Clinical Outcomes of Large-Bore Aspiration Thrombectomy for Tumor Pulmonary Embolism in Renal Cell Carcinoma
Anand Mulji, Tony Rizk, Yara Younan, Stephen Stringfellow, Antony Gayed

TL;DR
A 66-year-old man with kidney cancer had a successful treatment for a tumor blockage in his lung, with no recurrence after four years.
Contribution
Demonstrates long-term efficacy of large-bore aspiration thrombectomy in managing tumor pulmonary embolism.
Findings
No disease recurrence was observed over four years following the procedure.
The procedure provided both therapeutic and diagnostic benefits.
Large-bore aspiration thrombectomy enabled histopathologic analysis for treatment guidance.
Abstract
We present a 4-year longitudinal follow-up of a previously reported case involving a 66-year-old man with renal cell carcinoma who underwent radical nephrectomy, complicated by a massive pulmonary artery tumor embolism treated with large-bore aspiration thrombectomy. Serial clinical evaluations and imaging over 4 years have shown no evidence of disease recurrence following the initial intervention. This case underscores the evolving role of emergent large-bore aspiration thrombectomy in oncologic settings, not only as a therapeutic intervention but also for its diagnostic utility in enabling histopathologic characterization and guiding oncologic management. Large-bore aspiration thrombectomy may offer long-term disease control in cases of tumor pulmonary embolism. This procedure can aid diagnosis and inform oncologic treatment planning through tissue acquisition.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
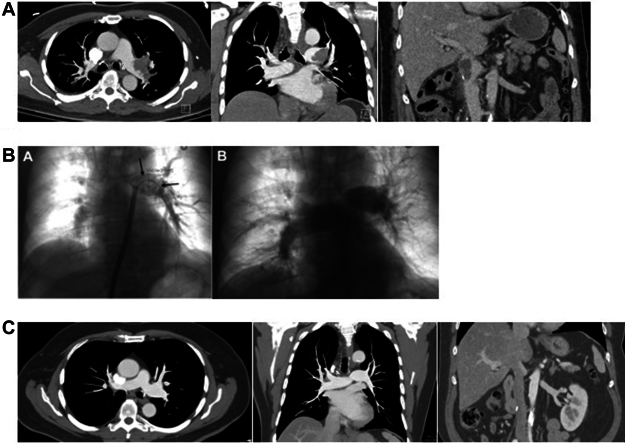 Figure 1
Figure 1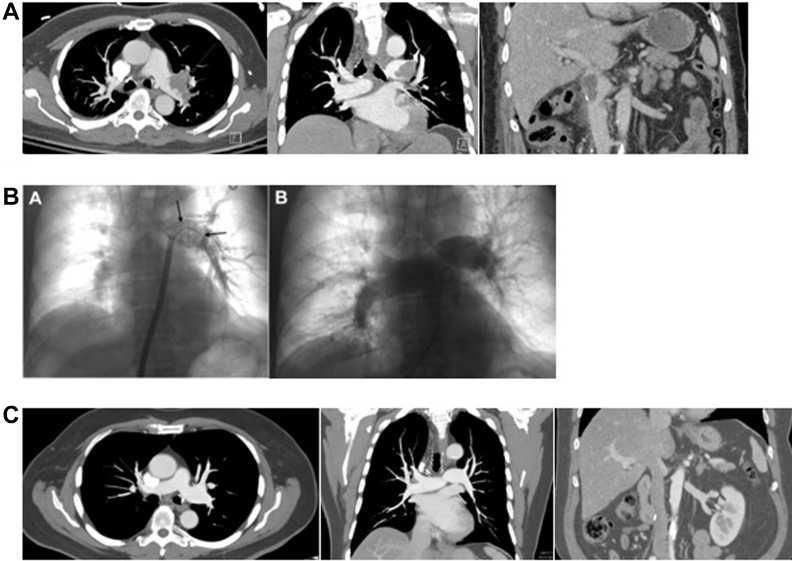 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac tumors and thrombi · Renal cell carcinoma treatment · Renal and Vascular Pathologies
Case Summary
A 66-year-old man presented with hematuria, anemia, and unintentional weight loss. Imaging revealed an 11-cm right renal mass with tumor extension into the right renal vein and a nonocclusive thrombus extending 4.7 cm into the infrahepatic inferior vena cava (IVC). The patient elected to undergo single-stage open right radical nephrectomy with planned IVC tumor thrombectomy. Intraoperatively, the patient experienced acute hemodynamic decompensation, and transesophageal echocardiography demonstrated a right heart thrombus in transit, which subsequently embolized into the pulmonary arterial circulation. Given the emergent circumstances, surgical IVC thrombectomy was deferred, and the nephrectomy was completed by stapling across the tumor-involved renal vein–IVC confluence. Due to the complexity of the case and surgical limitations, large-bore endovascular aspiration thrombectomy was performed the following day, targeting both the IVC and pulmonary embolism. Aspiration thrombectomy of the main and left pulmonary arteries resulted in successful extraction of a 15-cm tumor thrombus, confirmed on a histopathologic analysis. Postprocedural pulmonary angiography demonstrated resolution of the proximal embolus with improved hemodynamics. Intravenous anticoagulation was initiated on postoperative day 1, and transesophageal echocardiography revealed normal cardiac chamber sizes and estimated right atrial pressure. The patient was subsequently transferred out of the intensive care unit, recovered to his baseline functional status, and was discharged in stable condition.Take-Home Message
- •These cases underscore the value of large-bore aspiration thrombectomy in achieving both immediate stabilization and meaningful diagnostic insight in cancer-associated thromboembolism, ultimately informing long-term oncologic strategies.
In 2021, he completed systemic therapy with pembrolizumab and axitinib. In addition, he has since undergone 28 contrast-enhanced CT examinations, including 14 CTs of the abdomen and pelvis, 13 CTs of the chest, and 1 CT pulmonary angiogram (Figure 1). None have demonstrated local disease recurrence or distant metastasis. The patient remains on indefinite anticoagulation with apixaban. Clinically, he continues to be asymptomatic without functional limitations.Figure 1. Preprocedural CT, Intraprocedural Angiography, and Postprocedural CT Images of Pulmonary Arterial Tumor Thromboembolism(A) (left to right) Axial and coronal contrast-enhanced computed tomography (CT) chest demonstrating near-occlusive left pulmonary artery thrombus. Coronal contrast-enhanced CT abdomen and pelvis demonstrating infrahepatic inferior vena cava thrombus. (B) (left to right) Intraprocedural pulmonary angiograms before and after thrombectomy demonstrating near-occlusive left pulmonary artery filling defect (arrows), which resolved with thrombectomy. (C) (left to right) Most recent follow-up axial and coronal contrast-enhanced CT chest demonstrating patent left pulmonary artery. Coronal contrast-enhanced CT abdomen and pelvis demonstrating patent infrahepatic inferior vena.
Discussion
Several case reports have described the use of large-bore aspiration thrombectomy in patients with known malignancies, in both emergent and nonemergent settings. One case involved a patient with a sarcomatoid variant of urothelial carcinoma and thrombus extending into the left renal vein and IVC, who presented with sudden-onset dyspnea. Imaging revealed bilateral segmental pulmonary emboli and a tumor thrombus in transit within the right atrium.1 In another case, a patient with cirrhosis presented with acute respiratory decompensation; imaging revealed previously undiagnosed hepatocellular carcinoma (HCC) and a large right atrial thrombus.2 In both instances, large-bore aspiration thrombectomy resulted in hemodynamic and respiratory stabilization. In the case of undiagnosed HCC, definitive diagnosis was achieved via histologic analysis of the aspirated thrombus. In another illustrative case, a patient with known HCC who had undergone surgical resection was managed conservatively with anticoagulation following a postoperative pulmonary embolism. Ten months later, the patient presented with diffuse pulmonary metastases and increased clot burden. Large-bore aspiration revealed tumor infiltration in 20% of the embolus, confirmed by immunohistochemistry to be consistent with the patient's primary HCC.3
Funding Support and Author Disclosures
Dr Gayed has served as a Medtronic consultant and received grant from Bayer Research. The other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Fuher A.de Boer E.Hountras P.A case of pulmonary tumor embolism syndrome with thrombus in transit Respir Med Case Rep 45202310189610.1016/j.rmcr.2023.101896 PMC 1042420037583563 · doi ↗ · pubmed ↗
- 2Ghaleb M.Koushesh P.Bhatnagar U.Khan A.A.Park M.Sardar R.Aspiration of right atrial tumor metastasis JACC Case Rep 2917202410250210.1016/j.jaccas.2024.102502 PMC 1144216939359507 · doi ↗ · pubmed ↗
- 3Verloh N.Vogt K.Bettinger D.Percutaneous transcatheter aspiration of pulmonary embolism leading to diagnosis of hepatocellular carcinoma tumor embolus and change in systemic chemotherapy Acta Radiol Open 13620242058460124125378010.1177/20584601241253780 PMC 1110040038766646 · doi ↗ · pubmed ↗