Effect of progesterone sequential therapy on follicle stimulating hormone (FSH), luteinizing hormone (LH), and estradiol (E2) in perimenopausal dysfunctional uterine bleeding
Song Wu, Huiru Wang, Yuwei Zhao, Bo Tang, Qi Zhang, Dapeng Li

TL;DR
This study examines how progesterone sequential therapy affects hormone levels in women with perimenopausal dysfunctional uterine bleeding.
Contribution
The study introduces progesterone sequential therapy as a treatment for PDUB and evaluates its impact on key reproductive hormones.
Findings
FPST significantly reduced FSH and LH levels in PDUB patients.
Estradiol levels were also notably decreased in the FPST group.
FPST showed better clinical outcomes compared to curettage alone.
Abstract
Perimenopausal dysfunctional uterine bleeding (PDUB) is a common gynaecological disease with various clinical treatment options. The objective of this work was to investigate the clinical effect of female progesterone sequential therapy (FPST) on PDUB and follicle-stimulating hormone (FSH), luteinizing hormone (LH), and estradiol (E2). 140 cases of PDUB patients were enrolled and randomly rolled into an observation (Obs) group and a control (Ctrl) group, with 70 cases in each. The patients in the Ctrl group were given pure curettage treatment, and those in the Obs group were supplemented with FPST based on the intervention in the Ctrl group.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
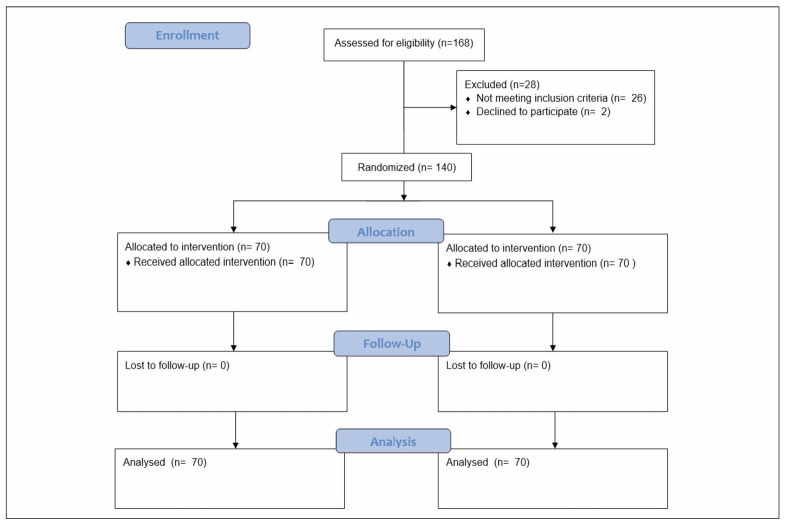 Figure 1
Figure 1| Variable | Obs Group (n=70) | Ctrl Group (n=70) | P-value |
|---|---|---|---|
| Age (years) | 47.5±2.8 (45–50) | 47.1 ± 3.2 (44–50) | 0.42 |
| The course of disease (months) | 6.7±1.2 (4–13) | 6.6 ± 1.3 (4–12) | 0.63 |
| Heart Rate (beats/min) | 76.5±5.6 | 77.1±6.0 | 0.51 |
| Systolic Blood Pressure (mmHg) | 115.3±9.5 | 116.0 ±8.8 | 0.71 |
| Diastolic Blood Pressure (mmHg) | 76.1±6.7 | 77.3±7.0 | 0.55 |
| Clinical Efficacy | |||
| ‣ Cured | 59 | 31 | <0.001 |
| ‣ Obviously Effective | 5 | 10 | 0.03 |
| ‣ Effective | 4 | 11 | 0.24 |
| ‣ Ineffective | 2 | 18 | <0.001 |
| Cure Rate (%) | 84.26 | 44.29 | <0.001 |
| Total Effective Rate (%) | 97.14 | 74.29 | 0.02 |
| FSH (U/L) | 22.8±3.6 | 35.1±4.2 | <0.001 |
| LH (U/L) | 21.1±2.8 | 29.6±3.7 | <0.001 |
| E2 (pmol/L) | 120.4±5.9 | 185.5±6.7 | <0.001 |
| Adverse Reactions (%) | 4.29 (3/70) | 2.86 (2/70) | 0.68 |
| Recurrence Rate (%) | 1.43 (1/70) | 44.29 (31/70) | <0.001 |
- —The research is supported by Wenyang stickers on spleen and kidney yang deficiency chronic bronchitis action mechanism research project number: 2014379, Patent Number: ZL 2015 1 0250209.8
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEndometriosis Research and Treatment · Ovarian function and disorders · Uterine Myomas and Treatments
Introduction
Perimenopause is the female reproductive system gradually from the fertile period to the menopause transition stage, which is an important physiological transition period in female life [1]. Among them, dysfunctional uterine bleeding is one of the common symptoms of perimenopause, mainly manifested as irregular menstrual volume, irregular cycle, prolonged menstruation, and other symptoms [2]. Perimenopausal women’s abnormal uterine bleeding affects quality of life; hysteroscopic treatments offer alternatives to hysterectomy with varied outcomes [3] [4]. Perimenopausal women with abnormal uterine bleeding require treatment evaluation, with urgency varying from anaemia to potential cancer diagnosis consideration. Treatment methods include estrogen replacement therapy, oral contraceptives, intrauterine devices, etc., but there are certain side effects and limitations [3] [4]. Estrogen-progesterone, as a commonly used hormone replacement therapy, has been widely used in perimenopausal women. By supplementing estrogen and progesterone, estrogen and progesterone can adjust endocrine levels, thus alleviating perimenopausal symptoms and improving quality of life [5].
Moreover, it has been applied to a certain extent in clinical practice as a comprehensive treatment of different types of hormones. However, its curative effect in PDUB is not yet clear [6]. Ismet Inan et al. found tibolone and estrogen-progestogen therapy equally effective in alleviating perimenopausal psychological symptoms, with added lipid benefits [7]. Jahedbozorgan & Hasanzadeh found that continuous hormone therapy led to amenorrhea in postmeno pausal women, whereas sequential therapy resulted in varied bleeding [8]. Armeni et al. [9] recommend se quential hormone therapy for managing meno pause, with individualization key to minimizing risks and maximizing efficacy benefits [10]. Ruan & Mueck reviewed and recommended sequential-combined estrogen/progestogen regimens for optimizing menstrual regulation and minimizing risks, with transdermal estradiol and progesterone or dydrogesterone as the »golden standard« for reducing venous thromboembolism and stroke risks in menopausal hormone therapy.
Despite the existing literature on the use of hormone replacement therapy (HRT) in perimenopausal women, there are several deficiencies in the current understanding of its effectiveness in managing PDUB. Firstly, most studies have focused on the use of estrogen-progesterone therapy in postmenopausal women, with limited research on its application in perimenopausal women with PDUB [8] [9]. Secondly, the existing studies have primarily evaluated the effects of HRT on menopausal symptoms, such as hot flashes and night sweats, with few studies examining its impact on PDUB specifically. Furthermore, the optimal regimen and dosage of HRT for managing PDUB remain unclear [8] [9] [10]. Therefore, this study aimed to investigate the clinical effect of female progesterone sequential therapy (FPST) on PDUB, focusing on its impact on FSH, LH, and estradiol levels. By comparing the therapeutic effects of FPST with those of pure curettage treatment, this study aimed to provide new insights into managing PDUB and contribute to developing more effective treatment strategies for perimenopausal women. Ultimately, this study aims to inform the development of more effective and personalized treatment strategies for perimenopausal women with PDUB, improving their quality of life and reducing the risk of complications associated with this condition.
Materials and methods
PDUB patients admitted to Qinhuangdao Hospital of Traditional Chinese Medicine from February 2022 to December 2023 were enrolled and randomly rolled into an observation (Obs) group and a control (Ctrl) group, with 70 cases each. This work has been approved by the Medical Ethics Committee of Qinhuangdao Hospital of Traditional Chinese Medicine (with code of 2014379), and all the patients’ families participating in the study have signed consent forms.
The patients enrolled here had to satisfy all the following items: ① perimenopausal women, aged 45–55 years; ② there were clinical symptoms of dysfunctional uterine bleeding including menorrhagia, irregular menstruation, and prolonged menstruation; and ③ no obvious organic diseases such as uterine fibroids and endometriosis were found through clinical examination and B-ultrasonography. The patients had to be excluded if they had any of the below conditions: ① patients with liver, kidney, and other organ diseases and those who had taken hormone drugs in the past 3 months; ② patients with a history of drug allergy related to this study; and ③ blood system diseases, such as coagulation dysfunction, were detected.
Treatment methods
Pure curettage treatment was given to patients in the Ctrl group. FPST treatment, including sequential use of estrogen and progesterone, was given to patients in the Obs group. That is, synthetic estrogens, such as estradiol, taken orally at 1 mg daily during the first 14 days of the menstrual cycle; using a synthetic progesterone, such as medroxyprogesterone acetate, orally at 10 mg daily on days 15–28 of the menstrual cycle.
Evaluation criteria and observation indexes of efficacy
The treatment efficacy was evaluated as four degrees. Cured: the symptoms of irregular vaginal bleeding disappeared completely, and there was no recurrence in 6 months. Obviously effective: the menstrual cycle and blood volume returned to normal or amenorrhea, and there was no recurrence at 6 months. Effective: the menstrual cycle and blood volume returned to normal. Ineffective: the menstrual cycle did not change, and the symptoms of vaginal bleeding did not improve or worsen compared with before treatment. After treatment, 5 mL of fasting venous blood was collected, centrifuged at 1,500 rpm for 10 min, and serum was collected to measure the follicle-stimulating hormone (FSH), luteinizing hormone (LH), and estradiol (E2) by radioimmunoassay. All patients were followed up for 3 months to count the recurrence and adverse reactions for comparison.
Statistical method
SPSS18.0 was utilized for statistical analysis of the data. The count and measurement data were expressed by frequency and mean ± standard deviation, respectively, subjecting to the 2 and independent sample t-tests. P<0.05 meant a statistically significant difference.
Results
The final number of 140 patients was included, as illustrated in Figure 1.
CONSORT flow diagram of the study.
In the Obs group, the patients were 45~50 years old and (47.5±2.8) years old. The course of disease (COD) ranged from 4 to 13 months ((6.7±1.2) months on average), the heart rate (HR) was (76.5±5.6) beats/min, the systolic blood pressure (SBP) was (115.3±9.5) mmHg, and the diastolic blood pressure (DBP) was (76.1±6.7) mmHg. The 70 patients in the Ctrl group ranged in age from 44 to 50 years ((47.1±3.2) years on average). The COD was 4∼12 months (averaged as (6.6±1.3) months). Meanwhile, the HR, SBP, and DBP were (77.1±6.0) beats /min, (116.0±8.8) mmHg, and (77.3±7.0) mmHg, respectively. A comparison of the above data revealed that the difference was insignificant (P>0.05).
Table 1 illustrates the clinical efficacies of patients in different groups. In the Obs group, 59 patients were cured, 5 were obviously effectively treated, 4 were effectively treated, and 2 were ineffectively treated. In the Ctrl group, the numbers of patients with cured, obvious effective, effective, and ineffective efficacy were 31, 10, 11, and 18, respectively. The above data suggested that the CR and TER in the Obs group (84.26% and 97.14%) were greatly higher than those in the Ctrl group (44.29% and 74.29%), exhibiting obvious differences (P<0.05). The specific data of CR and TER are displayed in Table 1.
The FSH, LH, and E2 levels of patients after they were treated differently were compared in Table 1. The above three indicators in the Obs group were (22.8±3.6) U/L, (21.1±2.8) U/L, and (120.4±5.9) pmol/L, respectively; while those in the Ctrl group were (35.1±4.2) U/L, (29.6±3.7) U/L, and (185.5±6.7) pmol/L, respectively. These findings suggested that the FSH, LH, and E2 levels of patients treated by FPST with curettage treatment were greatly lower than those treated by pure curettage treatment, showing obvious differences with P<0.05.
Among the 70 patients in the Obs group, 3 cases had mild adverse reactions such as nausea and vomiting after taking the drug, which disappeared without clinical treatment, and the incidence of adverse reactions was 4.29% (3/70). In the Ctrl group, 2 patients had mild adverse reactions such as nausea and vomiting after taking the drug, which disappeared without clinical treatment, and the incidence of adverse reactions was 2.86% (2/70). The comparison in incidences of adverse reactions of patients receiving different treatments exhibited no remarkable difference (P>0.05), as illustrated in Table 1.
After 3 months of follow-up, of the 70 patients in the Obs group, only 1 patient had recurrence, with a recurrence rate of 1.43% (1/70), while 31 patients had recurrence, with a recurrence rate of 44.29% (31/70) in the Ctrl group. As demonstrated in Table 1, the patients in the Obs group after the FPST with curettage treatment presented a lower recurrence rate than those treated by pure curettage treatment (P<0.05).
Discussion
PDUB is a common gynaecological disease, and there are many clinical treatment options, among which FPST has been widely undertaken as a conservative treatment [11] [12] [13]. The results of this work suggested that FPST has an obvious curative effect in treating PDUB. First, patients in the Obs group showed great improvement in menstrual cycle and menstrual volume. This work revealed that the TER and CR of patients after the FPST with curettage treatment were 97.14% and 84.26%, while those for patients treated with pure curettage were 74.29% and 44.29%, respectively. This suggests that FPST can regulate the menstrual cycle and reduce menstrual volume by adjusting estrogen levels, thus alleviating the symptoms of PDUB. This is consistent with the findings of many previous studies, which verified the effectiveness of FPST in treating PDUB [14] [15]. All patients had no serious adverse reactions, and patients with mild adverse reactions were slightly more in the Obs group, but P>0.05. The incidence of adverse reactions in patients after the FPST with curettage treatment was 4.29% (3/70), and that was 2.86% (2/70) for patients who were treated with pure curettage treatment, showing no great difference (P>0.05). This indicates that FPST is relatively safe in clinical application, and adverse reactions are mild and tolerable [16]. However, it should be noted that the sample size enrolled herein was small, and the treatment duration was short. Further, large-scale and long-term follow-up studies are needed to fully evaluate its long-term safety [17].
As a conservative therapy for treating PDUB, FPST has significant clinical effects [18]. By adjusting estrogen levels, the menstrual cycle and menstrual volume can be improved, thus relieving symptoms of PDUB and improving the QOL of patients [19] [20]. Secreted by the pituitary gland, FSH can promote the increase of endogenous LH and E2 levels, thus leading to the imbalance of estrogen and progesterone levels. It was indicated that the FSH, LH, and E2 levels greatly decreased after different interventions, and the degree of decrease was more obvious after FPST treatment. These results indicate that FPST can regulate hormone imbalance in PDUB patients. In addition, FPST showed good safety and tolerance in this study. Compared with traditional hormone replacement therapy, FPST has the advantage that it can better simulate the natural menstrual cycle and avoid the discomfort and side effects that may be caused by continuous hormone replacement [21] [22].
Additionally, FPST uses the alternate application of estrogen and progesterone, avoiding hormone dependence and decreased tolerance that can result from the long-term use of a single hormone. This gives an ideal choice for clinical treatment. However, this work was subject to several limitations [23]. In clinical practice, FPST has shown good efficacy and safety in treating PDUB [24] [25]. However, more large-scale and long-term follow-up clinical studies are still needed to confirm its efficacy and safety further and compare it with other treatment methods that can better guide clinical practice [26] [27] [28]. Further research and discussion are needed on the individualized treatment plan for different patients, including the type, dosage, and course of estrogen-progesterone.
To discuss the physiological aspects of the effects seen by this treatment, the menstrual cycle is regulated by the hormones estrogen (estradiol) and progesterone (medroxyprogesterone acetate). During days 1–14, estradiol stimulates the growth and thickening of the uterine endometrium by binding to estrogen receptors, leading to increased cell proliferation, angiogenesis, and glycogen and lipid synthesis. From days 15–28, progesterone promotes differentiation and preparation of the endometrium for implantation by binding to progesterone receptors, leading to changes in gene expression, decidualization, and the production of prostaglandins. If pregnancy does not occur, the withdrawal of progesterone on days 29-30 leads to the shedding of the endometrium, resulting in menstruation. This complex interplay between estrogen and progesterone regulates various biological processes, including endometrial growth, angiogenesis, immune modulation, and withdrawal bleeding, and is essential for a healthy menstrual cycle [29].
Conclusion
In summary, supplementing with FPST in the process of implementing curettage treatment of PDUB can effectively improve clinical effects and reduce the recurrence rate, which is worthy of in-depth clinical research and promotion. Due to the small sample size and research limitations, further large samples were still needed to verify and improve this conclusion. Future studies should be conducted to explore the therapeutic mechanism of this therapy and apply it to clinical practice to assess its safety and efficacy more fully.
Dodatak
Funding
The research is supported by Wenyang stickers on spleen and kidney yang deficiency chronic bronchitis action mechanism research project number: 2014379, Patent Number: ZL 2015 1 0250209.8.
Conflict of interest statement
All the authors declare that they have no conflict of interest in this work.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1414542020201710.1080/13697137.2017.1358921 Goldstein S R Lumsden M A Climacteric Abnormal uterine bleeding in perimenopause 28780893 · doi ↗ · pubmed ↗
- 2627369202010.1016/j.bpobgyn.2020.05.004 Jewson M Purohit P Lumsden M A Best Pract Res Clin Obstet Gynaecol Progesterone and abnormal uterine bleeding/menstrual disorders 32698992 · doi ↗ · pubmed ↗
- 32016112016 Khan R Sherwani R K Rana S Hakim S Jairajpuri Z S Iran J Pathol Clinco-pathological patterns in women with dysfunctional uterine bleeding 26870139 PMC 4749191 · pubmed ↗
- 45816642202310.5937/jomb 0-37007 Balamurugan V Maradi R Joshi V Shenoy B V Goud M B K J Med Biochem Dyslipidaemia and inflammatory markers as the risk predictors for cardiovascular disease in newly diagnosed premenopausal hypothyroid women 36819139 PMC 9920932 · doi ↗ · pubmed ↗
- 5262032855201610.31729/jnma.2834 Sharma J Tiwari S JNMA J Nepal Med Assoc Hysteroscopy in Abnormal Uterine Bleeding vs Ultrasonography and Histopathology Report in Perimenopausal and Postmenopausal Women 27935919 · doi ↗ · pubmed ↗
- 61712472015 Van den Bosch T Ameye L Van Schoubroeck D Bourne T Timmerman D Facts Views Vis Obgyn Intra- cavitary uterine pathology in women with abnormal uterine bleeding: a prospective study of 1220 women 25897368 PMC 4402439 · pubmed ↗
- 76426720200510.1080/09513590400020963 Inan I Kelekci S Yilmaz B Gynecol Endocrinol Psychological effects of tibolone and sequential estrogen-progestogen therapy in perimenopausal women 15823823 · doi ↗ · pubmed ↗
- 83134 Nov 10; 112007 Jahedbozorgan T Hasanzadeh S Journal of Inflammatory Diseases Evaluation of bleeding patterns in postmenopausal women under continuous or sequential hormone therapy