Treatment of Tuberculous Meningitis With Contezolid in a Patient With Complex Comorbidities: A Case Report and Literature Review
Qi Fan, Hong Sun, Shengsheng Liu

TL;DR
A patient with complex health issues was successfully treated for CNS tuberculosis using contezolid, a newer antibiotic that may be safer than older alternatives.
Contribution
This case report provides clinical evidence of contezolid's potential in treating complex CNS tuberculosis.
Findings
Contezolid was part of a successful multidrug regimen for a patient with severe CNS TB and multiple comorbidities.
The treatment suggests contezolid may be a safer alternative to linezolid in complex TB cases.
Further research is needed to confirm the role of contezolid in CNS TB treatment.
Abstract
Central nervous system (CNS) tuberculosis (TB) is a severe manifestation of Mycobacterium tuberculosis (MTB) infection, characterized by high mortality. Contezolid, a novel oxazolidinone antibiotic, exhibits in vitro activity against MTB and may offer a safety advantage over linezolid, a first-generation oxazolidinone frequently linked to myelosuppression and neuropathy. Clinical data on contezolid in CNS tuberculosis remain scarce. We report a middle-aged man with chronic renal allograft dysfunction who was receiving long-term hemodialysis and subsequently developed severe CNS TB complicated by multiple coinfections, diabetes mellitus, and pancytopenia. An individualized multidrug regimen that included contezolid was successfully employed, suggesting its potential utility in complex CNS TB. This report highlights therapeutic considerations for similar patients and underscores the need…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1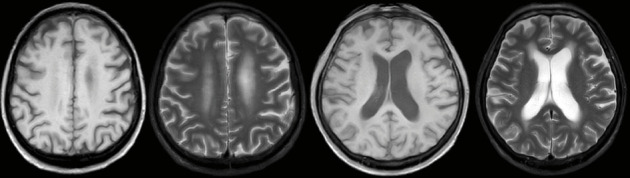 Figure 2
Figure 2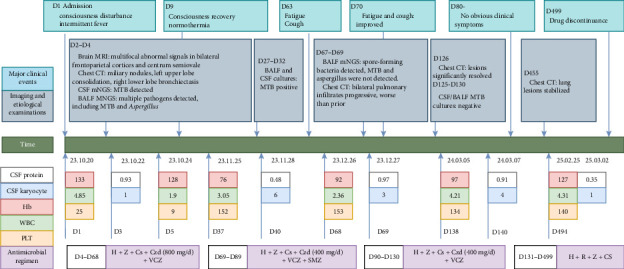 Figure 3
Figure 3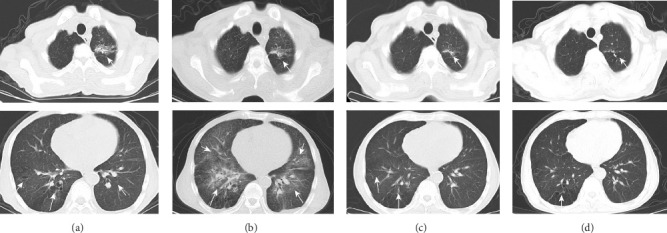 Figure 4
Figure 4- —Natural Science Foundation of Anhui Provincial Science and Technology Department
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfectious Diseases and Tuberculosis · Mycobacterium research and diagnosis · Tuberculosis Research and Epidemiology
1. Introduction
Central nervous system (CNS) tuberculosis (TB) represents the most severe form of extrapulmonary disease, often resulting in irreversible neurological sequelae such as encephalitis, cranial neuritis, hydrocephalus, vasculitis, and stroke, and is associated with substantial mortality [1]. Although current treatment combines antituberculosis (anti-TB) agents with anti-inflammatory therapy, optimal efficacy remains elusive, prompting interest in novel antibiotics or improved drug delivery to the site of infection. Agents with high cerebrospinal fluid (CSF) penetration, such as linezolid, have demonstrated efficacy in CNS TB and are recommended for multidrug-resistant (MDR) and extensively drug-resistant (XDR) TB [2]. However, linezolid's use is limited by adverse effects, including peripheral and optic neuropathy and bone-marrow suppression [3]. Contezolid, a next-generation oxazolidinone, was originally developed for MDR Gram-positive infections, including complicated skin and soft-tissue infections caused by Staphylococcus aureus, Streptococcus pyogenes, and Streptococcus agalactiae [4–6]. In vitro susceptibility testing has shown that contezolid possesses activity comparable to linezolid against both drug-susceptible and drug-resistant Mycobacterium tuberculosis (MTB) [7, 8], while emerging clinical data indicate a favorable safety profile with lower rates of myelosuppression and neurotoxicity [9–11]. Notably, contezolid does not require dose adjustment in mild-to-moderate renal impairment [12, 13], and its tolerability has been confirmed in patients receiving hemodialysis during short antibacterial courses [14]. A previous report documented successful treatment of recurrent refractory TB ascites with contezolid in a patient with chronic kidney transplant dysfunction [15]. Despite these promising findings, the clinical applicability and safety of contezolid, particularly concerning its distinct metabolic properties, require further validation. Here, we describe a middle-aged man with severe CNS TB and chronic renal allograft dysfunction on long-term hemodialysis, complicated by diabetes, pancytopenia, and polymicrobial infections, who responded favorably to an individualized multidrug regimen including contezolid. This report aims to broaden the understanding of anti-TB strategies in patients with complex comorbidities.
2. Case Presentation
A 62 year-old man with a 16 year history of well-controlled Type 2 diabetes mellitus, a 10 year history of hypertension, and a 13 year history of chronic kidney disease (on thrice-weekly hemodialysis for the past 4 years) was admitted on 20 October 2023 with a 4 day history of altered consciousness and an 11 day history of intermittent fever that had initially been overlooked until neurological deterioration prompted prior hospitalization, where empirical antimicrobial therapy proved ineffective. Three years after total gastrectomy for gastric cancer, he was transferred to our intensive care unit (ICU) with pancytopenia (white blood cells [WBCs]: 1.90 × 10^9^/L, red blood cells [RBCs]: 4.11 × 10^12^/L, and platelets [PLTs]): 9 × 10^9^/L), hypoalbuminemia (31.7 g/L), and acute-on-chronic renal failure (creatinine: 445.9 μmol/L). Brain magnetic resonance imaging (MRI) revealed multifocal abnormal signals in the bilateral frontoparietal cortices and semioval centers (Figure 1), while chest computed tomography (CT) showed miliary nodules, left upper-lobe consolidation, and right lower-lobe bronchiectasis. CSF analyzed by metagenomic next-generation sequencing (mNGS) yielded MTB DNA, confirming tuberculous meningitis. Bronchoalveolar lavage fluid (BALF) obtained via bedside bronchoscopy was positive on GeneXpert MTB/RIF (rifampicin-susceptible, “low” detection level); mNGS additionally identified Streptococcus pneumoniae, Pseudomonas aeruginosa, Aspergillus, Pneumocystis jirovecii, and MTB DNA sequences, supporting miliary TB. Subsequent cultures of both BALF and CSF confirmed growth of MTB, while BALF also yielded Aspergillus fumigatus with a positive galactomannan (GM) antigen test, indicating concomitant invasive pulmonary aspergillosis. Final diagnoses were CNS TB, miliary pulmonary tuberculosis (PTB), invasive pulmonary aspergillosis, and polymicrobial pulmonary coinfection.
Owing to preexisting bone-marrow suppression, linezolid, known to worsen cytopenias, was avoided in favor of contezolid. Because voriconazole was required for concurrent fungal infections and rifampicin markedly reduces voriconazole plasma concentrations [16], rifampicin was excluded from the initial regimen. The anti-TB regimen comprised isoniazid 300 mg once daily, pyrazinamide 1500 mg once daily, contezolid 400 mg twice daily, and cycloserine 250 mg twice daily, supplemented with voriconazole 200 mg twice daily for antifungal therapy. All medications were administered after hemodialysis sessions. PLT transfusions and other hematopoietic supportive measures were provided. The patient improved clinically within 6 days, with resolution of fever and restoration of consciousness. Follow-up laboratory tests showed hematological recovery: WBCs: 5.09 × 10^9^/L, RBCs: 4.13 × 10^12^/L, and PLTs: 54 × 10^9^/L. After stabilization, he was discharged to continue thrice-weekly hemodialysis.
At the 2-month follow-up, the patient reported fatigue and a new-onset cough of 1-week duration, without fever or neurological symptoms. Examination revealed no recurrence of CNS infection. CSF parameters remained stable compared to previous results (Figure 2), and cultures were negative, confirming controlled tuberculous meningitis. Chest CT showed progressive bilateral pulmonary infiltrates (Figure 3(b)). BALF mNGS detected spore-forming bacteria, prompting initiation of cotrimoxazole 960 mg three times daily after respiratory consultation. Drawing on the experience of linezolid dose adjustment in TB treatment in the literature [17] and considering the patient's limited financial resources, we reduced contezolid to 400 mg once daily. After 3 weeks of therapy and clinical improvement, cotrimoxazole was discontinued. Subsequent chest CT on 22 February 2024 demonstrated marked lesion resolution (Figure 3(c)). At the March review, he remained asymptomatic with normal findings. CSF profiles were stable from baseline (Figure 2), with negative MTB cultures from CSF and BALF, and no pathogens detected by mNGS. After clinical assessment confirmed cure of pulmonary aspergillosis, voriconazole was stopped, and anti-TB therapy was adjusted to rifampicin 600 mg once daily, isoniazid 300 mg once daily, pyrazinamide 1500 mg once daily, and cycloserine 250 mg twice daily. Follow-up has shown continued clinical stability, with chest CT on 17 January 2025 revealing unchanged pulmonary findings (Figure 3(d)). Throughout treatment, WBC and PLT counts fluctuated within safe ranges, while CSF cellularity and protein normalized (Figure 2). All microbiological results are summarized in Table 1. Key clinical events, examination findings, and treatment regimens are depicted in Figure 2. Anti-TB therapy was completed on 2 March 2025, with ongoing surveillance planned.
3. Discussion
This complex case involved concurrent CNS and PTB with polymicrobial coinfections, further complicated by diabetes mellitus, hypertension, and end-stage renal disease requiring maintenance hemodialysis. Unexplained pancytopenia posed additional therapeutic challenges, necessitating deviation from standard anti-TB protocols. The patient's multifaceted pathology demanded an individualized strategy that (1) tailored antimicrobial selection to address both tuberculosis and opportunistic infections while accommodating renal impairment, (2) carefully managed drug interactions, particularly between anti-TB and antifungal agents, and (3) ensured ongoing hematological monitoring given baseline cytopenias. This approach balanced microbiological efficacy with organ-system preservation, underscoring the need for personalized management in complex tuberculosis presentations.
Designing the initial anti-TB regimen was challenging due to the patient's complex clinical status, requiring individualization over standardization. Rifampicin was excluded initially due to its significant interaction with voriconazole [16]. CSF penetration guided agent selection; the initial regimen included isoniazid, pyrazinamide, and cycloserine, with an oxazolidinone added later. While linezolid offers strong CSF penetration and anti-TB activity, its risk of myelosuppression was problematic, given the patient's pancytopenia. We thus chose contezolid, a domestically developed oxazolidinone approved in 2021 for complex skin and soft-tissue infections [18], for its favorable safety profile. Contezolid's distinctive chemical structure, featuring a nonplanar A- and B-ring system conferred by an orthofluoro substituent, is associated with reduced myelosuppressive toxicity [19]. Clinical evidence demonstrates resolution of linezolid-associated peripheral neuropathy and hematological toxicity after switching to contezolid [9, 15, 20], while in vitro studies by Wang et al. revealed superior intracellular bactericidal activity against MTB compared to linezolid [21]. After a comprehensive discussion and informed consent from the patient's family, contezolid was incorporated into the anti-TB regimen.
To our knowledge, published reports of contezolid in CNS tuberculosis remain extremely limited. A literature search of PubMed from 1 January 2015 to 31 January 2025 using the terms “contezolid” and “tuberculosis” identified only three documented cases, including ours (Table 2; Supporting Figure 1). Among these, our patient presented the most complex clinical picture and posed the greatest therapeutic challenge. The case series comprised one male and two female patients (mean age: 54.3 years, range: 32–69). One case shared similar neurological manifestations, fever and altered consciousness [22], with our patient, whereas another exhibited only constitutional symptoms such as fever, nausea, and vomiting [20]. Notably, our case is the first in which contezolid was used as initial anti-TB therapy, whereas the other two involved substitution after linezolid intolerance. A further distinguishing feature is that our patient had pancytopenia while receiving long-term hemodialysis. The cytopenia most likely resulted from the combined effects of severe infection, renal anemia, and uremic thrombocytopenia rather than drug toxicity. After initiation of an anti-TB regimen containing contezolid 400 mg twice daily, no additional myelosuppression occurred; instead, blood counts gradually improved alongside infection control and adjunctive hematopoietic support. Although blood drug concentrations were not monitored, therapeutic efficacy was not compromised by hemodialysis. This observation may provide valuable guidance for treating TB in patients with renal failure requiring hemodialysis. The maximum reported duration of contezolid therapy was 8 months [22], with no drug-related adverse events in any case, suggesting its potential as a safer alternative to linezolid. Although anti-TB regimens differed, all three patients achieved favorable outcomes, indicating that contezolid is both effective and well tolerated in CNS TB. Pharmacokinetic data remain sparse, with only one case reporting CSF concentrations: at 7 h postdose during Weeks 7 and 11, serum levels were 9.64 mg/L and 9.36 mg/L, respectively, and corresponding CSF concentrations were 0.54 mg/L and 1.15 mg/L [20]. The limited sampling underscores the need for more comprehensive pharmacokinetic studies assessing tissue penetration, as well as randomized controlled trials to establish contezolid's role in CNS TB. Interestingly, rifampicin was omitted during a specific stage in all three cases for various reasons, yet successful outcomes were achieved, further supporting the potential inclusion of contezolid in CNS TB regimens.
Our investigation has two principal limitations. First, the absence of CSF and blood concentration monitoring for contezolid precludes definitive dose optimization for CNS TB. We plan to collect paired serum and CSF samples on Day 8 and at Weeks 4, 6, and 8 of therapy for pharmacokinetic analysis. Second, the patient's chronic hemodialysis complicated the accurate assessment of contezolid's nephrotoxic potential. Currently available pharmacokinetic data are insufficient to establish optimal dosing and administration timing for patients with renal impairment requiring dialysis, an important knowledge gap that warrants further study.
Despite these limitations, our findings suggest that contezolid may be a potentially valuable therapeutic alternative for CNS TB patients, who require hemodialysis and have baseline pancytopenia. These preliminary observations are hypothesis-generating; adequately powered, controlled studies involving larger cohorts are needed to confirm contezolid's role in TB management, particularly among patients with renal impairment or hematological vulnerability.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Leonard J. M. Central Nervous System Tuberculosis Microbiology Spectrum 20175210.1128/microbiolspec.tnmi 7-0044-20172-s 2.0-85016057322 PMC 1168748628281443 · doi ↗ · pubmed ↗
- 2Sun F. Ruan Q. Wang J. Linezolid Manifests a Rapid and Dramatic Therapeutic Effect for Patients With Life-Threatening Tuberculous Meningitis Antimicrobial Agents and Chemotherapy 20145810629763012509269210.1128/AAC.02784-14PMC 4187991 · doi ↗ · pubmed ↗
- 3Sotgiu G. Centis R. D’Ambrosio L. Efficacy, Safety and Tolerability of Linezolid Containing Regimens in Treating MDR-TB and XDR-TB: Systematic Review and meta-analysis European Respiratory Journal 2012406143014422249633210.1183/09031936.00022912 · doi ↗ · pubmed ↗
- 4Wu J. Wu H. Wang Y. Tolerability and Pharmacokinetics of Contezolid at Therapeutic and Supratherapeutic Doses in Healthy Chinese Subjects, and Assessment of Contezolid Dosing Regimens Based on Pharmacokinetic/Pharmacodynamic Analysis Clinical Therapeutics 201941611641174.e 43112669410.1016/j.clinthera.2019.04.025 · doi ↗ · pubmed ↗
- 5Kaul G. Dasgupta A. Chopra S. Contezolid in Complicated Skin and Soft Tissue Infection Drugs of Today 20225873153263585186710.1358/dot.2022.58.7.3389002 · doi ↗ · pubmed ↗
- 6Li B. Liu Y. Luo J. Cai Y. Chen M. Wang T. Contezolid, a Novel Oxazolidinone Antibiotic, May Improve Drug-Related Thrombocytopenia in Clinical Antibacterial Treatment Frontiers in Pharmacology 202314 p. 115743710.3389/fphar.2023.1157437 PMC 1016510037168994 · doi ↗ · pubmed ↗
- 7An H. Sun W. Liu X. Wang T. Qiao J. Liang J. In Vitro Activities of Contezolid (MRX-I) Against Drug-Sensitive and Drug-Resistant Mycobacterium tuberculosis Microbiology Spectrum 2023115 p. e 046272210.1128/spectrum.04627-22PMC 1058081637732805 · doi ↗ · pubmed ↗
- 8Shoen C. De Stefano M. Hafkin B. Cynamon M. In Vitro and in Vivo Activities of Contezolid (MRX-I) Against Mycobacterium tuberculosis Antimicrobial Agents and Chemotherapy 2018628 e 00493182978484810.1128/AAC.00493-18PMC 6105800 · doi ↗ · pubmed ↗