Incidence of local complications following implementation of alcoholic chlorhexidine for peripheral venous catheter site disinfection
Ventsislava Berg, Martin Nufer, Michaela Gligor, Christina Orasch, Rami Sommerstein

TL;DR
Using alcoholic chlorhexidine for catheter site disinfection did not significantly change local skin complication rates in real-world practice.
Contribution
Real-world validation of chlorhexidine's infection prevention without increasing skin complications.
Findings
CHG disinfection did not increase local skin complications.
Implementation of CHG showed no major change in complication incidence.
Real-world application confirmed controlled study benefits without new risks.
Abstract
A previous controlled study showed advantages of 2% Chlorhexidine Gluconate-Alcohol (CHG) over Povidone-Iodine-Alcohol in preventing infections after peripheral venous catheter placement. We applied these findings in a real-world before/after healthcare intervention and found that introduction of CHG disinfection was not associated with a major change of incidence in local skin complications.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
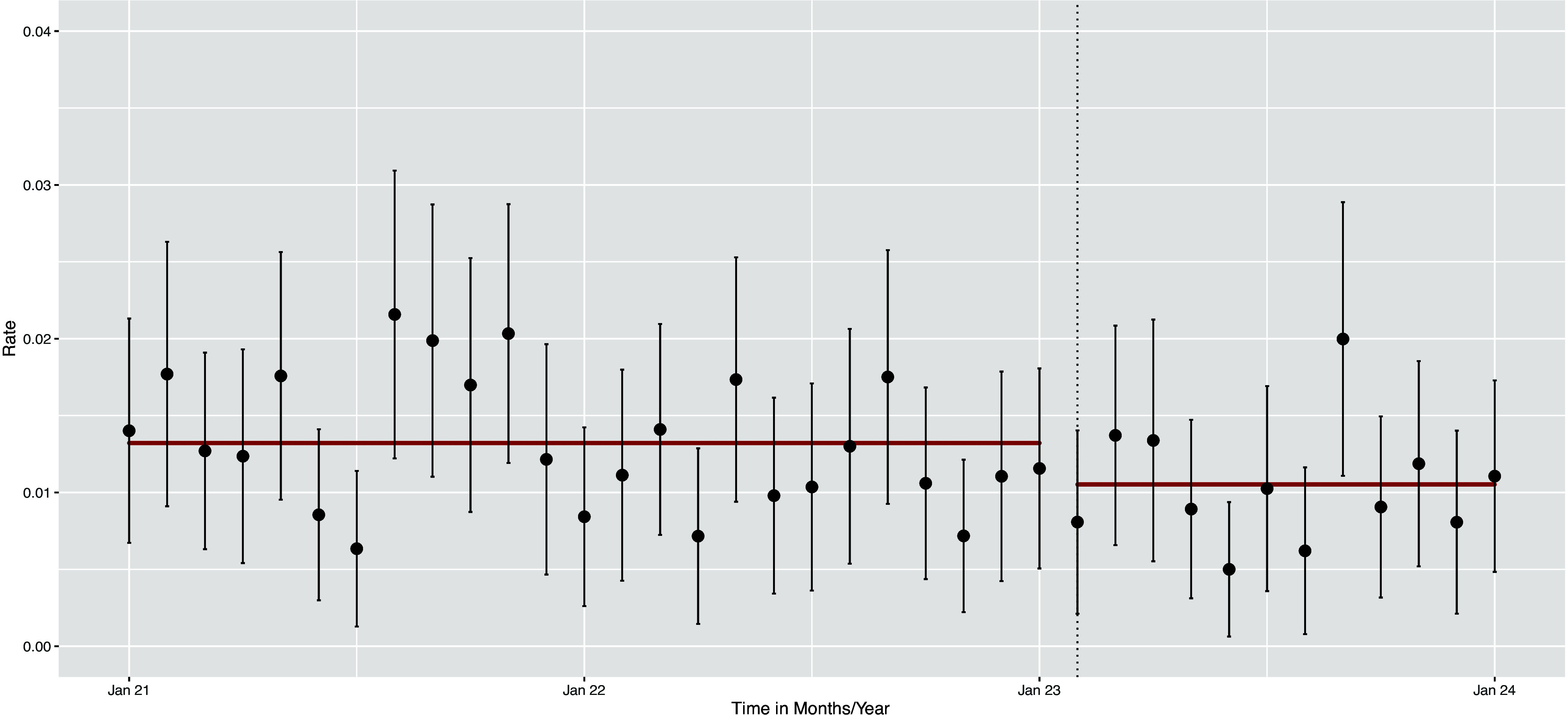 Figure 1
Figure 1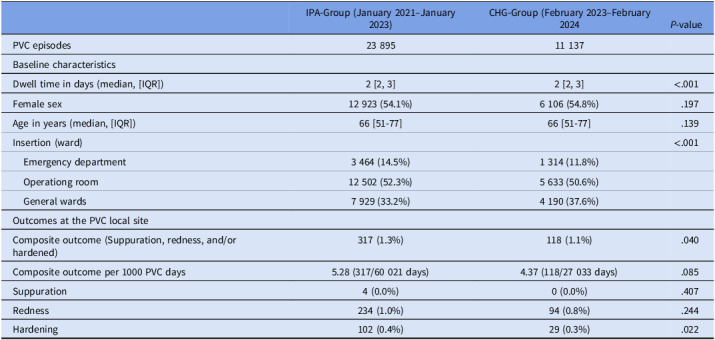 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCentral Venous Catheters and Hemodialysis · Medical Device Sterilization and Disinfection · Intravenous Infusion Technology and Safety
Introduction
Peripheral venous catheters (PVCs) are the most commonly used invasive devices in hospital settings, with up to 70% of hospitalized patients receiving a PVC^ 1 ^ and approximately 2 billion PVCs sold worldwide annually.^ 2 ^ While generally considered low-risk devices, PVCs can occasionally lead to serious adverse events, including mechanical, vascular, and infectious complications.
Research on strategies to reduce PVC-associated local complications has identified several risks: Key factors influencing complication rates include hand hygiene compliance, vein selection, puncture technique, skin disinfection, and regular inspection of the insertion site.^ 3,4 ^ Among available skin disinfectants, chlorhexidine stands out as a broad-spectrum antibacterial agent effective against both Gram-positive and Gram-negative bacteria, with additional activity against yeasts and dermatophytes.^ 5 ^
Previous studies have demonstrated that 2% chlorhexidine gluconate in 70% alcohol (CHG) outperforms other alcohol-based disinfectants in reducing infection-related complications.^ 6 ^ Our study aimed to evaluate whether implementing CHG as a routine disinfectant in a real-world setting would impact local PVC site complication rates.
Methods and findings
Study setting and intervention
Prior to 2023, the tertiary care hospital St. Anna (Lucerne, Switzerland) used isopropanol alcohol (IPA) as the standard skin disinfectant for PVC insertion. On February 1, 2023, following recommendations from the hospital hygiene department, all existing Kodan® forte bottles (containing isopropyl alcohol, propanol, and 2-phenylphenol) were replaced with Softasept® chlorhexidine 2% solution. This transition was preceded by staff communication, updates to standard operating procedures, and appropriate training.
Monitoring and documentation
The nursing staff maintained consistent, prospective monitoring practices throughout both periods, documenting local findings as long as the PVC was in place (suppuration, redness, vein hardening) three times daily in the electronic health record system. Individual PVC episodes were recognized and defined through specific attributes such as insertion and removal data; side (left vs right); as well as anatomic position (eg, wrist, forearm, cubital fossa). Postremoval PVC surveillance was by definition not possible. Ward of insertion was recorded as well in the data set—all PVC inserted outside the institution were excluded from the study.
The hospital hygiene staff conducted periodic checks to ensure proper implementation and documentation. Check on the implementation of disinfectant distribution and use was not performed pre intervention, as CHG was not available for PVC site disinfection in the designated wards.
Statistical analysis
We compared patient characteristics and outcome rates between the two periods using χ ^2^ tests for categorical data and Wilcoxon tests for continuous data. The primary outcome was a composite of local complications (redness, suppuration, and hardening). Sensitivity analysis included the composite redness and suppuration only, which can be viewed as a more reliable marker of possible PVC infection. We calculated the crude PVC outcome rate per 1 000 lay days, as well as the incidence rate ratio using Poisson regression, analyzing monthly complication rates before and after the intervention. Statistical significance was set at P < .05, using R version 4.1.2.
This quality assurance study was exempt from ethical review under Swiss law. According to the Swiss Human Research Act, quality assurance and quality control studies are classified as basic research activities protected under Article 20 of the Federal Constitution of the Swiss Confederation. Such studies do not require prior regulatory approval.
Results
Study population
After exclusion of 667 PVC inserted outside the institution, our analysis included 35,032 PVC episodes: 23 895 in the IPA group (January 2021–January 2023) and 11,137 in the CHG group (February 2023–January 2024). Both groups (Table 1) showed statistically not significantly different patient characteristics: Median PVC dwell time: 2 days in both groups. Sex distribution was 54.1% women (IPA) versus 54.8% (CHG) and the median age: 66 [IQR 51–77] years (IPA) versus 66 [IQR 51–77] years (CHG).
Table 1.Baseline characteristics and outcomes (composite and single events) per study periodIPA-Group (January 2021–January 2023)CHG-Group (February 2023–February 2024 P-valuePVC episodes23 89511 137Baseline characteristicsDwell time in days (median, [IQR])2 [2, 3]2 [2, 3]<.001Female sex12 923 (54.1%)6 106 (54.8%).197Age in years (median, [IQR])66 [51-77]66 [51-77].139Insertion (ward)<.001 Emergency department3 464 (14.5%)1 314 (11.8%) Operationg room12 502 (52.3%)5 633 (50.6%) General wards7 929 (33.2%)4 190 (37.6%)Outcomes at the PVC local siteComposite outcome (Suppuration, redness, and/or hardened)317 (1.3%)118 (1.1%).040Composite outcome per 1000 PVC days5.28 (317/60 021 days)4.37 (118/27 033 days).085Suppuration4 (0.0%)0 (0.0%).407Redness234 (1.0%)94 (0.8%).244Hardening102 (0.4%)29 (0.3%).022
Primary outcome
The composite outcome rate of local complications for the IPA group was 317/23 895 (1.3%) PVC episodes and in the CHG group 118/11 137 (1.1%) PVC episodes (P = .040). Per PVC days, the crude rate for the composite outcome was 5.28/1 000 lay days and 4.37/1 000 for CHG (P = .085).
The detailed comparison of individual outcomes are listed in Table 1.
The incidence rate ratio after CHG implementation was 0.80 (95% CI, 0.64–0.98; P = .037), indicating a statistically significant reduction in complications (Figure 1).
Figure 1.Incident rates per month with 95% CI and trendline per period (before/after intervention).
In the sensitivity analysis (Supplementary Table and Supplementary Figure) focussing on the outcome suppuration and redness only, the IRR was 0.86 (95% CI 0.67–1.09, P = .21)
Discussion
Our findings demonstrate that switching from IPA to CHG was associated with a marginally statistically significant reduction in local PVC complications, aligning with previous clinical trial data on CHG efficacy^ 3,8 ^. Taking into consideration the results of the sensitivity analysis, the statistically nonsignificant difference in the rate of outcome/1 000 PVC days and several limitations associated with this before/after study, our careful interpretation is, that the introduction of CHG disinfection was not associated with a major change of incidence in local skin complications.
While nursing adherence to insertion site monitoring was not directly measured, the consistent monthly PVC rates suggest stable compliance throughout the study period. To the best of our knowledge, there was no substantial change in other prevention methods throughout the study period, such as staff education on proper insertion, hand hygiene compliance, and sterile dressing options. Accordingly, we do not expect significant confounding due to other prevention methods introduced throughout the study period.
Study limitations include: i) Confounding by the study design (active change to a potentially better disinfectant with more allergies may lead to under/overreporting of outcomes); ii) inability to link microbiological results and mortality data due to separate database systems: these markers could have represented stronger biological correlation of poor or limited skin antisepsis; iii) lack of knowledge of concomitant antimicrobial therapy that may occult PVC outcomes (even though we do not believe, this is an effect modifier); iv) the role of the COVID pandemic and other time-dependent changes in infection-prevention practice that may have confounded results; and v) potential limitations in generalizability to facilities with different service ranges or microbial spectra.
Conclusion
The implementation of CHG as the standard skin disinfectant was not associated with a major change of incidence in local skin complications in our before/after healthcare intervention. We rather consider the result or our study as hypothesis-generating than practice changing.
Supporting information
10.1017/ash.2025.10170.sm001Berg et al. supplementary materialBerg et al. supplementary material
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Zingg W , Pittet D. Peripheral venous catheters: an under-evaluated problem. Int J Antimicrob Agents 2009;34 Suppl 4:S 38–42.19931816 10.1016/S 0924-8579(09)70565-5 · doi ↗ · pubmed ↗
- 2Rickard CM , Marsh N , Webster J , et al. Dressings and securements for the prevention of peripheral intravenous catheter failure in adults (SAVE): a pragmatic, randomised controlled, superiority trial. The Lancet 2018;392:419–30.10.1016/S 0140-6736(18)31380-130057103 · doi ↗ · pubmed ↗
- 3Guenezan J , Marjanovic N , Drugeon B , et al. Chlorhexidine plus alcohol versus povidone iodine plus alcohol, combined or not with innovative devices, for prevention of short-term peripheral venous catheter infection and failure (CLEAN 3 study): an investigator-initiated, open-label, single centre, randomised-controlled, two-by-two factorial trial. Lancet Infect Dis 2021;21:1038–48.33539734 10.1016/S 1473-3099(20)30738-6 · doi ↗ · pubmed ↗
- 4Buetti N , Abbas M , Pittet D , et al. Comparison of routine replacement with clinically indicated replacement of peripheral intravenous catheters. JAMA Intern Med 2021;181:1471–1478.34533191 10.1001/jamainternmed.2021.5345 PMC 8561330 · doi ↗ · pubmed ↗
- 5Mc Donnell, GE. Antisepsis, Disinfection, and Sterilization: Types, Action, and Resistance. Washington, DC: ASM Press; 2007.
- 6Adams D , Quayum M , Worthington T , Lambert P , Elliott T. Evaluation of a 2% chlorhexidine gluconate in 70% isopropyl alcohol skin disinfectant. J Hosp Infect 2005;61:287–290. 10.1016/j.jhin.2005.05.015 16221509 · doi ↗ · pubmed ↗
- 7Standard Operating Procedere. Instructions for nursing/medical technology nursing/venous access (SOP Peripheral venous catheters (PVK)/ Venflon, Version 4/15.11.2023). Klinik St. Anna, Lucerne, Switzerland.
- 8Small H , Adams D , Casey AL , Crosby CT , Lambert PA , Elliott T. Efficacy of adding 2% (w/v) chlorhexidine gluconate to 70% (v/v) isopropyl alcohol for skin disinfection prior to peripheral venous cannulation. Infect Control Hosp Epidemiol 2008: 29;963–965.18771405 10.1086/590664 · doi ↗ · pubmed ↗