Effect of Adjuvant Vitamin D Therapy on Total Nasal Symptoms Score, IgE, and Eosinophil Levels in Allergic Rhinitis: A systematic review and meta-analysis
Rahmi Surayya, Dwi R. Pawarti, Rizka F. Perdana, Citrawati D. K. Wungu

TL;DR
This study finds that adding vitamin D to treatment helps reduce nasal symptoms and immune markers in people with allergic rhinitis.
Contribution
A systematic review and meta-analysis showing vitamin D's effectiveness in reducing symptoms and immune markers in allergic rhinitis.
Findings
Vitamin D significantly reduced Total Nasal Symptoms Score in AR patients.
IgE levels were significantly lowered with vitamin D adjuvant therapy.
Eosinophil levels also decreased significantly in patients receiving vitamin D.
Abstract
This review investigated the effects of adjuvant vitamin D therapy on Total Nasal Symptoms Score (TNSS), IgE, and eosinophil counts in patients with allergic rhinitis (AR). The meta-analysis used databases, such as PubMed, Science Direct, Scopus, Web of Science, SAGE journals, and clinicaltrials.gov. Quality appraisal was performed using RoB 2 and NOS tools. The research was guided by the PRISMA 2020 chart and analyzed using RevMan 5.4. Sixteen articles, including 11 randomised controlled trials and five cohorts, met the inclusion criteria. Fourteen articles reported TNSS, while four reported IgE and eosinophil levels. Vitamin D significantly reduced TNSS (SMD –2.24; 95% confidence interval [CI]: –3.05, –1.43; P < 0.00001; I2 = 96%), IgE (SMD –1.45; 95% CI: –2.07 to –0.983; P < 0.00001; I2 = 79%), and eosinophil levels (SMD –2.20; 95% CI: –3.92 to –0.48; P = 0.01; I2 = 97%) in AR…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
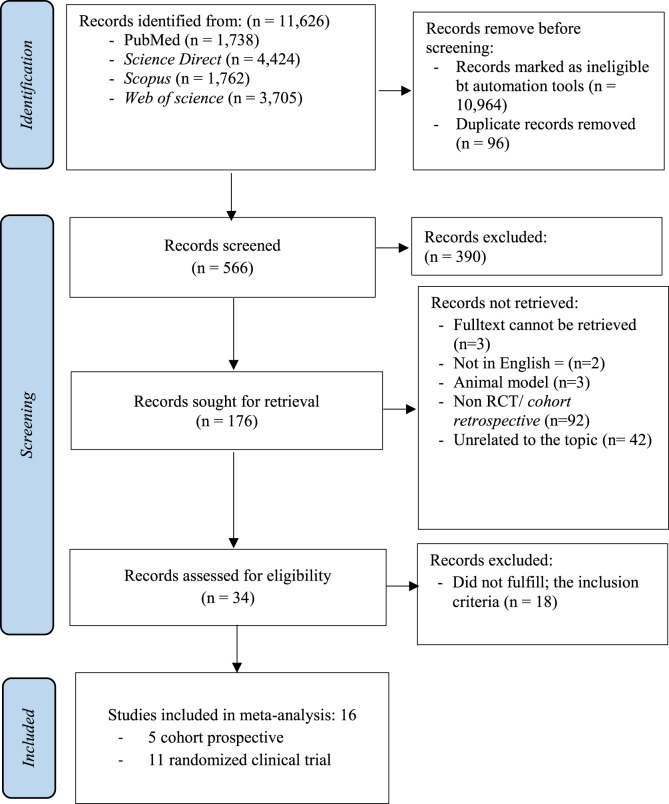 Fig. 1
Fig. 1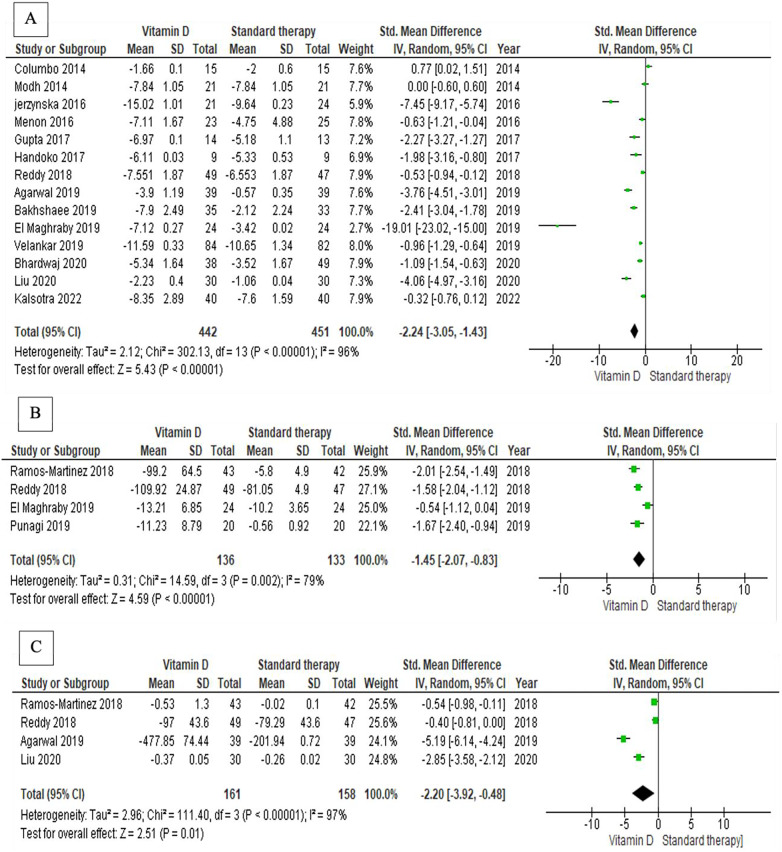 Fig. 2
Fig. 2| NOS | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
|
| |||||||||||
|
|
|
| |||||||||
|
|
|
| |||||||||
| No. | Study | Year | 1 | 2 | 3 | 4 | 1 | 1 | 2 | 3 | Total |
| 1 | Columbo | 2014 | * | * | * | * | ** | * | * | * | 9 |
| 2 | Modh | 2014 | * | * | * | * | * | * | * | * | 8 |
| 3 | Gupta | 2017 | * | * | * | * | * | * | * | 7 | |
| 4 | Agarwal | 2019 | * | * | * | * | ** | * | * | 8 | |
| 5 | El Maghraby | 2019 | * | * | * | * | ** | * | * | * | 9 |
| Vitamin D serum level | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
|
| Type of Vitamin D adjuvant | Duration of follow up | AR Classification | |||||||
| Comparison | Intervention | |||||||||
| No | Study, year, region | Outcome | Population | pre | post | pre | post | |||
| 1 | Columbo | TNSS | Geriatric, over 65 y.o | 29.7 ± 10.6 | 39.7 ± 8.9 | 29.7 ± 10.6 | 39.7 ± 8.9 | Vit D3 | 6 weeks | moderate to severe perennial AR |
| 2 | Modh | TNSS | Adult | 18.0 ± 5.6 | 23.9 ± 9.7 | 18.0 ± 5.6 | 23.9 ± 9.7 | Cholecalciferol | 3 weeks | perennial |
| 3 | Jerzynska | TNSS | Pediatric | 43.3 ± 3.6 | 53.3 ± 3.0 | 48.8 ± 5.3 | 94.8 ± 6.8 | Cholecalciferol | 5 months | intermittent or persistent |
| 4 | Menon | TNSS | Adult | 18.2 ± 4.7 | 18.7 ± 4.8 | 17.3 ± 8.3 | 29.7 ± 2.3 | Cholecalciferol; 1,000 IU | 4 weeks | perennial |
| 5 | Gupta | TNSS | Adult | NA | NA | NA | NA | Cholecalciferol, 1,000 IU | 3 weeks | moderate to severe |
| 6 | Handoko | TNSS | Adult | 10.2 ± 3.4 | 9.4 ± 4.5 | 8.5 ± 4.1 | 18.8 ± 10.8 | Vit D3 | 4 weeks | moderate to severe persistent AR |
| 7 | Ramos-Martinez | IgE, AEC | Adult | NA | NA | NA | NA | Calcitriol | 6 months | perennial |
| 8 | Reddy | TNSS, IgE, AEC | Adult | NA | NA | NA | NA | Vitamin D 1,000 IU | 3 weeks | perennial |
| 9 | Agarwal | TNSS, Eosinophil | Adult | 27.9 ± 13.4 | 27.4 ± 12.8 | 20.2 ± 10.3 | 38.1 ± 14.6 | Cholecalciferol, 1,000 IU | 3 months | perennial |
| 10 | Bakhshaee | TNSS | Adult | 14.67 | 15.1 ± 2.2 | 14.0 | 24.1 ± 3.9 | Vitamin D2 | 8 weeks | perennial |
| 11 | El Maghraby | TNSS, IgE | Adult | NA | NA | NA | NA | Vit D2 | 6 months | seasonal (date pollen) |
| 12 | Punagi | IgE | Adult | 15.3 ± 3.2 | 14.6 ± 3.6 | 14.9 ± 3.4 | 17.4 ± 2.6 | D3 | 4 weeks | seasonal or perennial. |
| 13 | Velankar | TNSS | Adult | 16.8 | 16.2 | 15.9 | 22.4 | Vitamin D 60,000 IU | 2 weeks | persistent moderate to severe |
| 14 | Bhardwaj | TNSS | Adult | NA | NA | NA | NA | Cholecalciferol | 4 weeks | moderate to severe, seasonal or perennial |
| 15 | Liu | TNSS | Adult | 23.4 ± 3.8 | 31.5 ± 2.9 | 23.7 ± 4.5 | 47.6 ± 2.8 | D3 Nasal drop | 4 weeks | mild seasonal pollen |
| 16 | Kalsotra | TNSS | Adult | NA | NA | NA | NA | D3 60,000 IU | 4 weeks | seasonal or perennial |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAllergic Rhinitis and Sensitization · Asthma and respiratory diseases · Urticaria and Related Conditions
1. Introduction
Allergic rhinitis (AR) is a common condition characterised by an immunoglobulin E (IgE)-mediated response to environmental allergens, resulting in significant morbidity and reduced quality of life. Although standard treatments, such as antihistamines and intranasal corticosteroids, are available, many patients experience insufficient symptom relief, indicating a need for alternative therapeutic options.^12^ This inadequacy suggests that current treatments may not fully address the underlying immunological mechanisms involved in AR, necessitating exploration of adjunctive therapies capable of modulating these pathways.^3^
The immunomodulatory capacity of vitamin D has led researchers to investigate its potential as adjuvant therapy for AR. Vitamin D plays a significant role in immune regulation, particularly through modulation of the Th1/Th2 cell balance, which is fundamental to allergic processes.^4^ Studies have shown that vitamin D can inhibit the production of inflammatory cytokines, specifically interleukin (IL)-5 and IL-13, which are associated with eosinophilic inflammation and IgE synthesis.^5^ Furthermore, vitamin D deficiency has been correlated with increased severity of allergic symptoms, suggesting that adequate levels may be necessary for optimal immune function and symptom control in patients with AR.^6^
Epidemiological studies have also demonstrated associations between serum vitamin D concentrations and clinical outcomes in AR, showing that higher vitamin D levels correlate with reduced IgE concentrations and lower symptom severity.^47^ The Total Nasal Symptom Score (TNSS) is a widely used metric for evaluating symptom severity, providing a semiquantitative assessment that aids in determining the effectiveness of therapeutic interventions.^8^ Randomised controlled trials (RCTs) have evaluated these outcomes alongside observational studies using scales such as the Newcastle–Ottawa Scale (NOS) for quality appraisal and the Cochrane Risk of Bias 2 (RoB 2) tool for assessing risk of bias in RCTs. Immunoglobulin E plays a crucial role in allergic disease pathophysiology by sensitising mast cells and triggering the release of inflammatory mediators that exacerbate allergic responses.^9^ Elevated IgE levels are often observed in patients with AR, correlating with symptom severity and eosinophilia, indicative of ongoing allergic inflammation.^1011^
Recent studies suggest that vitamin D may enhance the efficacy of conventional treatments through its immunomodulatory effects on innate and adaptive immune responses.^1213^ Additionally, vitamin D may augment glucocorticoid pathway activity, potentially reducing the required doses of corticosteroids in AR management.^14^ The interplay between vitamin D, IgE, and eosinophil counts in AR remains an area of active investigation. Some studies suggest that adequate vitamin D levels may reduce IgE production and eosinophilic inflammation, thereby alleviating AR symptoms.^1015^ However, findings remain inconclusive, with several studies failing to demonstrate a substantial effect of vitamin D supplementation on allergy-related outcomes across different populations.^1516^
Therefore, this systematic review aimed to investigate the effects of adjuvant vitamin D therapy on TNSS, IgE levels, and eosinophil counts in patients with AR, contributing to a clearer understanding of its therapeutic potential in allergic conditions.
2. Methods
This systematic review adhered to PRISMA guidelines and was registered in PROSPERO.^17^ A systematic literature search guided by a predefined PICOS framework (population, intervention, comparison, outcomes, and study design) targeted individuals of varying ages, ethnicities, and geographic origins diagnosed with AR. The intervention examined was vitamin D supplementation in addition to conventional AR treatment, compared to standard therapy alone.
2.1. Eligible criteria
This review aimed to evaluate the effect of adjunctive vitamin D therapy on TNSS, IgE concentration, and eosinophil count in patients with AR. Diagnosis of AR was based on clinical symptoms assessed by a rhinologist and/or by skin prick testing. RCTs and prospective cohort studies were eligible. Studies were included if they evaluated vitamin D supplementation in patients with AR using TNSS, IgE levels, and/or eosinophil counts as outcome measures. Articles addressing allergic conditions, including atopic dermatitis and asthma, were included provided that AR was one of the conditions examined. Studies were excluded if they involved animal research, cytokine or genetic data, or if they only evaluated serum vitamin D levels in specific populations such as intensive care patients or individuals with chronic or infectious diseases (e.g., tuberculosis, hypertension, autoimmune diseases, and cancer). Case-control studies, case series, and cross-sectional studies were excluded.
2.2. Search strategy
Articles were systematically retrieved from PubMed Central, publisher websites, ScienceDirect, Scopus, Web of Science, ClinicalTrials.gov, and the Cochrane Central Register of Controlled Trials. The search was conducted over two months, ending on 31 October 2022. Only articles published in Indonesian or English with full manuscripts available (open access) were included. No restrictions were imposed on publication year or type. Search terms included a combination of keywords and Medical Subject Headings (MeSH), as follows: (“allergic rhinitis” OR “perennial allergic rhinitis” OR “seasonal allergic rhinitis” OR “hay fever”) AND (“vitamin D” OR “cholecalciferol” OR “calcitriol” OR “dihydroxyvitamin D”).
2.3. Data extraction
Data extraction was performed by the primary investigator (R.S.) and independently verified by two reviewers (D.R.P. and R.F.P.). Titles and abstracts were screened for relevance, with ambiguous abstracts discussed collaboratively. Full-text articles were independently assessed for eligibility, with exclusion reasons documented. Included articles were cross-checked to maintain data integrity and prevent overlap. Discrepancies were resolved through discussion.
2.4. Assessment of methodological quality
Methodological quality was assessed using RoB 2 for RCTs and NOS for cohort studies. Two authors (R.S. and D.R.P.) independently evaluated each article, with final assessments reached through discussion; disagreements were resolved by consulting the third author (R.F.P.). RoB 2 evaluates bias across five domains: randomisation process, deviations from intended interventions, missing outcome data, outcome measurement, and selection of reported results, categorising studies as having low, moderate, or high risk of bias.^18^ NOS assesses non-randomised studies based on three dimensions—selection, comparability, and outcome—using a star system, with high-quality studies scoring up to nine stars.^19^
2.5. Statistical analysis
Extracted data were used to compute mean differences and 95% confidence intervals (CIs). When studies presented outcomes using different scales, SMD was applied for meta-analysis. The I^2^ statistic assessed heterogeneity, indicating the percentage of total variation between studies.^20^ Publication bias was evaluated using funnel plots based on standard error.^21^ An I^2^ value exceeding 50% indicated substantial heterogeneity, warranting a random-effects model; otherwise, a fixed-effects model was used. Data analysis was performed using Review Manager version 5.4 (The Cochrane Collaboration, London, UK).
3. Results
Of the 11,262 articles identified in the initial literature search, 34 were selected for in-depth analysis. Approximately 10,964 articles were excluded automatically by screening tools, and a further 96 were removed due to duplication. During screening of 566 articles, 390 were excluded for not meeting PICOS criteria. The population across included articles comprised patients with AR diagnosed clinically by an otorhinolaryngologist or through skin prick testing. The intervention involved adjuvant therapy with vitamin D compared to conventional AR therapy, with outcomes including TNSS, IgE levels, and eosinophil counts. All included articles were RCTs or prospective cohort studies. Following detailed review of 176 articles, 142 were excluded due to inability to retrieve full texts, lack of English language availability, or non-clinical study design. Of the 34 articles reviewed in full, 18 were excluded for not reporting mean ± SD values or differences in the three primary parameters. Sixteen articles were included in the meta-analysis. A visual presentation of the study selection process is provided [Fig. 1].
Flowchart of the study selection process.
The quality of observational studies was assessed using the NOS, which awards up to nine stars [Table 1]. Data from included articles were systematically collected using a standardised Excel spreadsheet.
3.1. Characteristic of included studies
Sixteen studies published between 2014 and 2022 investigated the efficacy of vitamin D adjuvant therapy in patients with AR. These studies assessed one or more of the following primary outcomes: TNSS, IgE levels, and eosinophil counts. Mean TNSS, IgE levels, and eosinophil counts were elevated prior to treatment across all studies and decreased to normal or near-normal levels following vitamin D supplementation. Treatment duration ranged from two weeks to six months, with an average duration of four weeks in most studies. The collected data encompassed study details, patient demographics, serum vitamin D concentrations before and after treatment, specific vitamin D supplements administered, duration of follow-up, and severity classification of AR [Table 2].
In total, 504 patients were enrolled in the vitamin D adjuvant therapy groups and 513 in control groups. One study evaluated individuals over 65 years of age (geriatric population),^22^ while another assessed children under five years (paediatric population).^23^ The remaining studies investigated adult populations, defined here as individuals aged 13–60 years.
3.2. Effect of vitamin D adjuvant therapy to TNSS, IgE, and eosinophil in allergic rhinitis patients
All included articles evaluated the effects of adjuvant vitamin D therapy on TNSS, IgE, and eosinophil levels. TNSS was measured in 14 studies,^1822232425262728293031323334^ IgE levels were assessed in four studies,^27313536^ and eosinophil counts were reported in four studies.^26313435^ Meta-analysis revealed that TNSS, IgE, and eosinophil levels decreased significantly following administration of adjuvant vitamin D therapy [Fig. 2]. A substansial decrease in nasal symptoms was seen in AR after Vitamin D administration (SMD = –2.24, 95% CI: -3.05 to -1.43; P = 0.001). Compared to standard therapy, vitamin D has a stronger effect on reducing nasal symptoms. Despite its significant heterogeneity (I^2^ = 96%), the results are more thorough because it has the largest sample and the most research [Fig. 2A]. Combined effect of vitamin D supplementation on AR to lower IgE secretion can be seen in [Fig. 2B]. It showed a significant effect on reducing IgE secretion (SMD =-1.45, 95% CI: -2.07 to -0.83; P = 0.001). Despite its impact on nasal symptoms being stronger, the studies in this group are more focussed and their moderate heterogeneity (I^2^ = 79%) may suggest that they are consistent with one another. The combined effect of vitamin D supplementation on AR in lowering eosinophil count showed in [Fig. 2C]. its significant heterogeneity (I^2^ = 97%) and broader confidence interval suggest greater ambiguity surrounding the effect size. However, the mean difference is still substantial and statistically significant (SMD =-2.20, 95% CI: -3.92 to -0.48; P = 0.01). Examination of the funnel plot indicated potential publication bias, as evidenced by asymmetrical distribution of plots on either side, with a standard error <0.4.
Effect of adjuvant vitamin D therapy on nasal symptoms, IgE, and eosinophil counts in patients with allergic rhinitis. A: Vitamin D supplementation's combined effect in reducing AR nasal symptoms. B: Vitamin D supplementation's combined effect on AR to lower IgE secretion. C: Vitamin D supplementation's combined effect on AR in lowering eosinophil count.
4. Discussion
Most of the studies included in this review were conducted in Asia, a region characterised by tropical and subtropical climates. The included articles encompassed diverse countries, ethnicities, and age groups. AR was predominantly observed among young adults, with a mean age of 29.5 years. These findings are consistent with Pontoh et al., who reported a higher prevalence of AR in younger populations. This trend may be attributable to the typically active and productive nature of young individuals, leading to increased exposure to allergens in professional, academic, or social settings.^37^
Cholecalciferol and calcitriol, derivatives of vitamin D_3_, were the primary forms used as adjuvant therapies for AR. While vitamin D exists in two forms, D_3_ and D_3_, cholecalciferol is often preferred due to its stronger binding affinity to the vitamin D binding protein (VDBP) receptor compared to vitamin D_2_.^3839^ This high affinity results in a prolonged half-life in circulation, maintaining higher serum concentrations over time. Furthermore, the D25-hydroxylase enzyme converts pro-vitamin D_3_ to 25(OH)D_3_ (the active form of vitamin D_3_ in blood) at a rate five times faster than it converts pro-vitamin D_2_ to 25(OH)D_2_.^3840^
In most analysed studies, vitamin D was administered at a dosage of 1,000 IU as a single daily dose.^23282931^ However, Columbo et al. used a lower daily dose of 400 IU,^22^ while one study administered 6,000 IU daily,^18^ and two studies adopted weekly dosing regimens of 60,000 IU.^2432^ Another investigation used a weekly dose of 50,000 IU.^33^ The predominant route of administration was systemic (oral intake), with one notable exception where topical vitamin D_3_ nasal drops were used.^18^ The doses employed across these studies align with guidelines from the International Organization of Medicine (IOM), which recommend increased dosages up to 50,000 IU weekly for 6–8 weeks in cases of deficiency.^41^
Topical nasal delivery of vitamin D enhances bioavailability and therapeutic efficacy. Nasal drops offer targeted absorption via the nasal mucosa, bypassing digestive enzymes and first-pass liver metabolism, thereby significantly improving bioavailability due to vitamin D_3_'s low molecular weight (4,000 g/mol). Moreover, the nasal mucosa demonstrates high affinity for lipophilic substances such as vitamin D_3_.^42^
The follow-up periods for vitamin D adjuvant therapy in the reviewed studies varied substantially, ranging from two weeks to six months.^2733^ Five studies implemented a four-week follow-up protocol,^1824283034^ while other durations included three weeks,^2529^ six weeks,^22^ eight weeks,^32^ three months,^26^ five months,^23^ and six months.^27^ Most studies adopted a four-week regimen. Vitamin D, a secosteroid within the steroid hormone group, is synthesised in the skin from 7-dehydrocholesterol via ultraviolet radiation exposure.^4143^ Accordingly, evaluation of vitamin D administration in patients with AR should be aligned with assessment methods used for standard steroid therapy. The ARIA 2008 guidelines recommend a two- to four-week administration period following treatment initiation.^44^
Statistical analysis demonstrated a significant reduction in TNSS after adjuvant vitamin D therapy (SMD = –2.24, 95% CI: -3.05 to -1.43; P = 0.001). This effect may be attributable to vitamin D's capacity to modulate immune system function. It influences the activity of various immune cells, including monocytes, dendritic cells, and T and B lymphocytes, which are crucial for adaptive immunity. Additionally, vitamin D affects the immune-related functions of epithelial cells.^2545^ Certain immune cells also possess enzymes that enable activation of vitamin D, allowing for localised conversion of inactive vitamin D to active calcitriol, thereby exerting paracrine and autocrine effects.
Adjuvant vitamin D therapy was effective in reducing IgE levels in patients with AR. Statistical analysis revealed a significant decrease in IgE levels following administration of vitamin D as adjuvant treatment. Type I hypersensitivity reactions are significantly influenced by IgE concentration. The transcriptional mechanism of ε-germline transcription mediates resistance to IgE production. This process begins when 25(OH)D binds to its receptor VDR, forming a heterodimer with the retinoid X receptor, which subsequently binds to VDRE in B cells. Transcription of the varepsilon germline occurs in the target gene region Iε. Inhibition of ε germline gene transcription suppresses the IgE class-switch recombination phase, thereby reducing IgE production.^394647^ Vitamin D also inhibits maturation of antigen-presenting cells and Th2 cells through direct or indirect mechanisms, including reduced IL-2 secretion and increased IL-10 production. This process induces T-cell regulatory hyporesponsiveness and inhibits mast cell degranulation, ultimately lowering IgE secretion.^47^
The main limitation of this study was that all types of AR, both seasonal and perennial, were evaluated without specifying the severity of AR experienced by the patients. The findings suggest that the effect of vitamin D on persistent and seasonal AR may differ, as the follow-up period after vitamin D administration varied between the two conditions.
This review found that adjuvant vitamin D therapy significantly decreased eosinophil infiltration (SMD = –2.20, 95% CI: -3.92 to -0.48; P = 0.01, I^2^ = 97%). Eosinophils are the primary inflammatory cells associated with AR. Vitamin D deficiency has been shown to induce spontaneous eosinophil activation.^34^ An inverse relationship exists between vitamin D levels and blood eosinophil counts in individuals with persistent AR.^3448^ Adjuvant vitamin D therapy has thus demonstrated efficacy in reducing eosinophil counts in patients with AR.
5. Conclusion
Adjuvant vitamin D therapy was effective in managing AR, as evidenced by significant reductions in TNSS, IgE levels, and eosinophil counts. The immunomodulatory properties of vitamin D address multiple aspects of AR pathophysiology, complementing conventional therapies. However, heterogeneity in dosing regimens, administration routes, and follow-up periods highlights the need for further research to establish optimal protocols and understand long-term effects. Although large-scale clinical trials are required to confirm these findings and refine treatment guidelines, this meta-analysis provides compelling evidence that vitamin D could serve as a complementary treatment for AR.
Authors' Contribution
Rahmi Surayya: Conceptualization, Methodology, Software, investigation, resources, Writing- Original draft preparation, Writing - Review & Editing. Dwi R. Pawarti: Validation, Supervision, Writing - Review & Editing. Rizka F. Perdana: Investigation, Validation, Resources, Writing - Review & Editing. Citrawati D.K. Wungu: Methodology, Data Curation, Writing - Review & Editing.
Data Availability
Data is available upon reasonable request from the corresponding author.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Jia X Zheng H Yan X Dai H Xiang Q Effect of baseline serum Vitamin D level on symptom and medication scores of subcutaneous immunotherapy in children with mite allergy. Front Pediatr 2022; 10:1018549. https://doi.org/10.3389/fped.2022.1018549.10.3389/fped.2022.101854936389357 PMC 9663479 · doi ↗ · pubmed ↗
- 2Joudi M Hosseini RF Khoshkhui M Salehi M Kouzegaran S Ahoon M Effects of serum vitamin D and efficacy of subcutaneous immunotherapy in adult patients with allergic rhinitis. Allergy Asthma Immunol Res 2019; 11:885. https://doi.org/10.4168/aair.2019.11.6.885.10.4168/aair.2019.11.6.88531552722 PMC 6761068 · doi ↗ · pubmed ↗
- 3Cho SW Zhang YL Ko YK Intranasal treatment with 1, 25-dihydroxyvitamin D 3 alleviates allergic rhinitis symptoms in a mouse model. Allergy Asthma Immunol Res 2019; 11:267. https://doi.org/10.4168/aair.2019.11.2.267.10.4168/aair.2019.11.2.26730661318 PMC 6340801 · doi ↗ · pubmed ↗
- 4Hembrom R Patra S Sinha R Sen I Mandal SC Chakrabarti A Vitamin D: A silent cofactor for allergic rhinitis. Bengal J Otolaryngol Head Neck Surg 2019; 27:107–12. https://doi.org/10.47210/bjohns.2019.v 27i 2.236.10.47210/bjohns.2019.v 27i 2.236 · doi ↗
- 5Izmailovich M Gazaliyeva M Glushkova N Suleimenov EM Suleimenov YA Allergen-specific immunotherapy in combination with vitamin D in patients with seasonal allergic rhinitis. Russian Open Med J 2022; 11:e 0205. https://doi.org/10.15275/rusomj.2022.0205.10.15275/rusomj.2022.0205 · doi ↗
- 6Izmailovich M Gazaliyeva M Glushkova N Semenova Y Burankulova S Shaydarova S Association between serum 25-hydroxyvitamin D concentration and severity of seasonal allergic rhinitis in Karaganda region (Kazakhstan). J Clin Med Kazakhstan 2022; 19:46–50. https://doi.org/10.23950/jcmk/12686.10.23950/jcmk/12686 · doi ↗
- 7Sudiro M Lestari BW Madiadipoera T Setiabudiawan B Boesoirie TS Vitamin D deficiency is correlated with severity of allergic rhinitis. O Alib 2017; 04:1–9. https://doi.org/10.4236/oalib.1103813.10.4236/oalib.1103813 · doi ↗
- 8Muddaiah D Venkatarangaiah S A study on total serum Ig E levels and absolute Eosinophil count in allergic rhinitis patients. J Evol Med Dent Sci 2020; 09:76–80. 10.14260/jemds/2020/17. · doi ↗