Isolated Pancreatic Sarcoidosis Masquerading as Pancreatic Adenocarcinoma: A Case Report
Andrew Mims, Sean Rice

TL;DR
A 50-year-old man was diagnosed with isolated pancreatic sarcoidosis after being initially suspected of having pancreatic cancer.
Contribution
This case report highlights the rare occurrence of isolated pancreatic sarcoidosis mimicking pancreatic adenocarcinoma.
Findings
A pancreatic mass was initially suspected to be adenocarcinoma based on CT and PET scans.
Biopsy results were inconclusive, leading to surgical intervention.
Pathology confirmed granulomatous inflammation consistent with sarcoidosis.
Abstract
A 50-year-old man with no known medical history presented with a four-year history of epigastric pain and weight loss. Computed tomography (CT) revealed a mass in the head of the pancreas concerning for adenocarcinoma. The patient twice underwent endoscopic ultrasound (EUS) with biopsy, with inconclusive results. Positron emission tomography (PET) scan revealed localized disease, concerning for malignancy. With no definitive diagnosis or treatment options, and after multidisciplinary discussion, the patient underwent a Whipple procedure. Pathology revealed granulomatous inflammation of the pancreas and surrounding lymph nodes, consistent with sarcoidosis. Here, we present a rare case of isolated pancreatic sarcoidosis masquerading as pancreatic malignancy in a patient without a known history of sarcoidosis.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1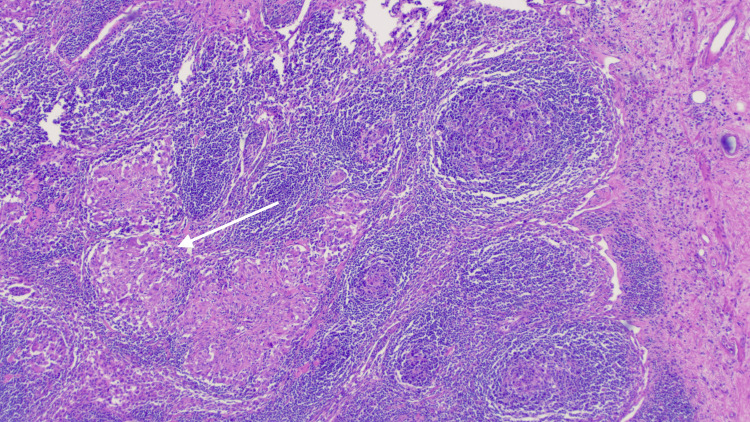 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSarcoidosis and Beryllium Toxicity Research · IgG4-Related and Inflammatory Diseases · Interstitial Lung Diseases and Idiopathic Pulmonary Fibrosis
Introduction
Sarcoidosis is a multisystem, idiopathic disease characterized by granulomatous inflammation. It most commonly affects the lungs; however, any organ can be affected. Symptomatic involvement of the gastrointestinal (GI) tract occurs in less than 1% of cases, and of those, the liver is most commonly involved [1,2]. Pancreatic involvement is exceedingly rare and is usually associated with multiorgan involvement of sarcoidosis. Most cases involving the pancreas are asymptomatic and are discovered on postmortem analysis [3]. The diagnosis of pancreatic sarcoidosis remains difficult, as pancreatic involvement may manifest as direct invasion of the organ, obstruction of the pancreatic or biliary ducts, hepatic lymphadenopathy, or a mimicker of pancreatic adenocarcinoma [4]. Here, we present a rare case of suspected pancreatic malignancy revealed as pancreatic sarcoid after surgical resection, in a patient with no other manifestations of sarcoidosis.
This article was previously presented as a meeting abstract at the 2022 American College of Gastroenterology (ACG) Annual Scientific Meeting on October 24, 2022.
Case presentation
A 50-year-old male with no known past medical history presented to the gastroenterology clinic reporting 3-4 years of epigastric pain radiating to the back with associated 30-pound weight loss.
He initially presented to an outside emergency department. A computed tomography (CT) scan demonstrated a 2.6-cm hyperdense mass-like lesion with infiltrative margins in the pancreatic head and uncinate process with mild biliary and pancreatic ductal dilation, highly suspicious for pancreatic adenocarcinoma (Figure 1). He underwent urgent endoscopic ultrasound (EUS), which further revealed biliary dilatation with a mass in the head of the pancreas. Pathology from fine needle aspiration (FNA) showed rare atypical cells in a background of chronic inflammation, and a neoplastic process could not be excluded. Stains for acid-fast and fungal organisms were negative. With inconclusive results, the patient underwent repeat EUS, which revealed an irregular mass in the pancreatic head. Pathology from the repeat EUS revealed chronic inflammation and was once again negative for malignancy. Follow-up positron emission tomography (PET) scan, however, revealed a lesion in the pancreatic head that had mild F-fluorodeoxyglucose (FDG) uptake suspicious for malignancy. Of note, IgG4 levels were normal. The case was presented at the multidisciplinary tumor board. Given the inconclusive results with limited treatment options for ongoing debilitating abdominal pain and the possibility of malignancy, the patient underwent a Whipple procedure without complication. Pathology was fortunately negative for malignancy but revealed granulomatous inflammation in the pancreas, with several lymph nodes of the pancreas, bile duct, and liver demonstrating granulomatous inflammation (Figure 2), findings suggestive of sarcoidosis. The postoperative course was uncomplicated. The patient was established with rheumatology and was started on prednisone with clinical improvement. At follow-up, the patient had no evident additional manifestations of sarcoidosis.
CT scan showing a hyperdense mass-like lesion in the pancreatic head and uncinate process (arrow)CT: computed tomography
Pathology from peripancreatic lymph node showing lymphohistiocytic inflammatory infiltrate with aggregates of histiocytes and no cellular debris (arrow), consistent with non-necrotizing granulomatous inflammation
Discussion
Sarcoidosis is a multisystem disease that most commonly affects the lungs, followed by the skin, eyes, joints, heart, and central nervous system. Gastrointestinal involvement most commonly involves the liver, followed by the stomach, and rarely finds its way to the pancreas [5,6]. Pancreatic involvement can manifest in many ways, including mimicking pancreatic adenocarcinoma. While pancreatic involvement of sarcoidosis is common, there have only been a few reported cases of isolated pancreatic sarcoidosis, which makes this case particularly interesting.
This patient presented with intractable abdominal pain with concern for a mass on imaging. He underwent two separate EUS procedures with no evidence of malignancy. These biopsies also revealed no evidence of non-caseating granulomas or other signs of sarcoidosis, as has been seen in other cases of isolated pancreatic sarcoidosis [7]. A follow-up PET scan was concerning for pancreatic malignancy. This provided a difficult clinical circumstance. This patient suffered from debilitating abdominal pain with no definitive diagnosis and thus no definitive treatment option. Furthermore, prompt diagnosis and treatment would be required if this suspicious mass indeed represented malignancy. Ultimately, after multidisciplinary collaboration, the patient underwent a Whipple procedure with relief of symptoms and a situationally fortunate diagnosis of sarcoidosis.
Conclusions
Given that pancreatic cancer typically portends a poor prognosis, there is greater urgency in diagnosis and treatment for suspicious pancreatic masses. A high degree of clinical suspicion is necessary to consider sarcoidosis in this setting, with the understanding that isolated pancreatic sarcoidosis is exceedingly rare compared to pancreatic malignancy. In pancreatic masses with no clear diagnosis on biopsy, further investigation for other signs of sarcoidosis should be considered.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1[Gastric sarcoidosis] (Article in Russian)Klin Med (Mosk) Maev IV Andreev DN KucheriavyĭIu A 1822922014 https://pubmed.ncbi.nlm.nih.gov/25796941/25796941 · pubmed ↗
- 2A rare presentation of sarcoidosis as a pancreatic head mass Case Rep Pulmonol Mony S Patil PD English R Das A Culver DA Panchabhai TS 703716220172017 https://doi.org/10.1155/2017/70371622832135510.1155/2017/7037162 PMC 5339531 · doi ↗ · pubmed ↗
- 3Extra-pulmonary manifestations of sarcoidosis Clin Radiol Vardhanabhuti V Venkatanarasimha N Bhatnagar G Maviki M Iyengar S Adams WM Suresh P 2632766720122209418410.1016/j.crad.2011.04.018 · doi ↗ · pubmed ↗
- 4Pancreatic sarcoidosis: a very rare presentation of the disease Cureus Ibrahim H Zebda H Meysami A 012202010.7759/cureus.7996 PMC 727426232523850 · doi ↗ · pubmed ↗
- 5Sarcoidosis of the pancreas: case report and review of the literature Am Surg Bacal D Hoshal VL Jr Schaldenbrand JD Lampman RM 675678662000 https://pubmed.ncbi.nlm.nih.gov/10917480/10917480 · pubmed ↗
- 6Pancreatic sarcoidosis discovered during Whipple procedure J Surg Case Rep Cook J Spees T Telefus P Ranaudo JM Carryl S Xiao P 2013201310.1093/jscr/rjt 016PMC 363522524964428 · doi ↗ · pubmed ↗
- 7Isolated pancreatic sarcoidosis diagnosed by endoscopic ultrasound-guided fine-needle aspiration Intern Med Takeda S Kawaratani H Takami M 140714125920203216121710.2169/internalmedicine.4034-19PMC 7332622 · doi ↗ · pubmed ↗