Revenue Differences Between Top-Selling Small-Molecule Drugs and Biologics in Medicare
Matthew Vogel, William B. Feldman, Zander Cowan, Benjamin N. Rome, Amitabh Chandra, Aaron S. Kesselheim, Olivier J. Wouters

TL;DR
This study compares how much money drug makers made from top-selling small-molecule drugs and biologics in Medicare over 9 to 13 years after FDA approval.
Contribution
It provides a revenue comparison of drug types eligible for Medicare price negotiations over an extended post-approval period.
Findings
Revenues were analyzed for 9 to 13 years after FDA approval for eligible drugs.
The study covers negotiation-eligible products approved between 2012 and 2022.
It highlights differences in revenue generation between small-molecule drugs and biologics.
Abstract
This study compares the revenues earned by manufacturers 9 vs 13 years following US Food and Drug Administration approval for negotiation-eligible products from 2012 to 2022.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
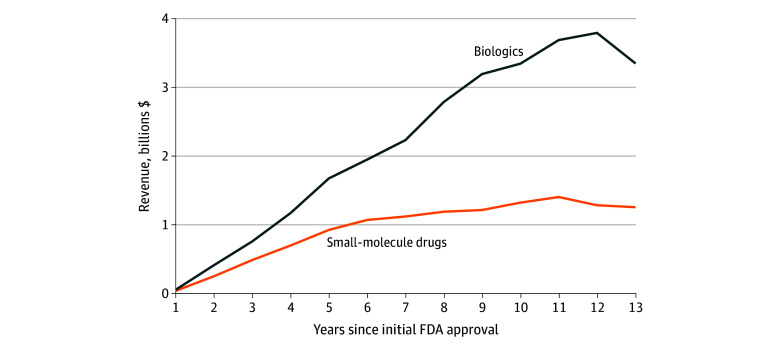 Figure 1
Figure 1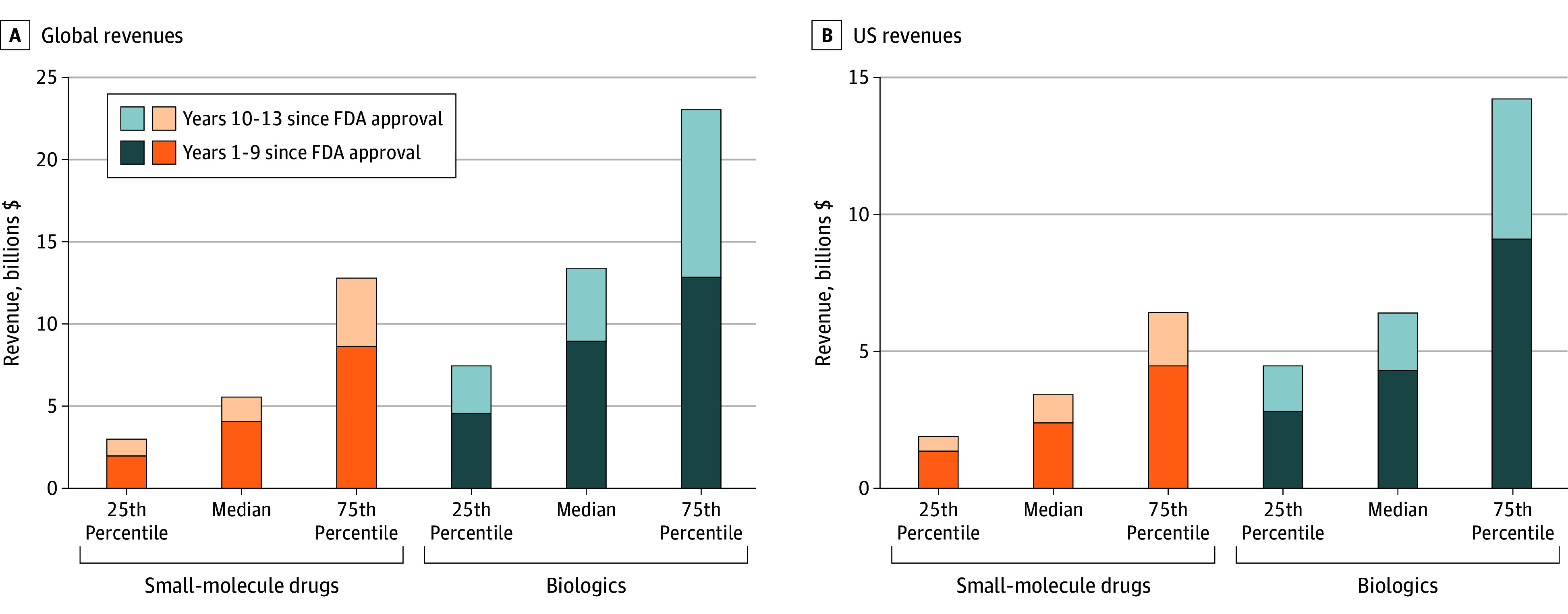 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPharmaceutical Economics and Policy · Health Systems, Economic Evaluations, Quality of Life · Pharmaceutical industry and healthcare
Introduction
The Inflation Reduction Act (IRA) requires Medicare to negotiate prices for certain brand-name drugs with gross annual Medicare spending exceeding $200 million. Small-molecule drugs are exempt from negotiation for 9 years following US Food and Drug Administration approval and biologics for 13 years. The pharmaceutical industry, some members of Congress, and the Trump administration have argued that this difference prioritizes the development of biologics over small-molecule drugs and have proposed aligning the initial eligibility periods for both at 13 years.^1,2^ To inform these policy discussions, we compared the revenues earned by manufacturers after 9 vs 13 years on negotiation-eligible products from 2012 to 2022.
Methods
We retrospectively applied the IRA’s eligibility criteria to Medicare drugs from 2012 to 2022 using the publicly available Medicare drug-spending dashboard.^3^ Following Medicare’s IRA implementation guidance,^4^ we aggregated spending by active moiety or ingredient and identified products meeting the $200 million spending threshold. Using previously described methods,^5^ we excluded products exempt from negotiation (eMethods in Supplement 1).
We obtained 1986-2024 annual US and global sales revenue (net of rebates and discounts) for each negotiation-eligible product from Evaluate Pharma, a third-party data provider (eMethods in Supplement 1). We compared median revenues for biologics and small-molecule drugs using 2-tailed Mann-Whitney U tests (α = .05). We evaluated the economic value of the first 13 years of US and global revenue using a 10.5% discount rate to account for the cost of capital.^1,2,5^ Revenues were inflation adjusted to 2024 dollars.
Institutional review board approval was not required for this study, as no data were collected from human participants. The study followed STROBE reporting guidelines.
Results
From 2012 to 2022, 153 products (122 small-molecule drugs and 31 biologics) met IRA eligibility requirements in at least 1 year and had at least 13 years of revenue data available. Median (IQR) peak annual global revenue was higher for biologics (2.3-1.4 billion [2.8 billion] in year 11) (P < .001; Figure 1).
Median Annual Global Revenues for Products Eligible for Medicare Price NegotiationFDA indicates the US Food and Drug Administration.
After 9 years, the median (IQR) economic value of global revenues was 2.0-9.0 billion (12.8 billion) for biologics; by year 13, these values increased to 3.0-13.4 billion (23.0 billion), respectively (Figure 2). The share of year 1 to 13 economic value earned in years 10 to 13 was 27% for small-molecule drugs and 33% for biologics. For US revenues, the median (IQR) economic value after 9 years was 1.3-4.3 billion (9.1 billion) for biologics; after 13 years it was 2.0-6.1 billion (13.6 billion), respectively (Figure 2).
Economic Value of Global and US Revenues for Top-Selling Biologics and Small-Molecule DrugsFDA indicates the US Food and Drug Administration.
Discussion
In this study, among drugs that met Medicare price negotiation eligibility criteria from 2012 to 2022, biologics generated 7.9 billion more over 13 years. The gap between biologics and small-molecule drugs was larger than reported in previous studies that included less commercially successful products than those eligible for price negotiation.^1,2^ A limitation of this study is that revenues were analyzed retrospectively and do not reflect potential impacts of the IRA on development, commercialization, and pricing decisions, or the timing of generic or biosimilar entry. Additionally, this study does not include an analysis of the relative therapeutic value of different drug modalities.
A prior analysis found higher revenues and clinical trial success rates for biologics than small-molecule drugs and comparable development costs.^1^ The present study further supports the conclusion that biologics, on average, have generated substantially higher revenues than small-molecule drugs by year 9. Implementing negotiated prices later for biologics than for small-molecule drugs may exacerbate this difference, influence industry decisions about which drugs to develop, and limit potential savings from price negotiations. Future research should examine drug revenues alongside development costs and operating expenses to inform optimal timelines for price negotiation.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Wouters OJ, Vogel M, Feldman WB, Beall RF, Kesselheim AS, Tu SS. Differential legal protections for biologics vs small-molecule drugs in the US. JAMA. 2024;332(24):2101-2108. doi:10.1001/jama.2024.1691139585667 · doi ↗ · pubmed ↗
- 2Wouters OJ, Kesselheim AS, Kuha J, Luyten J. Sales revenues for new therapeutic agents approved by the United States Food and Drug Administration from 1995 to 2014. Value Health. 2024;27(10):1373-1381. doi:10.1016/j.jval.2024.06.01538977188 · doi ↗ · pubmed ↗
- 3CMS drug spending. Centers for Medicare & Medicaid Services. Accessed November 20, 2024. https://www.cms.gov/data-research/statistics-trends-and-reports/cms-drug-spending
- 4Medicare Drug Price Negotiation Program: final guidance, implementation of sections 1191-1198 of the Social Security Act for initial price applicability year 2027 and manufacturer effectuation of the maximum fair price in 2026 and 2027. Centers for Medicare & Medicaid Services. October 2, 2024. Accessed September 22, 2025. https://www.cms.gov/files/document/medicare-drug-price-negotiation-final-guidance-ipay-2027-and-manufacturer-effectuation-mfp-2026-2027.pdf
- 5Vogel M, Kakani P, Chandra A, Conti RM. Medicare price negotiation and pharmaceutical innovation following the Inflation Reduction Act. Nat Biotechnol. 2024;42(3):406-412. doi:10.1038/s 41587-023-02096-w 38297186 · doi ↗ · pubmed ↗