old boy who developed Fusarium keratitis after minor ocular trauma and unsupervised corticosteroid use. Corneal scrapings showed septate hyphae, and identification confirmed Fusarium solani by matrix-assisted laser desorption/ionization time-of-flight mass spectrometry. Treatment with topical natamycin and voriconazole led to complete healing without surgery. This case highlights the need for early recognition, rapid microbiological confirmation, and appropriate antifungal therapy in pediatric fungal keratitis, while underscoring the dangers of unsupervised corticosteroid use in endemic regions.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
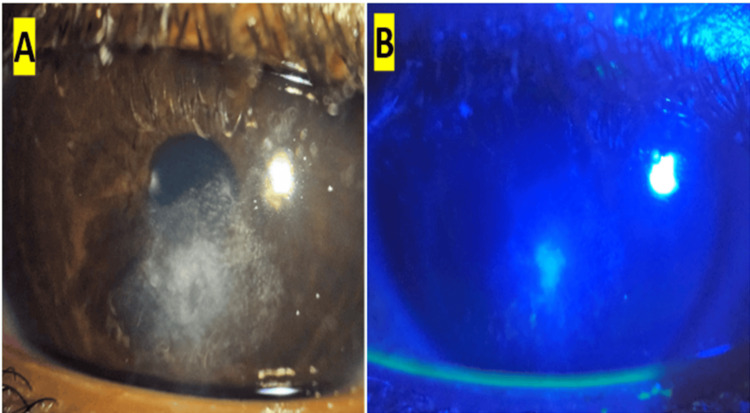 Figure 1
Figure 1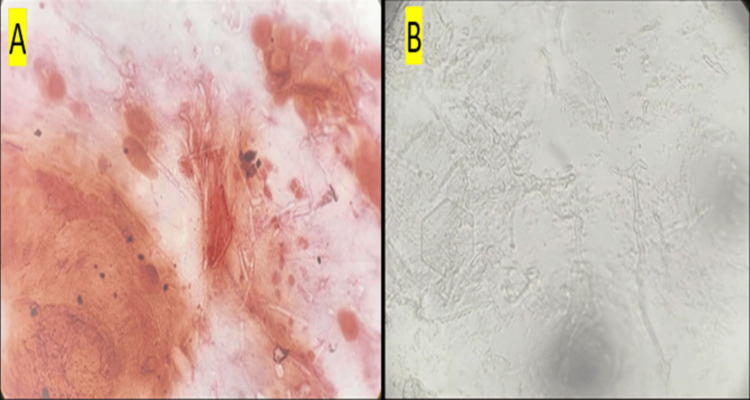 Figure 2
Figure 2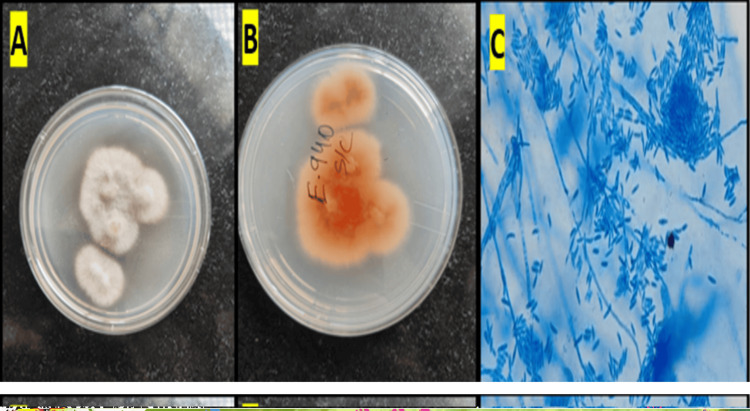 Figure 3
Figure 3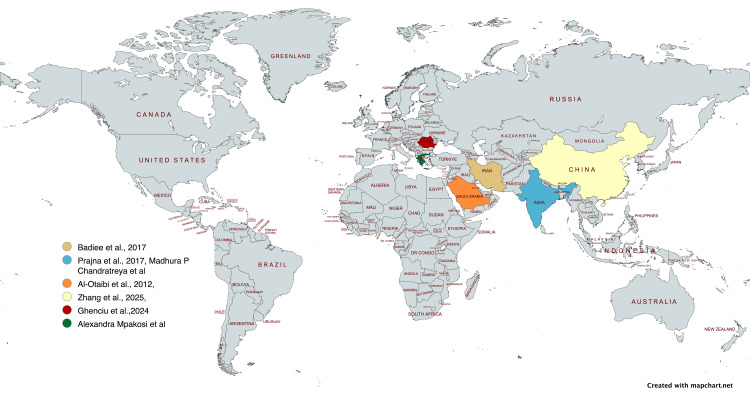 Figure 4
Figure 4| Study (region) | Year | Population | n (Fusarium) | Main risk factors | Diagnosis (molecular) | Monotherapy, n (%) | Dual Therapy (n, %) | Surgery (n, %) | Resolved on medical, n (%) | Main antifungals | Key outcomes |
| Al-Otaibi [ | 2012 | Pediatric | 34 | Trauma | Culture | Not specified | Not specified | 12 (35.3%) | 22 (64.7%) | Natamycin, voriconazole | Early diagnosis, intensive therapy, and surgery improve outcomes |
| Badiee et al. [ | 2017 | Pediatric | Review | Trauma | Culture | Not specified | Not specified | Not specified | Not specified | Natamycin, voriconazole | Early diagnosis and intensive therapy critical |
| Prajna et al. [ | 2017 | Pediatric | 234 (all pediatric keratitis) | Trauma | Culture | Not specified | Not specified | Not specified | Not specified | Natamycin | Fusarium is the most common fungus in children |
| Ghenciu et al. [ | 2024 | Mixed | Review | Trauma, CL use | Culture, molecular | Not specified | Not specified | Not specified | Not specified | Natamycin, voriconazole | Polyenes and azoles essential; molecular advances emerging |
| Zhang et al. [ | 2025 | Pediatric | 47 children (48 eyes) | Trauma (dust/vegetative) | Culture, PCR | 8/48 (16.7%) | Not specified | 32/48 (66.7%) (21 PK, 11 LKP) | 8/48 (16.7%) | Voriconazole, natamycin | Fusarium 41.7%; ulcer size predicts surgery; NLR predicts risk |
| Cintra et al. [ | 1969-2023 | Mixed | Review | Contact lens usage | Culture | Not specified | Not specified | Not specified | Not specified | Natamycin, voriconazole | Timely identification and early initiation of antifungal treatment |
| Mpakosi et al. [ | 16 years | Mixed | 35 fungal keratitis Fusarium species (n = 21, 61.8%) | Corneal injury by plant material and soft contact lens | Culture | Not specified | Not specified | Keratoplasty was required in 40% and enucleation in 8% | Antifungal therapy alone was 52% | Voriconazole, liposomal AmB | A large proportion of cases resulted in keratoplasty despite appropriate antifungal treatment |
| Chandratreya et al. [ | 18 months | Pediatric | 6.8% of eyes were culture positive, with bacterial isolates in 17.9% and fungi in 82.1%. Fusarium species (67.8%) | Trauma (unidentified foreign body) | Not specified | Polytherapy | Not specified | TPK was required for 2.6% of eyes | 87.80% | Natamycin and 0.5% moxifloxacin concurrently | Trauma was the leading predisposing factor for microbial keratitis |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOcular Infections and Treatments · Ocular Surface and Contact Lens · Intraocular Surgery and Lenses
Introduction
Fungal keratitis is a severe, vision-threatening corneal infection predominantly found in tropical and subtropical regions, where it accounts for up to 50% of corneal ulcers, particularly in South Asia and sub-Saharan Africa [1]. Among the causative pathogens, Fusarium spp. is recognized as one of the most virulent filamentous fungi associated with rapid progression and poor prognosis if not treated early [2]. While the clinical and microbiological characteristics of fungal keratitis in adults are well documented, pediatric presentations remain underreported and often underrecognized [3].
Children are susceptible to corneal infections due to their frequent exposure to environmental agents and a delay in reporting symptoms. Diagnosis is further complicated by nonspecific early signs, potential difficulty in patient cooperation during examination, and the tendency for delayed referral [4]. Moreover, the unsupervised use of over-the-counter corticosteroid eye drops can suppress immune responses and worsen fungal infections, making timely identification and appropriate therapy crucial [5].
Here, we report a rare pediatric case of Fusarium superficial keratitis with clinical features and rapid microbiological confirmation. The case was successfully treated with dual topical antifungal therapy. This report aims to contribute to the limited pediatric literature and reinforce the importance of early empirical management in suspected fungal keratitis.
Case presentation
A nine-year-old boy presented to the ophthalmology outpatient services in an tertiary care hospital with a two-day history of redness, ocular pain, photophobia, and blurring of vision in the left eye following minor trauma with a foreign body sustained during play. Before presentation, he had self-administered over-the-counter corticosteroid eye drops. There was no history of systemic or ocular comorbidities, and baseline viral markers were negative.
On examination, he was alert, afebrile, and systemically stable. Uncorrected visual acuity was 6/6 in the right eye and 6/12 in the left eye, improving with pinhole. Slit-lamp evaluation of the left eye revealed a central, dry corneal ulcer showing a 1-mm epithelial defect with surrounding stromal edema and peripheral scarring (Figure 1A). Fluorescein staining demonstrated a 1-mm epithelial defect (Figure 1B). Intraocular pressure and lens status were within normal limits. The posterior segment could not be visualized due to corneal opacity.
Slit‑lamp examination of the left eye(A) Slit‑lamp image showing a 1‑mm central epithelial defect with surrounding stromal edema and peripheral scarring. (B) Cobalt blue illumination with fluorescein staining highlighting the epithelial defect
Corneal scrapings were obtained under aseptic precautions and inoculated into 5% sheep blood agar and Sabouraud dextrose agar (SDA) plate along with direct microscopy for 10% potassium hydroxide (KOH) mount. A provisional diagnosis of fungal keratitis was made, and empirical therapy was initiated with natamycin 5% eye drops hourly, homatropine 2% thrice daily, and lubricants to relieve ciliary spasm and protect the ocular surface. The findings by direct microscopy are as follows: Gram staining revealed faintly stained filamentous structures (Figure 2A), and KOH mount showed abundant septate hyaline hyphae with branching (Figure 2B).
Direct microscopy of corneal scrapings(A) Gram stain showing faintly stained filamentous structures. (B) KOH mount demonstrating abundant septate, hyaline hyphae with branchingKOH: potassium hydroxide
Cultures on SDA and blood agar demonstrated white, fluffy colonies by day 3 (Figures 3A, 3B). A lactophenol cotton blue mount from the culture showed hyaline, septate hyphae with characteristic canoe-shaped macroconidia, confirming Fusarium species (Figure 3C) and later confirmed by matrix-assisted laser desorption/ionization time-of-flight mass spectrometry to be Fusarium solani.
Growth of Fusarium solani on SDA and microscopic morphology(A,B) White, fluffy colonies seen on SDA. (C) LPCB mount showing hyaline, septate hyphae with characteristic canoe‑shaped macroconidiaSDA: Sabouraud dextrose agar; LPCB: lactophenol cotton blue
Following microbiological confirmation, the treatment regimen was escalated to dual antifungal therapy with natamycin 5% and voriconazole 1% topical drops. By the third day of antifungal therapy, subjective improvement in vision and reduced discomfort were reported. Slit-lamp reevaluation showed resolution of hypopyon, reduction of stromal edema, and a decrease of the epithelial defect to about 1 mm, with fluorescein staining limited to the ulcer margins. Over the subsequent week, the ulcer demonstrated steady healing, with complete resolution of the epithelial defect and no evidence of stromal thinning, melting, or secondary infection.
At follow-up, corneal clarity had significantly improved, slit-lamp examination appeared normal, and the child's visual acuity had recovered to 6/6 bilaterally, with no surgical intervention required.
Discussion
Fungal keratitis is a major cause of corneal blindness worldwide, with a disproportionately high burden in tropical and subtropical regions. The estimated global incidence of infectious keratitis is 23.6 per 100,000 people annually, but this rises sharply in countries with hot, humid climates and agrarian risk factors, reaching 113 per 100,000/year in South India, 339 in Bhutan, 710 in Burma, and 799 in Nepal [6]. By contrast, developed countries such as the United States, England, and Australia report much lower rates, ranging from 6.6 to 40.3 per 100,000/year, where contact lens use rather than trauma is the predominant risk factor [6].
Fungal pathogens contribute to nearly one-quarter of all microbial keratitis cases globally, with India reporting even higher rates of 26%-37% of corneal ulcers being fungal in origin [6]. Among these, Fusarium species dominate in tropical climates, accounting for 40%-60% of fungal keratitis cases [6-8]. The estimated global burden of fungal keratitis exceeds one million cases annually, with Fusarium keratitis alone responsible for 420,000-630,000 cases [8]. This aggressive pathogen is distinguished by rapid stromal invasion, poor responsiveness to conventional antifungals, and a frequent need for surgical intervention.
Although adults constitute the majority of keratitis cases (87%-97%), children represent a smaller but clinically important group, comprising 3%-13% of all keratitis presentations [9-11]. Pediatric keratitis is often associated with trauma in developing countries and contact lens use in developed regions [9,11]. The course is frequently more severe in children due to delayed recognition, communication barriers, and challenges with compliance, which increase the risk of amblyopia and long-term visual disability [9,11]. Within pediatric fungal keratitis, Fusarium species are consistently reported as the most common isolate, comprising more than 60% of cases in large series [9,11] (Figure 4 and Table 1).
Published cases of pediatric Fusarium keratitis in different countriesGeographic distribution of pediatric Fusarium keratitis cases [1,9,12-15] Source: Map created using MapChart (www.mapchart.net)
The present case highlights these global patterns: classic clinical features, including feathery-edged infiltrates, stromal involvement, and early hypopyon-facilitated timely suspicion of fungal keratitis. Importantly, bacterial and fungal keratitis are often clinically indistinguishable at presentation, making early microbiological evaluation indispensable. Turnaround time from corneal scraping to definitive identification was three days, aligning with recommendations in the literature for timely confirmation and targeted therapy [17].
Dual antifungal therapy with natamycin and voriconazole was employed, reflecting evidence that combination therapy can be more effective than monotherapy in Fusarium infections [18]. Natamycin remains the gold-standard first-line agent for filamentous fungi, while voriconazole, with its superior stromal penetration, is valuable in deep or refractory infections [19]. The rapid resolution of hypopyon and reduction in ulcer size within 72 hours mirror reported outcomes of early, aggressive dual therapy.
This case also highlights the detrimental role of unsupervised corticosteroid use in ocular disease. Steroids, though beneficial in immune-mediated conditions, suppress local defenses and permit unchecked fungal proliferation [5]. Public health interventions, pharmacist regulation, and awareness campaigns are essential to prevent such misuse, particularly in low-resource settings. While pediatric Fusarium keratitis remains relatively rare, outcomes are often poor due to late diagnosis, inadequate therapy, and surgical dependence. By contrast, the favorable resolution in this case illustrates how early clinical recognition, prompt microbiological confirmation, and aggressive anti-fungal therapy can dramatically improve prognosis. At a global level, however, challenges, including limited access to natamycin in many regions, suboptimal drug delivery systems, and high surgical burden, remain. These underscore the urgent need for novel antifungal agents, improved treatment delivery, and preventive strategies to reduce the global burden of Fusarium keratitis.
Conclusions
Pediatric Fusarium keratitis, though rare, demands high clinical suspicion following ocular trauma. This case highlights the effectiveness of early dual antifungal therapy, initiated based on classical clinical signs and rapidly supported by microbiological evidence. The favorable outcome without surgical intervention reinforces the importance of early sample collection, accurate diagnosis, and intensive medical management. It also serves as a reminder of the potential hazards of unsupervised corticosteroid use in red eye conditions. This case contributes valuable evidence to the limited literature on pediatric fungal keratitis and supports current recommendations advocating prompt empirical treatment when fungal etiology is suspected.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Fungal keratitis: the Aravind experience Indian J Ophthalmol Prajna VN Prajna L Muthiah S 9129196520172904405310.4103/ijo.IJO_821_17PMC 5678324 · doi ↗ · pubmed ↗
- 2Fungal infections of the cornea Eye (Lond) Thomas PA 8528621720031463138910.1038/sj.eye.6700557 · doi ↗ · pubmed ↗
- 3A study on childhood microbial keratitis in South India Indian J Ophthalmol Chandratreya MP Mudduluru D Venugopal A Varghese AK Ghorpade AS 8418467120233687268910.4103/ijo.IJO_1314_22PMC 10229912 · doi ↗ · pubmed ↗
- 4Risk factors for treatment outcome in fungal keratitis Ophthalmology Lalitha P Prajna NV Kabra A Mahadevan K Srinivasan M 52653011320061658141410.1016/j.ophtha.2005.10.063 · doi ↗ · pubmed ↗
- 5Corneal ulceration in the developing world--a silent epidemic Br J Ophthalmol Whitcher JP Srinivasan M 622623811997934914510.1136/bjo.81.8.622PMC 1722289 · doi ↗ · pubmed ↗
- 6Infectious keratitis: a review Clin Exp Ophthalmol Cabrera-Aguas M Khoo P Watson SL 5435625020223561094310.1111/ceo.14113 PMC 9542356 · doi ↗ · pubmed ↗
- 7Trends in infectious keratitis 7 2025 2022 https://www.reviewofcontactlenses.com/article/trends-in-infectious-keratitis
- 8The global incidence and diagnosis of fungal keratitis Lancet Infect Dis Brown L Leck AK Gichangi M Burton MJ Denning DW 495721202110.1016/S 1473-3099(20)30448-533645500 · doi ↗ · pubmed ↗