A Rare Clinical Presentation of Congenital Superficial Angiomyxoma: A Case Report
Saman Al‐Zahawi, Sara Masoomi, Maryam Ghiasi, Vahidesadat Azhari, Kambiz Kamyab, Faezeh Khorasanizadeh, Ifa Etesami

TL;DR
This case report describes a rare congenital form of superficial angiomyxoma in the vulvar region, observed from birth and growing over two years.
Contribution
The report presents the third documented case of congenital vulvar superficial angiomyxoma, expanding clinical understanding of its rare presentation.
Findings
Superficial angiomyxoma can present congenitally in the vulvar region.
The lesion showed gradual growth over two years, appearing as a pedunculated, red, jelly-like mass.
Abstract
Angiomyxoma is a rare atypical mesenchymal proliferation with two distinct forms, deep and superficial. Superficial Angiomyxoma tends to be benign with limited skin involvement. Rarely, Superficial Angiomyxoma appears in the vulvar region in the form of cystic, vascular, or tumoral lesions. The onset of vulvar superficial angiomyxoma is variable and ranges from early childhood to the post‐menopausal period. To the best of our knowledge, this report presents the third documented case of vulvar superficial angiomyxoma with an onset at birth and a subsequent gradual increase in size over 2 years. A pedunculated, cauliflower red‐colored, jelly mass in the left vulvar region (A) & (B).
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
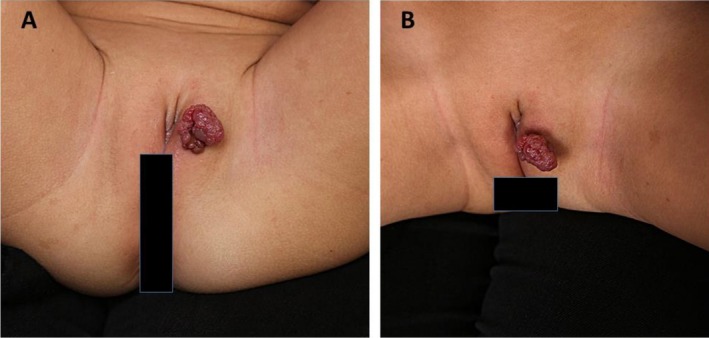 FIGURE 1
FIGURE 1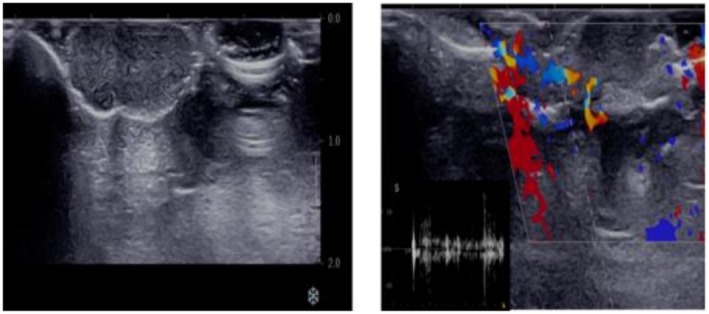 FIGURE 2
FIGURE 2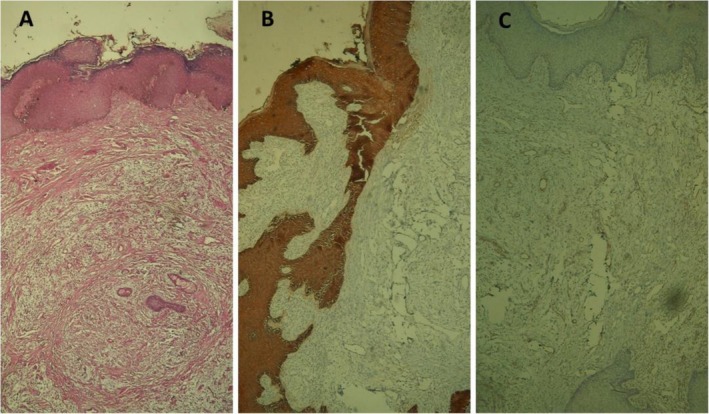 FIGURE 3
FIGURE 3| Reported cases | Age at presentation | Onset of the lesion appearance | Symptoms and finding | Size | Treatment |
|---|---|---|---|---|---|
| Okada et al. | 3‐year | 18 months before presentation | Pedunculated polypoid covered by normal skin | Not reported | Excision |
| Calonje et al. | 11‐year | 8‐year | Vulval mass | 4 cm | Excision |
| Lee et al. | 13‐year | 11‐year | Vulval mass with bleeding | 7 cm × 3 cm × 2 cm | Excision |
| Flynn and O'Brien | 7‐year | Since birth | Pink‐tan, pedunculated, cauliflower‐like mass | 2.5 cm × 1.5 cm × 1.2 cm | Excision |
| Hafeez et al. | 17‐month‐old girl | 2–3 months of age | Pink cerebriform nodule | 0.5 cm | Excision |
| Rose and Arredondo | 6‐year | Since birth | Exophytic tumor | 4.5 × 4.5 × 2.5 cm | Excision |
| Oral et al. | 8‐year | 2 weeks after bone marrow transplantation | Painless vulvar mass | 1 cm × 1 cm | Excision |
| Our case | 2‐year | Since birth | Exophytic, lobulated, vascularized tumor | 2 cm × 3 cm | Excision |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsUrologic and reproductive health conditions · Soft tissue tumor case studies · Genital Health and Disease
Summary
- Pediatric vulvar superficial angiomyxoma is a rare, benign tumor requiring surgical excision and long‐term follow‐up for recurrence and to rule out Carney complex, especially if congenital.
Introduction
1
Angiomyxoma is a rare atypical mesenchymal proliferation with two distinct forms, superficial and deep [1]. While superficial angiomyxoma (SAM) is a benign, cutaneous tumor with limited skin involvement, deep angiomyxoma tends to be aggressive with local invasion and rarely distant metastasis [2]. Although initially, SAM was described in association with the Carney complex, sporadic SAM has frequently been recognized. Sporadic SAM is located mainly in the trunk, head, and neck, with a rare occurrence in the vulva. The onset of vulvar superficial angiomyxoma varies and ranges from early childhood to post‐menopausal [3, 4]. The vulvar subtype may have a cystic, vascular, or tumoral appearance. They might be confused with skin tags, labial cysts, and cysts of Bartholin ducts [5]. Importantly, it should be distinguished from deep angiomyxoma when angiomyxoma is vulvar in origin.
Diagnosis depends on clinical suspicion and pathological findings of the diffuse mucinous matrix within the dermis and subcutis, admixed with fibroblasts and collagen fibers in a well‐lobulated lesion [6]. In the vulvar subtype, immunohistochemistry (IHC) for hormonal receptors like estrogen and progesterone may help to exclude deep angiomyxoma [2]. When the IHC is positive for hormonal receptors, it should be followed by an MRI to define the extent of the disease and instruct the surgeon for wide local excision because of a high rate of recurrence [7]. Although the treatment approach for SAM is local excision, similar to deep angiomyxoma, more conservative excision is applied than that for deep angiomyxoma [2]. This report presents a case of vulvar superficial angiomyxoma diagnosed at birth that demonstrated gradual enlargement over 2 years.
Case History/Examination
2
A 2‐year‐old female patient presented to our center with a pedunculated mass on the vulva. The vulvar lesion started as a small erythematous nodule at birth. Then, there was a gradual increase in the size of the lesion within 2 years, making the parents apprehensive and prompting them to seek medical consultation. The parents stated that the neonatal and perinatal periods were uneventful, and she had been fully vaccinated with no known medical or surgical events.
On examination, there was a 2 × 3 cm, red‐fleshy colored, jelly consistency, cauliflower‐like pedunculated mass on the left vulvar region (Figure 1). On palpation, there was no induration of the mass, and the lesion had no extension to the mucosa of the genitalia. Additionally, there were no widespread nevi or lentiginous lesions on total skin examination.
A pedunculated, cauliflower red‐colored, jelly mass in the left vulvar region (A, B).
Differential Diagnosis, Investigations, and Treatment
2.1
Metabolic panel and blood chemistry were normal, and there were no signs of endocrinopathies. Ultrasound was performed to assess the mass before total excision of the lesion for biopsy. Doppler Ultrasound showed an 18 × 18 mm, well‐defined, hypoechoic, pedunculated mass, with mild internal and peripheral vascularity (Figure 2A,B). Total mass excision was performed with a 2 mm free margin and free tension primary closure.
Color Doppler ultrasound using an 18 MHz linear probe revealed a well‐defined hypoechoic pedunculated mass measuring 18 × 18 mm in the vulva, exhibiting mild peripheral and internal vascularity with a peak systolic velocity of approximately 10 cm/s.
Histopathological evaluation of the specimen revealed a polypoid skin lesion covered by acanthotic epidermis. There was an ill‐defined, dermal multinodular neoplastic proliferation composed mainly of satellite‐spindle cells in extensive myxoid stroma with prominent vasculature. Scattered epithelial strands and keratin‐filled epidermoid cystic spaces were also present. The margin of the excised lesion was free of tumoral proliferation. The clinical‐pathological findings were compatible with superficial angiomyxoma, and the pathologist recommended further evaluation by IHC. IHC was positive for vimentin, CD34, and SMA, but it was negative for desmin, Pan CK, EMA, desmin, and S100 (Figure 3A–C).
H & E revealed ill‐defined, dermal multinodular neoplastic proliferation composed mainly of satellite‐spindle cells in extensive myxoid stroma, with prominent vasculature (A), IHC showed negative pan‐cytokeratin (B), and staining for desmin was negative (C).
Outcome and Follow‐Up
2.2
To ensure optimal follow‐up, patients were recommended to return to our center for check‐ups every 3 months during the first year after excision. This monitoring period was designed to detect any recurrent lesions, the presence of multiple nevi, or the appearance of new skin lesions.
Discussion
3
Pediatric vulvar superficial angiomyxoma is a benign, sporadic, extremely rare tumor, with only eight cases being reported in the literature (including ours) (Table 1). The vulva is the third most common location of SAM in children after the head and neck [3]. Vulvar lesions of SAM are usually asymptomatic and appear as a painless mass, pedunculated lesion, ulcerated bleeding mass, cerebriform nodule, or vascularized pedunculated mass.
The age of onset of pediatric valvar SAM has varied from birth until 11 years, with usual late consultation with physicians until the lesion grows larger or develops ulceration with bleeding. To our knowledge, this is the third case of SAM with an onset at birth and late presentation at 2 years after significant growth of the lesion. The size may be as small as 0.5 cm to as large as 7 cm [8, 9]. Although the literature has defined sporadic SAM as an acquired condition [10], our case is the third case of having lesions at birth, which may point to a sporadic congenital condition unrelated to the known Carney Complex. Nevertheless, children with early‐onset SAM should be evaluated thoroughly for the latter syndrome as angiomyxoma may be the first sign of Carney Complex. Carney Complex is an autosomal dominant condition characterized by skin pigmentation, endocrine overactivity, and myxoma due to a mutation in PRKAR1A. The absence of blue nevi, endocrinopathies, and multiple cutaneous myxomas in different anatomical locations led to the exclusion of the Carney Complex in our study. Other conditions involving the female genitalia in a child should be considered, like rhabdomyosarcoma, liposarcoma, epidermal cyst, abscess, and the aggressive, deep form of vulvar angiomyxoma [11].
Pathological assessment is essential for the definitive diagnosis of clinically suspected cases of pediatric vulvar SAM and differentiation from the aforementioned conditions. The characteristic pathological finding is a well‐defined tumor with diffuse vascular proliferation in an abundant mucinous matrix. IHC is usually recommended to distinguish between the aggressive, deep angiomyxoma, which is hormone‐dependent and is positive for both estrogen and progesterone receptors, from the superficial angiomyxoma, which is CD34+, Vimentin negative, and S100+ [12]. Our case was S100 negative, Vimentin+, and CD34+, findings compatible with superficial angiomyxoma. However, entities with mucin infiltration, like focal cutaneous mucinosis, cutaneous myxoid cyst, dermal nerve sheath myxoma, and myxoid liposarcoma, should be considered in the histopathological differential diagnosis of SAM.
To distinguish the deep angiomyxoma from the vulvar superficial angiomyxoma, radiological evaluation with either MRI or Ultrasound is needed to evaluate the depth of the lesions and their vascular characterization. The aforementioned preoperative imaging aids in the complete surgical resection of the lesion, which is the standard treatment modality. It is noteworthy that incomplete surgical excision accounts for 30%–40% of recurrent cases of angiomyxoma [13]. Also, recurrence in pediatric vulvar SAM after surgical resection has been reported in one patient by Raquel et al. in their systematic review of pediatric vulvar SAM [3]. We recommend longitudinal evaluation of children with pediatric vulvar SAM for recurrence and signs of Carney Complex.
Conclusion
4
Pediatric vulvar angiomyxoma is a rare benign condition in children with a variable onset from birth to late adolescence. Lesions are treated by surgical excision. Patients are longitudinally evaluated for recurrence and to exclude the Carney complex.
Author Contributions
Saman Al‐Zahawi: writing – original draft, writing – review and editing. Sara Masoomi: writing – original draft, writing – review and editing. Maryam Ghiasi: conceptualization, data curation. Vahidesadat Azhari: visualization. Kambiz Kamyab: visualization. Faezeh Khorasanizadeh: visualization. Ifa Etesami: data curation, supervision.
Consent
Written informed consent was obtained from the patient to publish this report following the journal's patient consent policy.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1H. Hamali , M. Khordadmehr , and F. Jigari‐Asl , “Clinical and Histopathological Diagnosis of Superficial Angiomyxoma in a Pregnant Holstein Heifer,” Iranian Journal of Veterinary Surgery 19, no. 1 (2024): 73–76.
- 2A. Navitski , L. Adams , B. N. Brzezinska , et al., “A Tale of Two Vulvar Angiomyxomas: Two Cases and Review of the Literature,” Gynecologic Oncology Reports 47 (2023): 101204.37304973 10.1016/j.gore.2023.101204 PMC 10248035 · doi ↗ · pubmed ↗
- 3R. Ros Briones , J. Arredondo Montero , M. Bronte Anaut , S. Hernández‐Martín , and R. Guarch Troyas , “Pediatric Vulvar Superficial Angiomyxoma: A Case Report With Clinical, Radiological, and Anatomopathological Characterization and a Comprehensive Review of the Literature,” International Journal of Surgical Pathology 31, no. 5 (2023): 852–860.36476168 10.1177/10668969221140381 · doi ↗ · pubmed ↗
- 4S. H. Lee , Y. J. Cho , M. Han , et al., “Superficial Angiomyxoma of the Vulva in a Postmenopausal Woman: a Case Report and Review of Literature,” Journal of Menopausal Medicine 22, no. 3 (2016): 180–183.28119899 10.6118/jmm.2016.22.3.180PMC 5256360 · doi ↗ · pubmed ↗
- 5B. Brzezinska , A. E. Clements , K. S. Rath , and G. C. Reid , “A Persistent Mass: a Case of Aggressive Angiomyxoma of the Vulva,” Gynecologic Oncology Reports 24 (2018): 15–17.29552629 10.1016/j.gore.2018.02.002PMC 5852285 · doi ↗ · pubmed ↗
- 6H. S. Kim , G. Y. Kim , S. J. Lim , K. D. Ki , and H. C. Kim , “Giant Superficial Angiomyxoma of the Vulva: a Case Report and Review of the Literature,” Journal of Cutaneous Pathology 37, no. 6 (2010): 672–677.19615026 10.1111/j.1600-0560.2009.01333.x · doi ↗ · pubmed ↗
- 7J. F. Fetsch , W. B. Laskin , and F. A. Tavassoli , “Superficial Angiomyxoma (Cutaneous myxoma) a Clinicopathologic Study of 17 Cases Arising in the Genital Region,” International Journal of Gynecological Pathology 16, no. 4 (1997): 325–334.9421071 10.1097/00004347-199710000-00006 · doi ↗ · pubmed ↗
- 8A. D. Oprea , “Solitary Superficial Angiomyxoma in an Uncommon Location: A Case Report and Literature Review,” Cureus 16, no. 8 (2024): 726.10.7759/cureus.67521 PMC 1141620139310581 · doi ↗ · pubmed ↗