C. Diff-erently: evaluating the association of inappropriate antibiotic use with hospital-onset Clostridioides difficile infection
Amie John, Antoinette Acbo, Kelsie Cowman, Yi Guo, Priya Nori, Gregory Weston

TL;DR
This study examines whether inappropriate antibiotic use is linked to hospital-onset Clostridioides difficile infection in a New York City hospital.
Contribution
The study evaluates the association between inappropriate antibiotic use and hospital-onset C. difficile infection in an inpatient setting.
Findings
Elevated or inappropriate antibiotic use was not associated with hospital-onset C. difficile infection.
The study compared antibiotic use in C. difficile cases to matched controls in an inpatient setting.
Abstract
Hospital-onset C. difficile infection (HO-CDI) remains a common cause of healthcare-associated infection. This study evaluated antibiotic use (AU) and appropriateness in hospital-onset C. difficile cases compared to matched controls in an inpatient setting at a New York City hospital. Elevated or inappropriate AU was not associated with HO-CDI.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
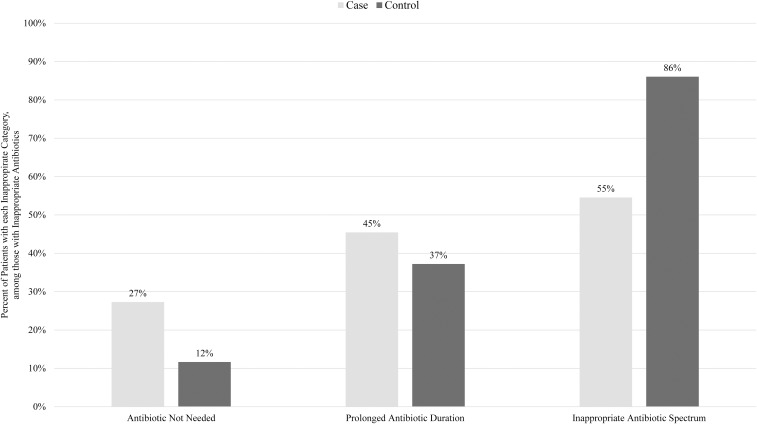 Figure 1
Figure 1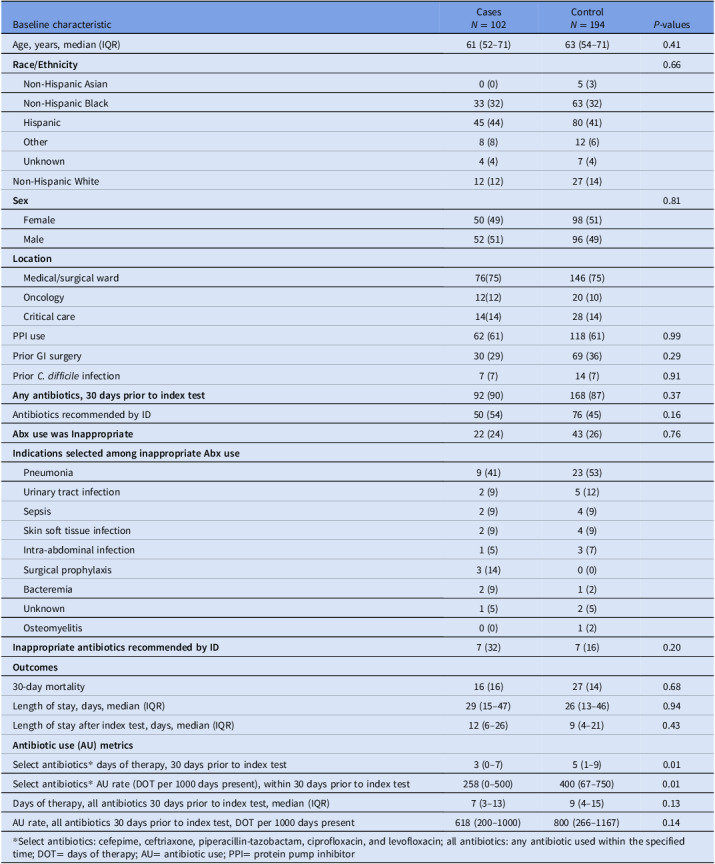 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntibiotic Use and Resistance · Pharmaceutical Practices and Patient Outcomes · Patient Satisfaction in Healthcare
Introduction
Hospital-onset Clostridioides difficile infection (HO-CDI) is a common healthcare-associated infection and is associated with increased costs, morbidity, and mortality.^ 1–3 ^ Although any antibiotic exposure might increase patient risk for HO-CDI, unnecessary antibiotic use (AU) represents the modifiable portion of that risk. Studies have shown substantial inappropriate AU in patients with CDI, but without comparison to control patients.^ 4 ^ This study evaluated the association of inappropriate AU with HO-CDI.
Methods
This observational, retrospective, case–control study included admitted patients ≥18 years with a CDI test between 1/1/23 and 2/28/24. Testing consisted of initial glutamate dehydrogenase/toxin testing (Techlab, Inc.) with additional PCR (Cepheid GeneXpert) for discordant glutamate dehydrogenase and toxin results. HO-CDI cases were defined by National Healthcare Safety Network criteria.^ 5 ^ Controls had a negative CDI test sent on or after hospital day 4 and no positive CDI test within the index admission. In controls with multiple negative CDI tests, the last one was used for analysis. Cases and controls were matched 1:2, when possible, based on patient location (critical care, oncology, or medical-surgical) and month of index test. Inappropriate AU and antibiotic indication were determined by chart review by an infectious diseases (IDs) trained physician or pharmacist. Inappropriate AU was categorized as antibiotic not needed, prolonged antibiotic duration, or inappropriate antibiotic spectrum (Supplement Part A). Appropriateness of AU for infectious syndromes was determined using institutional guidelines (Supplement Parts B, C).^ 6 ^ Questionable instances of inappropriate AU or antibiotic indication were adjudicated by additional investigators. Patients could be assigned multiple categories of inappropriateness. The AU rate of all antibiotics and selected high-risk antibiotics^ 7 ^—cefepime, ciprofloxacin, levofloxacin, ceftriaxone, and piperacillin-tazobactam—during 30 days prior to the index test was calculated as days of therapy (DOT) per 1000 patient days. Demographics, race and ethnicity, proton pump inhibitor use, prior CDI history, gastrointestinal surgery, hospital length of stay (LOS), and all-cause mortality within 30 days of index test were collected from the electronic health record.
Sample size calculation
We included eligible cases during the study period that had at least one matching control patient. We used a previous study to estimate inappropriate AU in cases^ 4 ^ and calculated that matching cases to controls 1:2 would provide 80% power with α = 0.05 to detect an effect size of 45% inappropriate AU in the cases and 28% in controls.
Statistical analysis
Baseline characteristics and secondary outcomes were summarized using descriptive statistics. Bivariate analyses were conducted via χ2 test, Fisher’s exact test, and Wilcoxon rank sum as appropriate. All tests were two-tailed, and *p–*values < .05 were considered significant. Statistical analysis was conducted using SAS version 9.4 software (SAS Institute, Cary, NC).
Results
Two hundred ninety-six patients were included: 102 cases and 194 controls. Only one matching control could be identified for ten cases. Median age was similar between cases and controls (61 vs 63 yr). Substantial proportions of the population identified as Black (32% cases and 32% controls) or Hispanic (44% cases and 41% controls). There were no significant differences in race or ethnicity distribution between cases and controls. Most patients were admitted to medical-surgical wards (75% cases and 75% controls). The ID service recommended antibiotics in 54% of cases and 46% of controls. AU rate for high-risk antibiotics was lower in cases compared to controls (P = .01) (Table 1). However, there was no significant difference between the groups in AU rate for all antibiotics. Inappropriate AU was observed in 24% of cases and 26% of controls with prior AU (P = .76). The most common category of inappropriate AU was inappropriate spectrum—accounting for 55% and 86% of inappropriate AU among cases and controls, respectively (Figure 1). No need for antibiotic therapy accounted for 27% of inappropriate AU among cases and 12% among controls. The most common indication for prescribed inappropriate antimicrobials was pneumonia (41% cases and 53% controls). There were no significant differences in mortality or LOS.
Figure 1.Categories of inappropriate antibiotic use. Denominator of percentage is the number of patients who had inappropriate antibiotic use (case n = 22; control n = 43). A given patient could have more than one category of inappropriate antibiotic use, and more detailed definitions of each category of inappropriate antibiotic use are available in the supplementary appendix.
Table 1.Characteristics, antibiotic utilization and appropriateness, and outcomes, stratified by groupBaseline characteristicCases N = 102Control N = 194 P-valuesAge, years, median (IQR)61 (52–71)63 (54–71)0.41 Race/Ethnicity 0.66 Non-Hispanic Asian0 (0)5 (3) Non-Hispanic Black33 (32)63 (32) Hispanic45 (44)80 (41) Other8 (8)12 (6) Unknown4 (4)7 (4)Non-Hispanic White12 (12)27 (14) Sex 0.81 Female50 (49)98 (51) Male52 (51)96 (49) Location Medical/surgical ward76(75)146 (75) Oncology12(12)20 (10) Critical care14(14)28 (14)PPI use62 (61)118 (61)0.99Prior GI surgery30 (29)69 (36)0.29Prior C. difficile infection7 (7)14 (7)0.91 Any antibiotics, 30 days prior to index test 92 (90)168 (87)0.37Antibiotics recommended by ID50 (54)76 (45)0.16 Abx use was Inappropriate 22 (24)43 (26)0.76 Indications selected among inappropriate Abx use Pneumonia9 (41)23 (53) Urinary tract infection2 (9)5 (12) Sepsis2 (9)4 (9) Skin soft tissue infection2 (9)4 (9) Intra-abdominal infection1 (5)3 (7) Surgical prophylaxis3 (14)0 (0) Bacteremia2 (9)1 (2) Unknown1 (5)2 (5) Osteomyelitis0 (0)1 (2) Inappropriate antibiotics recommended by ID 7 (32)7 (16)0.20 Outcomes 30-day mortality16 (16)27 (14)0.68Length of stay, days, median (IQR)29 (15–47)26 (13–46)0.94Length of stay after index test, days, median (IQR)12 (6–26)9 (4–21)0.43 Antibiotic use (AU) metrics Select antibiotics* days of therapy, 30 days prior to index test3 (0–7)5 (1–9)0.01Select antibiotics* AU rate (DOT per 1000 days present), within 30 days prior to index test258 (0–500)400 (67–750)0.01Days of therapy, all antibiotics 30 days prior to index test, median (IQR)7 (3–13)9 (4–15)0.13AU rate, all antibiotics 30 days prior to index test, DOT per 1000 days present618 (200–1000)800 (266–1167)0.14 * Select antibiotics: cefepime, ceftriaxone, piperacillin-tazobactam, ciprofloxacin, and levofloxacin; all antibiotics: any antibiotic used within the specified time; DOT= days of therapy; AU= antibiotic use; PPI= protein pump inhibitor
Discussion
This study found no association between inappropriate AU and HO-CDI. This result was unexpected given available data regarding CDI and AU. A 2014 meta-analysis found that exposure to antibiotics was associated with a 60% increased risk of CDI.^ 7 ^ A retrospective chart review of antibiotic courses prior to HO-CDI at two academic tertiary acute care hospitals in Ontario, Canada, found 45.5% of antibiotic courses were inappropriate.^ 4 ^ Another study of inpatient AU found that 56% of patients had AU that was not supported by clinical data.^ 8 ^
This study found inappropriate AU in 24% of cases and 26% of controls. This frequency of inappropriate AU is lower than other studies have reported. In studies by Srigley et al^ 4 ^ and Magill et al,^ 8 ^ inappropriateness categories were similar to those of our study. Clinical guidelines were used to identify AU that was not needed, was given longer than is recommended, or covered a wider spectrum of bacteria than is recommended. Those studies reviewed patients from 2011–2012 and 2015 and did not report frequency of ID consultation. Progress in antimicrobial stewardship practices since 2015,^ 9 ^ as well as frequent ID consultation in our population, might contribute to the finding of less inappropriate AU in our study.
Conflicting with prior studies, our control group had significantly higher rates of AU for five high-risk antibiotics compared to cases. However, the analysis of all antibiotics given prior to the index test showed no significant difference. Control selection might have contributed to this finding. C. difficile tests are typically ordered for patients with prior AU. Selection based on C. difficile orders may bias the control group toward a higher proportion of patients with antibiotic exposure compared to a random sample of admitted patients. Studies assessing AU and CDI should consider inclusion of a control group with no history of CDI test. Another reason for this unexpected result may be the lack of data on AU from outside institutions. Alternatively inappropriate AU might not be a key driver of HO-CDI in our institution. Infection control practices or patient colonization might also be important factors.^ 1 ^
Limitations of this study include its retrospective design, limited sample size, matching, and subjective judgment in determining appropriateness of AU. Matching can limit the potential for bias due to confounding but cannot eliminate it. The use of patient location in matching was intended to maintain similarities between the groups in broad categories such as oncology or critical care. With this strategy, we could not identify two controls for every single case. Matching on more specific patient characteristics might have increased similarity between the groups but would have made it more difficult to match controls to cases. Although identification of “appropriate AU” was based on clinical judgment, questionable cases were adjudicated by additional investigators. One strength of our study was detailed review of patient charts to determine appropriateness of AU in addition to reporting overall AU rate. Another strength is the applicability of our study to hospitals that serve a population with a substantial proportion of Black and Hispanic patients.^ 10 ^
In conclusion, this study did not find more inappropriate or total AU in HO-CDI cases compared to CDI negative controls. This finding may reflect advances in antimicrobial stewardship practices, frequent ID consultation in our institution, or the choice of control group in the study. Nevertheless, opportunities remain for overall reduction in inappropriate AU.
Supporting information
10.1017/ash.2025.10161.sm001John et al. supplementary materialJohn et al. supplementary material
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kociolek LK , Gerding DN , Carrico R , et al. Strategies to prevent Clostridioides difficile infections in acute-care hospitals: 2022 update. Infect Control Hosp Epidemiol 2023; 44:527– 549.37042243 10.1017/ice.2023.18PMC 10917144 · doi ↗ · pubmed ↗
- 2FA Qs: Multidrug-Resistant Organism & Clostridioides difficile Infection (MDRO & CDI). US Centers for Disease Control and Prevention. https://www.cdc.gov/nhsn/faqs/faq-mdro-cdi.html. Published 2023. Accessed September 22, 2023.
- 3Guh AY , Mu Y , Winston LG , et al. Trends in U.S. Burden of Clostridioides difficile infection and outcomes. N Engl J Med 2020; 382:1320– 1330.32242357 10.1056/NEJ Moa 1910215 PMC 7861882 · doi ↗ · pubmed ↗
- 4Srigley JA , Brooks A , Sung M , Yamamura D , Haider S , Mertz, D . Inappropriate use of antibiotics and Clostridium difficile infection. Am J Infect Control 2013; 41:1116–1118.23932828 10.1016/j.ajic.2013.04.017 · doi ↗ · pubmed ↗
- 5National Healthcare Safety Network. Multidrug-resistant organism & Clostridioides difficile infection (MDRO/CDI) module. US Centers for Disease Control and Prevention. https://www.cdc.gov/nhsn/pdfs/pscmanual/12pscmdro_cdadcurrent.pdf. Published 2025. Accessed June 16, 2025.
- 6Spivak ES , Cosgrove SE , Srinivasan A. Measuring appropriate antimicrobial use: attempts at opening the black box. Clin Infect Dis 2016; 63:1639– 1644.27682070 10.1093/cid/ciw 658PMC 6487652 · doi ↗ · pubmed ↗
- 7Slimings C , Riley TV. Antibiotics and hospital-acquired Clostridium difficile infection: update of systematic review and meta-analysis. J Antimicrob Chemother 2014; 69:881– 891.24324224 10.1093/jac/dkt 477 · doi ↗ · pubmed ↗
- 8Magill, SS , O’Leary, E , Ray, SM , et al. Assessment of the appropriateness of antimicrobial use in US hospitals. JAMA Netw Open 2021; 4:e 212007.33734417 10.1001/jamanetworkopen.2021.2007 PMC 7974639 · doi ↗ · pubmed ↗