Prevalence, Intensity, and Risk Factors of Schistosoma mansoni and Other Intestinal Parasites: A Cross-Sectional Study in Rural Agricultural Communities of Lango Subregion, Uganda
John Paul Byagamy, Robert Opiro, Margaret Nyafwono, Geoffrey Maxwell Malinga, Richard Echodu, Emmanuel Igwaro Odongo-Aginya

TL;DR
This study examines the spread and risk factors of Schistosoma mansoni and other intestinal parasites in rural Uganda, finding age and location as key contributors.
Contribution
The study provides new local epidemiological data on schistosomiasis and intestinal parasites in the Lango subregion of Uganda.
Findings
Schistosoma mansoni was the most prevalent parasite, affecting 21.2% of participants.
Age and subcounty location were significant risk factors for S. mansoni infection.
The study identified the need for targeted interventions to reduce infection rates in high-risk areas.
Abstract
In developing countries such as Uganda, intestinal parasitic infections and schistosomiasis remain a serious threat to public health. Local epidemiological data are critical for the prevention and control of the disease. This study was aimed at determining the prevalence, intensity, and risk factors of schistosomiasis and other intestinal parasite infections among rural agricultural communities in the Lango subregion, northern Uganda. A cross-sectional study was carried out in Lira city, Kole, and Lira district in the Lango subregion, northern Uganda, involving 438 participants aged between 5 and 85 years. Urine and stool samples were collected and examined for parasites using urine circulating cathodic antigen (POC-CCA), filtration methods, and the Odongo-Aginya technique. Information on sociodemographic factors and other predisposing factors to infections was obtained using…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
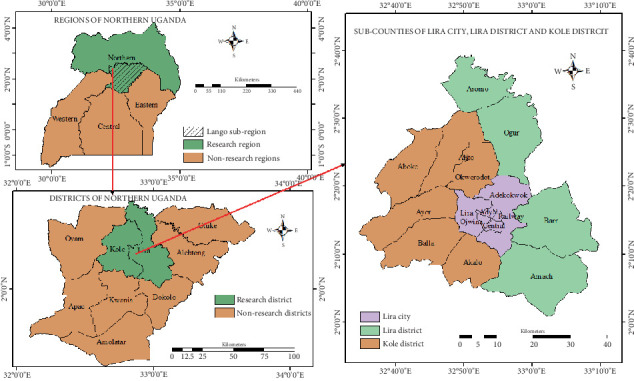 Figure 1
Figure 1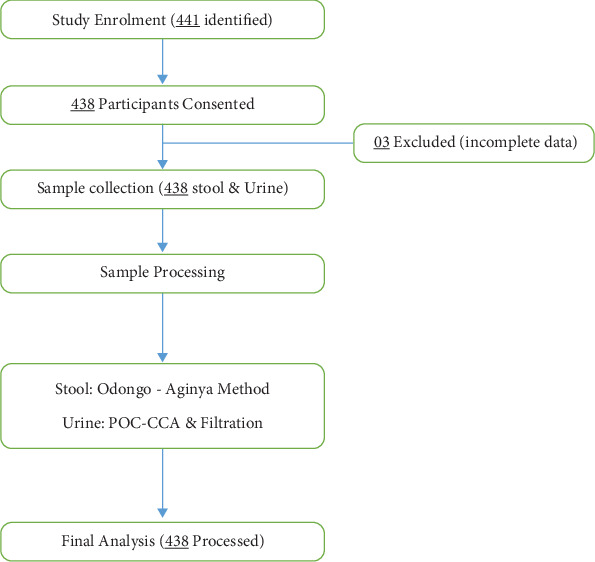 Figure 2
Figure 2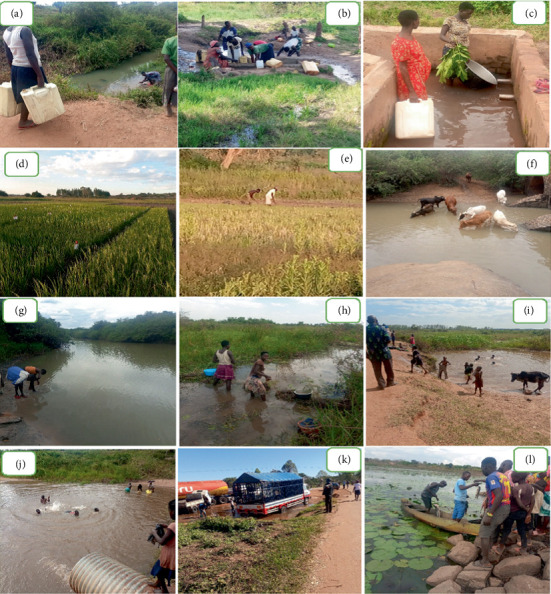 Figure 3
Figure 3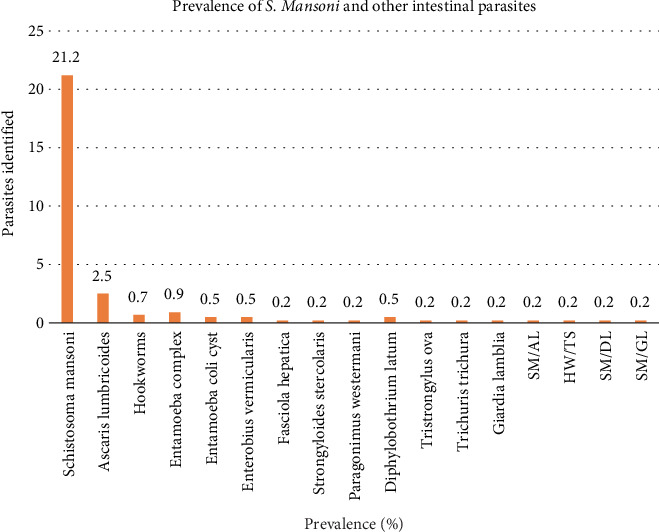 Figure 4
Figure 4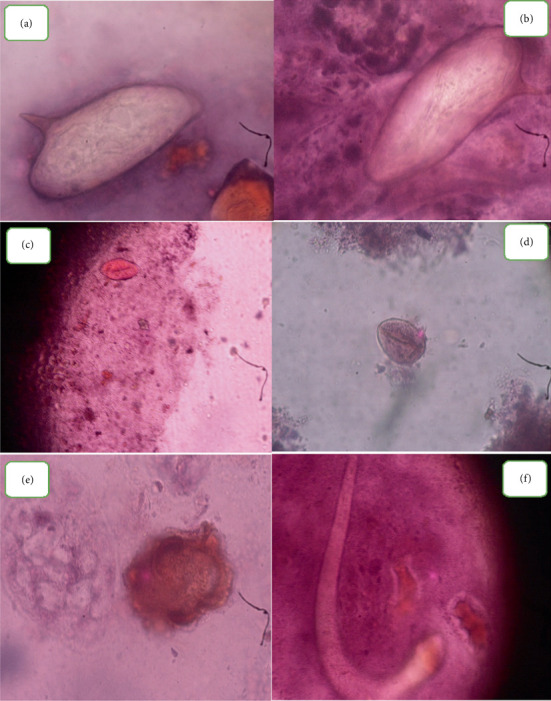 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFood Security and Health in Diverse Populations
1. Background
Human schistosomiasis (bilharziasis) is a water-borne parasitic disease caused by schistosomes and transmitted by snail intermediate hosts mainly of the genera Biomphalaria and Bulinus species [1]. Globally, it is estimated that about 252 million people are infected with Schistosoma species in 78 tropical countries and that 500–600 million people are at risk of infection [2]. Out of over 200 million cases of infection in a year, 120 million are symptomatic and 20 million have severe debilitating disease [3, 4]. The disease is commonly found in tropical countries with permanent water bodies infested with freshwater snail intermediate hosts that contain the infective cercariae in Asia, Africa, and South America [4, 5]. Both intestinal and urinary schistosomiasis cause acute and chronic diseases [4]. Infections occur during water contact activities along the permanent water bodies and in people engaged in domestic, agricultural, and recreational activities, which expose them to cercarial-infested water [6]. Recent estimates indicate that at least 290.8 million people require praziquantel treatment for schistosomiasis. However, only 97.2 million have been treated [7, 8]. The World Health Organization (WHO) has embarked on the elimination of schistosomiasis as a public health problem in endemic countries in a roadmap from 2021 to 2030 [9].
In sub-Saharan Africa, recent estimates reveal that 54 million people are currently infected with Schistosoma mansoni, causing blood in stool in 4.4 million, hepatomegaly in 8.5 million, and an annual mortality of 130,000 people [10]. Agricultural activities, mainly in areas of water resource development like irrigation fields and the construction of dams, have encouraged the spread of the disease [11, 12]. These project areas are suitable habitats for snail intermediate hosts shedding the cercariae, which are the infective stages of the parasite [11, 12]. A typical example of irrigation schemes' role in the transmission of schistosomiasis is in Egypt and Sudan, where the prevalence of periportal fibrosis is considerably high at 79.3% compared with countries such as Kenya and Mali, where the prevalence of periportal fibrosis is markedly low at 27.5% and 23.6%, respectively [13].
In Uganda, schistosomiasis causes high morbidity and mortality in most communities, especially along the lakeshores and river banks [4, 14, 15]. It is the second most significant disease in terms of public health impact and socioeconomic burden, following malaria [16, 17], causing both intestinal and urinary complications that significantly affect the quality of life [4, 18]. Countrywide, 81 districts and an estimated 5.4 million people are affected, with 14.7 million at risk of the infection [18]. The disease mainly affects the rural poor, especially peasant farmers. Infections do occur also among people living in urban or periurban settings [4, 19]. The WHO introduced the mass drug administration (MDA) in Uganda in 2003 as a way of reducing morbidity and mortality due to schistosomiasis in affected communities [19–22]. Despite this intervention, the prevalence is still high (more than 50%) among school children and rural communities [4, 23]. This group of people generally has low socioeconomic status with poor sanitation and limited access to clean water. Their main sources of income are fishing in the lakes or the rivers, swamps, dams, farming, and collection of water from these water bodies and, as a result, exposing them to infections [4, 19]. Furthermore, while schistosomiasis is a major focus of disease control programs, coinfection with intestinal parasites such as Ascaris lumbricoides, Trichuris trichiura, and hookworms, as well as Entamoeba species, is also widespread in the country [24, 25], with prevalence reaching as high as 90%, especially among children and rural communities with poor sanitation [4, 18]. These infections often share similar risk factors, including poor sanitation, contaminated water sources, and low socioeconomic status [26]. Coinfections with intestinal parasites can impact schistosomiasis treatment outcomes by altering immunological responses, contributing to malnutrition, anemia, and overall morbidity [27]. Individuals harboring multiple parasitic infections may respond differently to praziquantel and other anthelmintic therapies, necessitating an integrated approach to disease control [28].
The Lango subregion is known to be one of the areas harboring both Schistosoma haematobium and S. mansoni in Uganda [4, 24]. However, while previous studies have extensively documented S. mansoni prevalence in Uganda [4], there is a paucity of information concerning the actual magnitude of the disease and specific risk factors for infection in the subregion. Yet this kind of information is necessary to guide the prevention, control, and possibly elimination of the disease as suggested by WHO [4] and Adriko [9]. Furthermore, there is limited recent data on the burden of nonschistosome intestinal parasites in specific regions such as the Lango subregion [29]. Understanding their prevalence alongside schistosomiasis is crucial for designing comprehensive interventions that address multiple parasitic infections simultaneously.
This study is aimed at determining the prevalence, intensity, and risk factors of S. mansoni and other intestinal parasitic infections among rural agricultural communities in the Lango subregion of northern Uganda. By investigating both schistosomiasis and coendemic intestinal parasites, this study seeks to fill gaps in current epidemiological data and provide insights into how these infections interact within affected populations. The findings will inform targeted public health interventions, improved treatment strategies, and more effective control measures to reduce the burden of parasitic diseases in Uganda.
2. Materials and Methods
2.1. Study Area
The study was conducted in Lira (2°14′50.0^″^N 32°54′00.0^″^E) and Kole (2°23′59.99^″^N 32°47′59.99^″^E) districts in the Lango subregion, northern Uganda [30]. These districts are among the nine districts in the Lango subregion, predominantly inhabited by the Lango tribe (Figure 1). The study areas of Lira city, Kole, and Lira districts were selected due to their varied agroecological profiles, high agricultural activity, and historical burden of both S. mansoni and S. haematobium, making them representative of rural settings within the Lango subregion [30]. The main economic activities are commercial and subsistence farming, small-scale fishing, retail and wholesale business, and a commercial center for northern Uganda and the Lango subregion [30]. The area is characterized by a tropical type of climate with an average rainfall of 1500 mm, with the least received in January and the maximum in May [31]. There are two rainy seasons, April to May and August to November every year [31]. Temperature varies between 65°F and 95°F [31]. The dry seasons range from December to March and from June to August. Approximately 30% of the land area is covered by freshwater bodies like rivers, permanent and seasonal swamps, and wetlands. These water bodies are potential sources of infection for S. mansoni and S. haematobium, as they harbor numerous snail intermediate hosts [31]. The communities use these water bodies for different domestic purposes. The estimated total population of the Lango subregion is 2,513,700 people [32].
2.2. Study Design
The study was cross-sectional, targeting rural communities of Lango subregion, northern Uganda, to assess the prevalence of intestinal parasites, infection intensity, and risk factors of schistosomiasis. Participants were drawn from rural community members, especially farmers in wetlands, irrigation schemes, dams, and car washers, and screened for both S. mansoni and S. haematobium. Participants were subjected to both stool and urine examinations to detect and identify the schistosome eggs and other intestinal parasites.
2.3. Study Population
The target population comprised selected community members aged 5–85 years and all persons exposed to water containing snail vectors who were involved in washing clothes, wetland farming, rice fields, water collection for domestic use, and swamp car washers in all the selected districts in the Lango subregion.
2.4. Sample Size Determination
The sample size was calculated using the formula described by Lwanga [33]. N = Z^2^ × PQ/d^2^, where N is the desired sample size, P is the estimated prevalence, estimated to be 50%, Q is the percentage of people not infected (1 − p), d is the degree of precision required, usually set at 0.05, and Z is the confidence limit at 95% interval (1.96).
Substituting in the above formula, N = (1.96^2^ × 0.5 × (1–0.5) = 384.16 ≈ 384)/±0.05^2^.
However, after accounting for a 15% nonresponse rate, the final calculated sample size was 441, although only 438 participants provided both urine and stool samples.
2.5. Sampling Techniques
The study used a multistage sampling procedure to select representative sample sizes in the study. Three out of nine districts were selected randomly using a lottery method, followed by five subcounties, 10 parishes, and 2–3 villages. Finally, the selected villages were then surveyed for urine and stool samples obtained from 438 community members involved in water contact activities. Questionnaires were administered to the consented participants, ensuring a comprehensive understanding of the community's water use (Figure 2).
2.6. Stool and Urine Collection, Processing, and Examination
Only consented participants were provided with stool containers, well labeled with the participant's code, laboratory number, date, and time of sample collection. Each participant was instructed to collect an equivalent of 10 g of stool in the morning between 8 and 10 a.m. and deliver it to the laboratory within 1 h after the specimen collection. The stool specimens were processed using the Odongo-Aginya method (compound stain: consisting of 5% eosin yellow in 10% formalin mixed 1:1 with 7.5% nigrosin in 10% formalin) [34]. Cellophane cover slips cut in 25 × 40 mm pieces were presoaked in 50% glycerin [34].
Stool specimens were strained through a sieve, cleaned, and placed on a microscope slide through a template measuring 41.7 mg. A compound stain was added, and a cellophane cover slip was blotted out. The slide was then examined under a light microscope to identify and quantify Schistosoma eggs and other intestinal parasites based on their morphological characteristics, following WHO guidelines and using the Odongo-Aginya method [34]. Specimen processing and examination were done at the Lira Regional Referral Hospital (LRRH) laboratory, and the slides were read by two qualified technicians and re-examined by a senior laboratory technologist for quality control [34]. Urine was collected using well-labeled sterile containers with participant's ID codes. Twenty to 30 mL of freshly voided urine was collected from each participant between 10 a.m. and 2 p.m. and tested within 1 h of collection at LRRH laboratory [35]. The study used a commercial antigen test kit called point-of-care circulating cathodic antigen assay (POC-CCA) to measure the CCA levels of juvenile and adult S. mansoni in the urine [36]. The test was performed and reported according to the manufacturer's instructions. The tests were interpreted by lab technicians independently to accurately assess the infection prevalence [36].
The urine filtration technique was also employed to examine and quantify S. haematobium in urine [37] by experienced laboratory technicians in the LRRH laboratory. A 10-mL syringe with a Swinney filter holder of 13-mm diameter and polycarbonate membrane filter was employed to recover the eggs of S. haematobium in urine and placed on a glass slide, examined using a light microscope at ×40 objective lens [37]. Samples found to have eggs were recorded as positive and the number of eggs counted to determine the intensity (Figure 2). Those found to be positive were treated with praziquantel 40 mg/kg body weight free of charge [38].
2.7. Risk Factors for Schistosoma Infection
Consenting community members involved in any water contact activities were interviewed using a pretested questionnaire to collect the demographic and sociocultural information and other associated risk factors for S. mansoni infection (Figure 3). The factors investigated included education level, employment status, income level, socioeconomic activities, water contact activities, home distance from the water source, frequency, and length of exposure to an open water source and sources of domestic water.
2.8. Data Analysis
The data was analyzed using SPSS Version 25.0 [39]. A Pearson's chi-square test, binary, and multivariable logistic regressions were performed to assess the association between variables. The odds ratios (ORs) with 95% confidence intervals were used to measure the strength of associations. p values < 0.05 were considered statistically significant. The intensity of S. mansoni infection was calculated using WHO guidelines [37], which classify infections into light, moderate, and heavy classes.
3. Results
3.1. Sociodemographic Characteristics of Study Subjects
A total of 438 participants aged 5–85 were enrolled in the study. Out of these, 193 (44.1%) were males and 245 (55.9%) were females. The mean age of participants was 38.9 ± 15.1 years (mean ± standard deviation), with the majority, 150 (34.4%), being younger than 30 years old (Table 1). The majority of participants, 373 (85.2%), were farmers, 292 (66.7%) had a primary level of education, 234 (53.4%) lived less than 500 m from a water source, and the two most common sources of domestic water were piped water, 180 (41.1%), and boreholes, 104 (23.7%) (Figure 3). The major reasons for water contact were farming, 287 (65.5%), and fetching water for domestic use, 53 (12.1%) (Table 1). S. mansoni prevalence among participants was significantly associated (p < 0.05) with age, location, occupation, education level, source of domestic water, and contact with open water sources (Table 1).
3.2. Prevalence of S. mansoni and Other Intestinal Parasites
The overall prevalence of intestinal parasites including S. mansoni was 27.4% (120/438). S. mansoni had the highest prevalence of 21.2% (93/438). However, the prevalence of other intestinal parasites was low: Ascaris lumbricoides (2.5%); Entamoeba complex (0.9%); hookworms (0.7%); Entamoeba coli, Enterobius vermicularis, and Diphyllobothrium latum (D. latum) with 0.5%, respectively; and Trichuris trichiura, Fasciola hepatica, Giardia lamblia, Strongyloides stercoralis, Paragonimus westermani, and Trichostrongylus ova (0.2%) (Figures 4 and 5). There was a low prevalence of mixed infection with single incidences of each of S. mansoni/Ascaris lumbricoides, S. mansoni/D. latum, S. mansoni/Giardia lamblia, and hookworms*/Trichostrongylus ova* (Figure 4). S. haematobium was not detected in this study.
3.3. Intensity of Infection With S. mansoni in the Study Area
The intensity of infection was calculated based on WHO grading of eggs per gram (EPG) as light, moderate, and heavy as 1–99, 100–399, and > 400 EPG, respectively [32]. The heavy intensity of infection was found in a single female in the age group of 17–20 years with a mean egg count of 480 EPG (Table 2). The majority of the participants had low to moderate intensity of infection with mean egg counts ranging between 72–75.4 and 144–187 EPG, respectively (Table 2).
3.4. Risk Factors Associated With S. mansoni Infection
Human water contact activities in these study areas were high. All the participants visited the water bodies at least once a week, either for wetland farming, swimming, fishing, washing clothes, bathing (Figure 2), or fetching water (Table 3). In the univariable binary logistic regression, the age group of participants, subcounty location, and source of domestic water had a p value less than 0.05 and were further analyzed by multivariable logistic regression (Table 3). However, participants who were recruited from the subcounties of Ogur, Aromo, and Barr were 9, 6, and 4 times more likely to get infected with S. mansoni, respectively. Those who fish, ford, swim, and bathe in open water sources were also more likely to get infected with S. mansoni (Table 3). The multiple logistic analysis revealed that the only factors significantly associated with S. mansoni infection were the age of the participant and subcounty location (Table 3). Participants from the Aromo subcounty had two times [AOR = 1.837, 95% CI: 1.274–2.650, p < 0.001] higher odds of infection than those hailing from the Okwerodot subcounty. This could be due to the presence of more water bodies, specific livelihood practices, or local environmental conditions that favor snail habitats. Similarly, participants aged 5–9 years had two times [AOR = 1.448, 95% CI: 1.207–1.737, p < 0.001] higher odds of infection when compared to those above 50 years of age (Table 3). This could be attributed to higher exposure due to economic and domestic activities (e.g., wetland farming and water collection).
4. Discussion
Results indicate that there were high S. mansoni infections (21.2%) in the study area. This is in agreement with the study in high prevalence communities in Uganda 25.6% [40] and Gulu 20.1% [18]. However, the prevalence was lower than those reported from studies in other parts of Uganda, such as 52% in Mayuge [41] and L. Victoria fishing community, 88.6% [42]. The lower prevalence in Lango than in these other areas could be attributed to repeated MDA with praziquantel among the population of the Lango subregion [21], small sample size variations [43], or environmental conditions of the study area as compared to other studies elsewhere [15, 44].
Although S. mansoni was identified in this study area, all urine samples tested negative for S. haematobium despite previous reports pointing to the Lango subregion as harboring the parasite [4, 19, 24, 45]. This could be due to yearly mass treatment campaigns implemented by the Ministry of Health since 2003 [21]. Additionally, climate change and ecological shifts may have contributed to this finding. Climate variability affects Schistosoma transmission by influencing the distribution of intermediate host snails. Rising temperatures, changing rainfall patterns, and habitat degradation may have made the environment less suitable for S. haematobium transmission [44, 46, 47]. This aligns with findings from Codjoe et al. [44], who reported that climate variability significantly impacts the distribution of intermediate host snails, affecting schistosomiasis transmission. Similarly, McCreesh and Booth [46] demonstrated that increasing temperatures can reduce snail survival rates, leading to lower transmission of schistosomiasis. Adekiya et al. [47] further highlighted that changes in water levels and vegetation cover due to climate change have influenced Schistosoma transmission in sub-Saharan Africa.
Furthermore, past intervention strategies may have influenced the observed trends. Sustained MDA efforts in Uganda, particularly in high-endemic areas, have significantly reduced schistosomiasis prevalence. Adriko et al. [21] found that repeated annual praziquantel treatment led to a substantial decline in S. mansoni and S. haematobium infections over time. Similarly, Adriko et al. [48] reported that long-term MDA efforts in Uganda resulted in the near-elimination of S. haematobium from certain regions. Additionally, the WHO [49] emphasized that MDA, combined with water, sanitation, and hygiene (WASH) interventions, has led to significant reductions in schistosomiasis prevalence [49].
Compared to earlier research, the prevalence of other intestinal parasites was very low [50, 51]. This could be due to different interventions undertaken in the study areas, such as repeated biannual MDA of albendazole in schools and the rural communities for the past two decades and health education [19]. Previous studies have demonstrated that improved sanitation, water access, and hygiene education are critical in reducing the burden of intestinal parasitic infections [47, 52].
The intensity of infection with S. mansoni was studied according to WHO classification [37]. There were light, moderate, and heavy infections with S. mansoni among the participants with 66 (72%), 24 (26%), and 2 (2.2%), respectively. However, other studies reported higher infection intensity than the current study [42, 53]. These studies were done before praziquantel's yearly distribution to the study area's community members.
Females were more infected than males, 58.1% and 41.9%, respectively, which agrees with other studies [8, 15]. The high prevalence in females is explained by their more frequent water contact activities than the males, such as wetland farming, fetching water for domestic use, washing clothes, and bathing [15]. Similar to previous studies, we found that infection rates were higher among the 10–16 and 17–20 age groups compared to older individuals, a trend also observed in other research [15, 17]. The significance of this age group's greater involvement in economically generating activities, such as wetland farming, car and motorcycle washing, fetching water for domestic use, fishing, grazing cattle in wetlands, and also bathing in open water sources, might be infested with cercariae.
Our results showed that the age of the participant and subcounty location had significant associations with S. mansoni infections. The geographical location of the study areas contributed to different sources of economic activities. These therefore contributed to the infections; Lira district had the highest number of infections at 74.2%, while the subcounties of Barr (39.8%), Ogur (29.9%), and Bala (10.8%) had higher infection rates with S. mansoni than other subcounties (Table 1). This could be attributed to the numerous freshwater bodies in these localities compared to other study location sites. Lira district has rice irrigation schemes in Abolet, Okile, and Olilo, especially in Barr subcounty [4]. Ogur subcounty has numerous water bodies like Opeta swamp, Akano, Akangi, Obim, and Abongodyang, respectively [4]. Bala subcounty has 30% of the land surface covered with swamps like Onoo, Okwor, Alemi, Okole, Opeta, and Wang Tula, thus harboring numerous snail hosts. This finding is in agreement with previous studies elsewhere [6, 12, 15, 52]. This explains why numerous water bodies contribute to suitable habitats for the snail intermediate host and ease of transmission. Also, the frequent use of unprotected water sources for domestic use predisposes the community to the risk of infection. This concurs with a study conducted in Pader district by Omona et al. [54]. This could be due to the presence of more water bodies, specific livelihood practices, or local environmental conditions that favor snail habitats. Overall, this study highlights the impact of long-term intervention programs, climate variability, and ecological changes on schistosomiasis transmission.
5. Conclusions
This study highlights a high prevalence of S. mansoni in the Lango subregion, with age and subcounty location being major risk factors. Targeted interventions, including ongoing MDA to at-risk population groups and regions, health education, improved sanitation, and access to clean water, are essential for effective control. Community engagement and behavioral change programs can further reduce infection risks. Future research should explore the long-term effects of climate change on parasite ecology and transmission dynamics, as well as the sustainability of MDA programs in schistosomiasis-endemic areas. A multifaceted approach integrating treatment, prevention, and policy-driven strategies is crucial for sustained schistosomiasis control and eventual elimination in affected communities.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bergquist R. Zhou X. N. Rollinson D. Reinhard-Rupp J. Klohe K. Elimination of Schistosomiasis: The Tools Required Infectious Diseases of Poverty 2017611910.1186/s 40249-017-0370-72-s 2.0-8503457724329151362 PMC 5694902 · doi ↗ · pubmed ↗
- 2Rasoamanamihaja C. F. Rakotoarivelo R. A. Edosoa G. Schistosomiasis Elimination in Madagascar: Challenges and Opportunities for Implementing the New WHO Guidelines BMJ Global Health 2023881810.1136/bmjgh-2023-01259837580102 PMC 10432657 · doi ↗ · pubmed ↗
- 3Singh K. Muddasiru D. Singh J. Current Status of Schistosomiasis in Sokoto, Nigeria Parasite Epidemiology and Control 20161323924410.1016/j.parepi.2016.08.0032-s 2.0-8498479482529988177 PMC 5991846 · doi ↗ · pubmed ↗
- 4Adriko M. Tinkitina B. Tukahebw E. M. Standley C. J. Stothard J. R. Kabatereine N. B. The Epidemiology of Schistosomiasis in Lango Region Uganda 60 Years After Schwetz 1951: Can Schistosomiasis Be Eliminated Through Mass Drug Administration Without Other Supportive Control Measures? Acta Tropica 201818541241810.1016/j.actatropica.2018.06.0092-s 2.0-8504930845829935144 · doi ↗ · pubmed ↗
- 5Atalabi T. E. Lawal U. Akinluyi F. O. Urogenital Schistosomiasis and Associated Determinant Factors Among Senior High School Students in the Dutsin-Ma and Safana Local Government Areas of Katsina State, Nigeria Infectious Diseases of Poverty 201651 p. 6910.1186/s 40249-016-0158-12-s 2.0-8500621954327480058 PMC 4969719 · doi ↗ · pubmed ↗
- 6Lund A. J. Rehkopf D. H. Sokolow S. H. Land Use Impacts on Parasitic Infection: A Cross-Sectional Epidemiological Study on the Role of Irrigated Agriculture in Schistosome Infection in a Dammed Landscape Infectious Diseases of Poverty 202110 p. 3510.1186/s 40249-021-00816-5PMC 798327833745442 · doi ↗ · pubmed ↗
- 7Klohe K. Koudou B. G. Fenwick A. A Systematic Literature Review of Schistosomiasis in Urban and Peri-Urban Settings P Lo S Neglected Tropical Diseases 2021152 e 000899510.1371/journal.pntd.0008995 PMC 790640833630833 · doi ↗ · pubmed ↗
- 8Alemayehu B. Tomass Z. Wadilo F. Leja D. Liang S. Erko B. Epidemiology of Intestinal Helminthiasis Among School Children With Emphasis on Schistosoma Mansoni Infection in Wolaita Zone, Southern Ethiopia BMC Public Health 2017171 p. 58710.1186/s 12889-017-4499-x 2-s 2.0-8502090923828633651 PMC 5479011 · doi ↗ · pubmed ↗