Association between periodontal disease and prostate disease: a mini review
Shuxin Li, Hongliang Cao, Yueqiu Zhang, Tong Yang, Mingxuan Li, Chensen Lv, Xin Lian

TL;DR
This review explores how periodontal disease in the mouth might be linked to prostate diseases like cancer and inflammation.
Contribution
The paper systematically reviews the emerging connections between oral and prostate health, focusing on potential mechanisms and treatment approaches.
Findings
Periodontal disease is linked to systemic conditions, including prostate diseases.
Managing periodontal disease may offer new prevention and treatment strategies for prostate conditions.
The review highlights possible pathological mechanisms connecting oral and prostate health.
Abstract
Periodontal disease (PD) is one of the most common chronic diseases in the oral cavity, typically referring to chronic inflammation caused by infection with pathogenic microorganisms in the oral cavity. PD primarily affects the tissues surrounding the teeth, leading to inflammation of the gums and periodontal tissues, destruction of the alveolar bone, and even loosening of the teeth. Numerous studies have shown that PD is not limited to the oral cavity but is also associated with the occurrence of diseases in multiple systems throughout the body. In recent years, increasing attention has been directed toward the interaction between PD and prostate diseases. This article reviews the potential associations between PD and prostate conditions such as chronic prostatitis, benign prostatic hyperplasia (BPH), and prostate cancer (PCa). It explores the pathological mechanisms underlying this…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
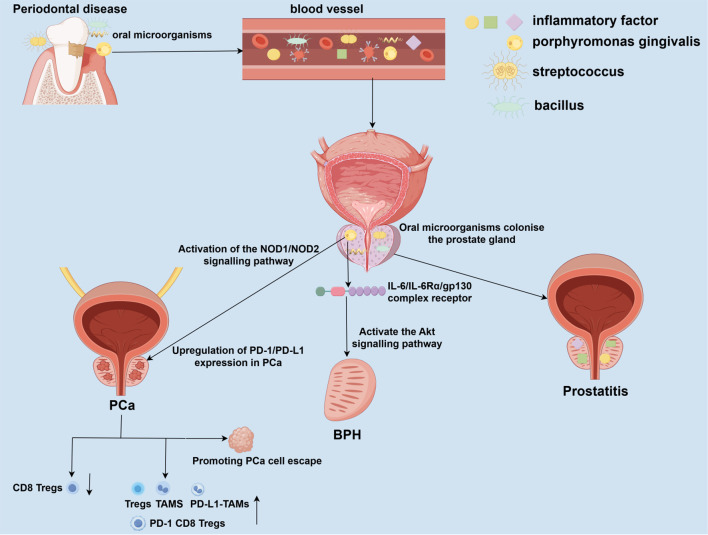 Figure 1
Figure 1| Research type | Prostate disease | First author/Year | Subject | Sample size | Research type | Main outcome |
|---|---|---|---|---|---|---|
| Observational | ||||||
| Cohort Studies | Prostatitis |
| human | 13,530 | Cohort | Periodontitis patients had a higher risk of developing prostatitis. |
| BPH |
| human | 79,497 | Cohort | Periodontitis increased the risk of developing BPH within 1 year. | |
| PCa |
| human | 280 | Prospective Cohort | Men with periodontitis had a significantly increased risk of prostate cancer. | |
| Prostatitis |
| human | 2,013 | Longitudinal Cohort | Periodontal disease was associated with a 14% increased risk of prostatitis. | |
| Case-Control | Prostatitis |
| human | 100 | Case-Control | Periodontal parameters were significantly elevated in patients with moderate to severe prostatitis. |
| PCa |
| human | 372 | Case-Control | The prevalence and severity of periodontitis were higher among prostate cancer cases. | |
| Cross-Sectional | BPH |
| human | 4,930 | Cross-Sectional | PD increased the risk of BPH by 1.68 times. |
| Molecular | Prostatitis/BPH |
| human | 24 | 16S rRNA sequencing | Oral pathogens (e.g., P. gingivalis, T. denticola) were detected in both prostate secretions and plaque samples. |
| BPH/PCa |
| human | 90 | 16S rRNA sequencing | The expression of Corynebacterium was significantly higher in BPH, inflammation, and cancer tissues. | |
| Mendelian randomization | ||||||
| BPH |
| human | 284,358 | MR | No evidence of a causal relationship between periodontitis and BPH was observed. | |
| BPH/Prostatitis |
| human | 489,422 | MR | No causal relationship between periodontitis and prostate disease was found. | |
| Experimental | ||||||
| Animal Studies | BPH |
| human/rat | – | Animal experiments | P. gingivalis infection upregulated inflammatory cytokines and activated the Akt pathway, associated with BPH. |
| PCa |
| rat | – | Animal experiments | Periodontitis promoted tumor growth and immune escape via PD-1/PD-L1, attenuated by anti-PD-1 therapy. | |
| Cell Studies | PCa |
| PCa cells | – | Cell experiments | P. gingivalis infection induced PD-L1 upregulation via NOD1/NOD2, promoting immune evasion. |
| Meta-analysis | PCa |
| human | 440,911 | Meta-analysis | Periodontal disease significantly increased the risk of prostate cancer by 1.40 times. No significant increase was found in treated patients. |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOral microbiology and periodontitis research · Periodontal Regeneration and Treatments · Oral Health Pathology and Treatment
Introduction
1
Prostate diseases are common urological conditions, primarily including non-cancerous prostate conditions such as prostatitis and benign prostatic hyperplasia (BPH), as well as prostate cancer (PCa). The global burden of prostate diseases is significant, particularly among middle-aged and older men (Gupta et al., 2017; Al-Ghazawi et al., 2023; Calderone et al., 2023). Prostate diseases impose a substantial economic burden on society and severely impact men’s quality of life and survival time (Calderone et al., 2023). Prostatitis can occur in men of all ages, with approximately 5–9% of adult men worldwide affected by prostatitis (Li et al., 2020; He et al., 2023). According to the classification system of the National Institutes of Health (NIH), prostatitis can be categorized into acute bacterial prostatitis, chronic bacterial prostatitis, chronic prostatitis, chronic pelvic pain syndrome (CP/CPPS), and asymptomatic prostatitis. Whether acute or chronic, patients with bacterial prostatitis may experience prominent lower urinary tract symptoms (LUTS) and urinary discomfort (Lam and Stokes, 2024). Patients with acute bacterial prostatitis may present with systemic infection symptoms, such as high fever, chills, severe pain in the perineum or suprapubic region, and a swollen, tender prostate palpable during digital rectal examination (Schoeb et al., 2017; Lam and Stokes, 2024; Yang et al., 2024). Chronic bacterial prostatitis, on the other hand, is characterized by recurrent urinary tract infection symptoms, including dull pain in the lower abdomen, and may be accompanied by sexual dysfunction (Schoeb et al., 2017; Lam and Stokes, 2024). The primary clinical symptom of chronic pelvic pain syndrome is persistent pelvic pain lasting ≥3 months, often radiating to the lower back, and frequently accompanied by urinary and sexual dysfunction (Hervás-Pérez et al., 2020; Matsukawa et al., 2022; Stevens et al., 2023). The incidence of BPH increases significantly with age, affecting over half of men over 50 years old (Yu et al., 2020; Calderone et al., 2023; Wang et al., 2025). BPH primarily manifests as non-cancerous enlargement of the prostate gland. The enlarged prostate gland compresses the urethra, causing bladder outlet obstruction and resulting in lower urinary tract symptoms such as weak urine flow, difficulty urinating, and a sensation of incomplete emptying (Sundaram et al., 2017; Zattoni et al., 2017; Dias et al., 2021; Liu et al., 2023; Kaltsas et al., 2025). In severe cases, it can lead to acute urinary retention and recurrent urinary tract infections (Kang et al., 2016; Zattoni et al., 2017; Kim EH. et al., 2018). PCa is the second most common malignant tumor in men globally, following lung cancer (Hussain et al., 2021). The incidence and mortality rates of prostate cancer have significantly increased in recent years, particularly among older men. Common clinical manifestations of PCa include increased nocturia, weakened urine flow, erectile dysfunction, and gross hematuria (Merriel et al., 2018). If PCa metastasizes to the spine and pelvis, it can cause metastatic bone pain (Yamashita et al., 2018). When it invades the spinal cord and nerves, it can lead to neurological symptoms (Viglialoro et al., 2021). However, due to the insidious nature of early symptoms, some cases are already at an advanced stage by the time of diagnosis, increasing treatment difficulty. Although prostate diseases have a high prevalence in the population and significantly impact men’s health, the factors influencing their occurrence and progression remain unclear.
Periodontal disease (PD) is a common, chronic inflammatory condition of the oral cavity, primarily comprising gingivitis or periodontitis (Zhao et al., 2024). PD often affects the supporting tissues surrounding the teeth, including the gums, periodontal ligaments, cementum, and alveolar bone. The development of PD is triggered by a complex inflammatory response resulting from an imbalance of oral microorganisms, which is associated with the immune response to pathogenic microorganisms and their toxins (Zhang et al., 2025). The human oral cavity harbors a diverse array of microorganisms, including bacteria, fungi, viruses, and protozoa, collectively referred to as the oral microbiota (Chattopadhyay et al., 2023). A normal microbiota maintains oral environmental stability, regulates oral pH levels, and stimulates the activation of immune-protective functions in the oral mucosa (Chattopadhyay et al., 2023). However, these microorganisms can also cause oral diseases; an increase in pathogenic bacteria and their metabolites may contribute to tooth destruction and oral tissue inflammation (Zhang et al., 2025). Additionally, oral microorganisms can enter the bloodstream and produce inflammatory factors, potentially triggering diseases in multiple systems throughout the body (Li et al., 2022). Recent studies have shown that PD caused by dysbiosis of the oral microbiota plays a significant role in the onset and progression of prostate diseases. In this review, we summarize epidemiological and pathophysiological studies on the relationship between PD and prostate diseases to explore potential methods for preventing and treating prostate diseases through PD intervention.
Observational and experimental evidence suggest a strong association between PD and prostate disease
2
Recent observational studies have shown that the oral health of male patients with prostate disease differs significantly from that of healthy males. This suggests that PD may play an essential role in the development, progression, and treatment outcomes of prostate disease. Additionally, several animal studies have reported similar findings (Table 1).
PD and prostatitis
2.1
PD is a chronic inflammatory disease, and its inflammatory mediators may affect distant organs through the bloodstream. For example, PD may influence the development of prostatitis. In a clinical study, 100 patients with both PD and chronic prostatitis were grouped, and periodontal parameters and serum PSA levels were recorded separately (Boyapati et al., 2018). It was found that periodontal parameters were significantly elevated in patients with moderate to severe prostatitis, indicating a pathological association between periodontitis and chronic prostatitis. In a cohort study in Taiwan comparing individuals with chronic periodontitis and healthy individuals, the risk of prostatitis was significantly higher in periodontitis patients than in those without periodontitis (Fu et al., 2021). Furthermore, John Estemalik et al. also identified similar DNA from Porphyromonas gingivalis and Treponema denticola in prostate secretions and subgingival plaque from the same individuals with chronic prostatitis (Estemalik et al., 2017). These observational studies suggest that oral pathogens could potentially influence prostatitis through hematogenous spread or direct diffusion, confirming the association between PD and prostatitis.
PD and BPH
2.2
BPH is the most common urinary tract disease in elderly men, mainly manifested as cell proliferation in the prostate tissue, leading to an enlarged prostate. There may be a potential link between PD and the occurrence of BPH. A cross-sectional study of 4,930 men found that PD increased the risk of BPH by 1.68 times, with periodontitis patients having an even higher risk (Wu et al., 2019). In this study, the population was also grouped based on prostate volume, and PD was still found to increase the risk of BPH in different subgroups. However, individuals with a prostate volume >60g had a higher risk of PD (Wu et al., 2019). A cohort study in South Korea found that participants with a history of recurrent periodontitis had a higher incidence of BPH, indicating that chronic periodontitis is a risk factor for BPH (Kwon et al., 2025). Additionally, another study found that patients who underwent periodontal treatment had a reduced risk of BPH (Fu et al., 2021). In patients with both BPH and periodontitis, the same oral pathogens were detected in both prostate fluid and subgingival plaque (Estemalik et al., 2017). These studies suggest that PD may contribute to the development of BPH in men. However, other studies have yielded differing results, and Mendelian randomization studies on PD and BPH have not confirmed causal relationships at the genetic level (Wei et al., 2024; Yang L. et al., 2025). Future prospective cohort studies with larger sample sizes may be needed to clarify the true association between PD and BPH.
PD and PCa
2.3
Prostate cancer (PCa) is one of the most common malignant tumors in men. The association between PD and PCa has been confirmed in numerous studies. In a case-control study involving 152 PCa patients and 220 control cases, periodontal examinations revealed a higher prevalence of PD among PCa patients, suggesting a link between periodontitis and the development of PCa (Vitor et al., 2025). In a 12-year longitudinal cohort study in South Korea, PD was found to increase the risk of PCa by 14%, with a significant positive correlation between PD and PCa (Lee et al., 2017). Additionally, Omer Dizdar et al. conducted a 12-year follow-up study on 280 participants with moderate to severe periodontitis, finding that periodontitis patients had a higher risk of developing PCa and blood cancer (Dizdar et al., 2017). A meta-analysis of cohort studies on the association between PD and PCa found that PD is associated with an increased risk of PCa. However, no significant association was observed in patients who received periodontal treatment (Guo et al., 2021). In another study, using 16S rRNA as primers, genomic DNA analysis of PCa glandular tissue identified specific periodontal pathogens, such as Fusobacterium nucleatum (Alluri et al., 2021). These study results support the view that PD is a risk factor for PCa. Middle-aged and older men should enhance their awareness of oral health and implement preventive and therapeutic measures for PD to reduce the risk of PCa.
Potential biological mechanisms linking PD and prostate disease
3
Although current observational studies have identified several associations between PD and prostate disease, and the differences described in these studies may become targets for the prevention and treatment of prostate disease, their specific mechanisms of action remain to be further clarified. This section will discuss in detail the potential mechanisms of action between PD and prostate disease, as well as how PD affects the development of prostate disease (Figure 1). It has been hypothesized that PD may directly or indirectly affect the onset and progression of prostate disease through the oral-prostate axis (Estemalik et al., 2017; Alluri et al., 2021; Wang SY. et al., 2024). One proposed mechanism suggests that oral pathogens may enter compromised periodontal tissues and subsequently enter and colonize the prostate via the blood or lymphatic systems (Estemalik et al., 2017; Alluri et al., 2021; Wang SY. et al., 2024). Moreover, PD is a chronic inflammatory disease, and the inflammatory factors it releases may affect prostate tissues through blood circulation, leading to a chronic inflammatory microenvironment, which in turn promotes the transformation of prostate disease from inflammation to hyperplasia or cancer. In recent years, with the advancement of biotechnology, researchers have gradually discovered the phenomenon of oral microbial transfer. In one study, 30 prostate tissue samples were selected from patients with inflammation, benign hyperplasia, and cancer (Alluri et al., 2021). Using 16S rRNA as primers, DNA from periodontal pathogens was detected in all these tissues (Alluri et al., 2021). Additionally, Wang et al. cultured subgingival plaque and prostate fluid from patients with BPH complicated by periodontitis, performed 16S rDNA sequencing, and detected oral pathogens such as Porphyromonas gingivalis, Streptococcus oralis, and Fusobacterium nucleatum ( Wang SY. et al., 2024). In animal experiments, researchers established rat models of periodontitis and benign prostatic hyperplasia (BPH), as well as their co-morbidities, to explore their interrelationships. Analysis of the gut microbiota by 16S rDNA sequencing and LC-MS/MS-based fecal metabolomics demonstrated that periodontitis may contribute to the pathogenesis of BPH by inducing dysbiosis of the gut flora and altering microbial-derived metabolites (Guo et al., 2023). When these periodontal pathogens colonize and infect the prostate, they may cause local inflammation and induce the onset of prostatitis. Infection of the prostate with Porphyromonas gingivalis upregulates the expression of inflammatory cytokines interleukin-6 (IL-6), interleukin-6 receptor-α (IL-6Rα), and glycoprotein 130 (gp130) in the tissue. Its toxic factor, Porphyromonas gingivalis lipopolysaccharide (P.g-LPS), activates the Akt pathway through the IL-6/IL-6Rα/gp130 complex, significantly inhibiting prostate cell apoptosis and proliferation while promoting cell mitosis and proliferation, leading to BPH (Wang SY. et al., 2024). Additionally, Porphyromonas gingivalis and its LPS can upregulate PD-1/PD-L1 expression in PCa cells via the NOD1/NOD2 signaling pathway, promoting the increase in the proportion of tumor-associated macrophages (TAMs), regulatory T cells (Tregs), PD-L1 TAMs, and PD-1 CD8 Tregs, while reducing the proportion of CD8 Tregs (Groeger et al., 2022; Wang S. et al., 2024). This alters the tumor microenvironment to promote tumor immune escape and may contribute to the development and progression of PCa (Groeger et al., 2022; Wang S. et al., 2024).
Potential mechanisms linking periodontal disease to prostate disease pathogenesis. Periodontal disease (PD), driven by oral dysbiosis, may impact prostate health through direct and indirect pathways. Oral pathogens from compromised periodontal pockets can enter the circulation and disseminate to the prostate gland. Colonization and infection by these pathogens can directly incite local inflammation, contributing to prostatitis. PD serves as a reservoir of chronic inflammation, releasing pro-inflammatory mediators and components of periodontal pathogens, such as lipopolysaccharide (LPS), into the bloodstream. This systemic inflammatory milieu can promote a pro-inflammatory microenvironment within the prostate. Infection with P. gingivalis and its LPS upregulates inflammatory cytokines, activates the IL-6/IL-6Rα/gp130 complex, and subsequently stimulates the Akt signaling pathway. This cascade disrupts the balance between cell proliferation and apoptosis, favoring prostate tissue hyperplasia. P. gingivalis infection, mediated through pattern recognition receptors, can upregulate immune checkpoint molecules like PD-L1 on tumor cells. This, along with the systemic inflammatory response, contributes to an immunosuppressive TME characterized by increased TAMs, regulatory Tregs, and exhausted CD8+ T cells, ultimately facilitating tumor immune evasion and progression. PD, periodontal disease; BPH, benign prostatic hyperplasia; PCa, prostate cancer; IL-6, interleukin-6; IL-6Rα, interleukin-6 receptor alpha; gp130, glycoprotein 130; LPS, lipopolysaccharide; Akt, protein kinase B; NOD1/2, nucleotide-binding oligomerization domain-containing protein 1/2; PD-L1, programmed cell death ligand 1; TME, tumor microenvironment; TAMs, tumor-associated macrophages; Tregs, regulatory T cells.
Discussion
4
This review focuses on studies investigating the association between PD and prostate disease, as well as the potential mechanisms by which periodontal disease and its common oral pathogens influence the onset and progression of prostate disease (Figure 1). We propose that controlling PD may reduce the risk of developing prostate disease. This review primarily covers epidemiological studies on the association between PD and prostate disease, as well as a limited number of in vivo and in vitro studies. Epidemiological studies mainly include case-control studies and cross-sectional studies. In vivo studies primarily use rat or mouse animal models to simulate how PD-associated pathogens and inflammatory factors promote the development of prostate diseases. In vitro studies mainly involve microbiome and metabolome research, utilizing 16S rRNA sequencing of prostate-related tissues and subgingival exudate (Estemalik et al., 2017).
When interpreting the epidemiological association between PD and prostate diseases, it is essential to consider the influence of multiple potential confounding factors carefully. These confounding variables may partially drive the correlations observed in observational studies. Age represents the most clearly identified common risk factor shared by prostate diseases and PD. Advanced age is not only associated with prostate tissue hyperplasia and the accumulation of genetic mutations. Still, it is also closely linked to the physiological degeneration of periodontal tissues and prolonged microbial exposure (Tan et al., 2021; Fox et al., 2023; Bertolini and Clark, 2024). Furthermore, smoking is a well-established risk factor for periodontitis while also inducing systemic inflammation and oxidative stress (Mazurek-Mochol et al., 2017; Ehsan, 2025). Research indicates smoking may independently increase prostate cancer risk or influence its progression. Smokers typically exhibit poorer oral health and may face distinct prostate disease risks compared to non-smokers, making smoking a significant potential confounder (Tang et al., 2017; AlQobaly et al., 2022; Huang et al., 2024; Yang X. et al., 2025). Diabetes is also strongly associated with more severe and extensive periodontitis, exacerbating periodontal destruction through mechanisms such as advanced glycation end-product (AGEs) accumulation and immune dysfunction (Liu et al., 2018; Nonaka et al., 2018). Simultaneously, diabetes is recognized as a risk factor for BPH (Ozcan et al., 2017). The chronic inflammatory state accompanying diabetes may represent an upstream pathway linking PD to prostate diseases (Chen and Feng, 2023). Socioeconomic status (SES) is a multidimensional factor encompassing education, income, occupation, and access to healthcare. Lower SES is typically associated with poorer oral hygiene, reduced dental care utilization, higher smoking rates, unhealthy diets, and inadequate management of systemic diseases (Fowke et al., 2008; Kim HN. et al., 2018; Park et al., 2018; Tadakamadla et al., 2020; Mikami et al., 2023). These factors may contribute to the elevated burden of both PD and prostate disease in this population, introducing confounding into analyses (Fowke et al., 2008; Kim HN. et al., 2018; Park et al., 2018; Tadakamadla et al., 2020; Mikami et al., 2023). Although most observational studies attempt to control these variables through multivariate regression models, residual confounding may persist. Furthermore, Mendelian randomization studies have failed to establish a genetic-level causal relationship between PD and BPH, which partially weakens the causal inferences drawn from observational findings. This suggests that such associations may be influenced by the confounding factors or reverse causality.
Recent studies have shown that PD is closely associated with prostate diseases, including chronic prostatitis, BPH, and PCa. Research indicates that periodontal disease may affect prostate health through microbial transmission and systemic inflammation, highlighting the importance of oral health in preventing the risk of prostate diseases. Oral pathogens, such as Porphyromonas gingivalis and Fusobacterium nucleatum, have been detected in prostate tissue, supporting the hypothesis that these pathogens may spread from the oral cavity to the prostate via the bloodstream or lymphatic system (Alluri et al., 2021). These pathogens may not only directly induce prostate inflammation but also promote cancer development by altering the local microenvironment. For example, Porphyromonas gingivalis has been shown to upregulate the expression of inflammatory cytokines and activate the Akt signaling pathway and the PD-1/PD-L1 receptor pathway, which are closely associated with the development of BPH and PCa (Groeger et al., 2022; Wang SY. et al., 2024). Furthermore, chronic inflammation caused by periodontal disease can exacerbate prostate lesions by releasing pro-inflammatory mediators such as IL-6 and reactive oxygen species into the bloodstream (Tonguç et al., 2022; Wang S. et al., 2024). This systemic response may sustain a pro-inflammatory environment within the prostate, thereby inducing tissue hyperplasia or malignant transformation (Groeger et al., 2022; Wang S. et al., 2024). The observed reduction in the risk of benign prostatic hyperplasia following periodontal treatment further underscores the critical role of inflammation in disease progression (Fu et al., 2021). Although most observational studies support a positive correlation between PD and prostate disease, considerable heterogeneity exists between studies, with inconsistent and even contradictory conclusions emerging, particularly in BPH research. For instance, cross-sectional and cohort studies by Wu et al. and Kwon et al. both indicated that PD significantly increases the risk of BPH, whereas studies by Wei et al. and Yang et al., based on Mendelian randomization (MR) analysis, failed to identify a genetic causal relationship between the two (Wu et al., 2019; Wei et al., 2024; Kwon et al., 2025; Yang L. et al., 2025). These inconsistencies may stem from several factors. Observational studies are susceptible to confounding variables, while MR analysis, although it reduces confounding, remains sensitive to weak instrumental variables or differences in population structure. Furthermore, inconsistencies in diagnostic criteria for BPH and severity classification of PD across studies may introduce bias. Some studies were based on Asian populations, while others utilized European databases; differences in genetic backgrounds, environmental factors, and healthcare accessibility may affect the generalizability of the findings.
This study has several limitations, primarily focused on epidemiological and in vitro experimental aspects, with limited involvement in vivo experiments. The specific molecular pathways by which bacterial translocation and oral pathogens induce prostatitis and carcinogenesis require further elucidation using advanced animal models and multi-omics approaches. Additionally, while the potential of PD management to alleviate the burden of prostate disease appears promising, it has not been fully explored. However, there is currently a complete lack of evidence from randomized controlled trials (RCTs) to substantiate that treating periodontal disease can alleviate symptoms of prostate conditions or alter their natural course. For instance, whether routine periodontal care for high-risk populations, such as elderly men, can reduce the incidence of PCa remains to be determined. Future research should utilize animal models that simulate the coexistence of PD and prostate disease to elucidate the molecular mechanisms and validate targeted therapeutic approaches. PD can facilitate the entry of oral pathogens into the bloodstream, causing transient bacteremia (Gualtero et al., 2023). While the existence of a resident blood microbiome in healthy individuals is debated and not supported by large-scale studies, it is plausible that during periods of active periodontal infection, these circulating pathogens could disseminate to and seed the prostate gland (Tan et al., 2023). Integrating multi-omics technologies, such as metagenomics and metabolomics, enables a systematic analysis of microbial characteristics and metabolite associations between oral and prostate dysbiosis. Furthermore, metagenomic sequencing of matched oral, blood, and prostate samples allows tracing the migration and colonization pathways of oral microbiota (Tan et al., 2023). Conducting additional randomized controlled trials to evaluate the impact of periodontal treatment on the severity of prostate symptoms or disease progression will provide stronger scientific evidence for clinical application.
Conclusion
5
The interplay between PD and prostate diseases highlights a potential shared pathophysiology centered on infection and inflammation. While current observational evidence suggests an association, it does not establish a causal relationship. Periodontitis may represent a novel, modifiable risk factor for prostate diseases. However, translating this association into clinical practice requires rigorous mechanistic studies to elucidate the causal pathways and, crucially, interventional trials to confirm that periodontal treatment can effectively improve prostate health outcomes. Enhancing oral health awareness and integrating dental care into urological health strategies may offer a promising avenue for the prevention and adjunctive therapy of prostate diseases, pending validation from future research.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Al-Ghazawi M.Salameh H.Amo-Afful S.Khasawneh S.Ghanem R. (2023). An in-depth look into the epidemiological and etiological aspects of prostate cancer: A literature review. Cureus. 15, e 48252. doi: 10.7759/cureus.48252, PMID: 38054148 PMC 10694784 · doi ↗ · pubmed ↗
- 2Alluri L. S. C.Paes Batista da Silva A.Verma S.Fu P.Shen D. L.Mac Lennan G.. (2021). Presence of specific periodontal pathogens in prostate gland diagnosed with chronic inflammation and adenocarcinoma. Cureus. 13, e 17742. doi: 10.7759/cureus.17742, PMID: 34659955 PMC 8492166 · doi ↗ · pubmed ↗
- 3Al Qobaly L.Abed H.Alsahafi Y.Sabbah W.Hakeem F. F. (2022). Does smoking explain the association between use of e-cigarettes and self-reported periodontal disease? J. Dent. 122, 104164. doi: 10.1016/j.jdent.2022.104164, PMID: 35580834 · doi ↗ · pubmed ↗
- 4Bertolini M.Clark D. (2024). Periodontal disease as a model to study chronic inflammation in aging. Geroscience. 46, 3695–3709. doi: 10.1007/s 11357-023-00835-0, PMID: 37285008 PMC 11226587 · doi ↗ · pubmed ↗
- 5Boyapati R.Swarna C.Devulapalli N.Sanivarapu S.Katuri K. K.Kolaparthy L. (2018). Unveiling the link between prostatitis and periodontitis. Contemp Clin. Dent. 9, 524–529. doi: 10.4103/ccd.ccd_746_18, PMID: 31772457 PMC 6868634 · doi ↗ · pubmed ↗
- 6Calderone C. E.Turner E. M.Hayek O. E.Summerlin D.West J. T.Rais-Bahrami S.. (2023). Contemporary review of multimodality imaging of the prostate gland. Diagnostics (Basel) 13, 1860. doi: 10.3390/diagnostics 13111860, PMID: 37296712 PMC 10252565 · doi ↗ · pubmed ↗
- 7Chattopadhyay I.Lu W.Manikam R.Malarvili M. B.Ambati R. R.Gundamaraju R. (2023). Can metagenomics unravel the impact of oral bacteriome in human diseases? Biotechnol. Genet. Eng. Rev. 39, 85–117. doi: 10.1080/02648725.2022.2102877, PMID: 35861776 · doi ↗ · pubmed ↗
- 8Chen G.Feng L. (2023). Analysis of platelet and monocyte-to-lymphocyte ratio and diabetes mellitus with benign prostatic enlargement. Front. Immunol. 14, 1166265. doi: 10.3389/fimmu.2023.1166265, PMID: 37492582 PMC 10363740 · doi ↗ · pubmed ↗