The iron woman: a case report of contemporary cardiac support
Jeremy A Brooksbank, Nikolaos Spilias, Carmela D Tan, Randall C Starling, Samir Kapadia

TL;DR
This case report describes a female patient with severe heart failure who received multiple advanced cardiac treatments before undergoing a heart transplant.
Contribution
The novelty lies in the comprehensive documentation of sequential device-based therapies applied in a single patient with advanced heart failure.
Findings
The patient received a full range of device-based therapies for heart failure and mitral regurgitation.
The case highlights the progression from temporary to durable mechanical support and eventual heart transplantation.
The report reviews indications and anatomical considerations for various cardiac devices.
Abstract
Modern cardiovascular practice utilizes various devices and procedures to treat functional and structural heart disease. We report an interesting case of a female patient with heart failure with reduced ejection fraction (HFrEF) and severe mitral regurgitation who received the full spectrum of available device-based therapies including mitral transcatheter edge-to-edge repair, percutaneous mitral annuloplasty with the Carillon device, temporary mechanical circulatory support, durable left ventricular assist device, and eventually cardiac transplantation. Management of HFrEF and functional mitral regurgitation is a common clinical issue for which numerous devices may be utilized to improve patient symptoms and outcomes. In this report, we review indications, supporting data, and anatomical relationships of some of these devices. We also highlight stepwise progression to advanced heart…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1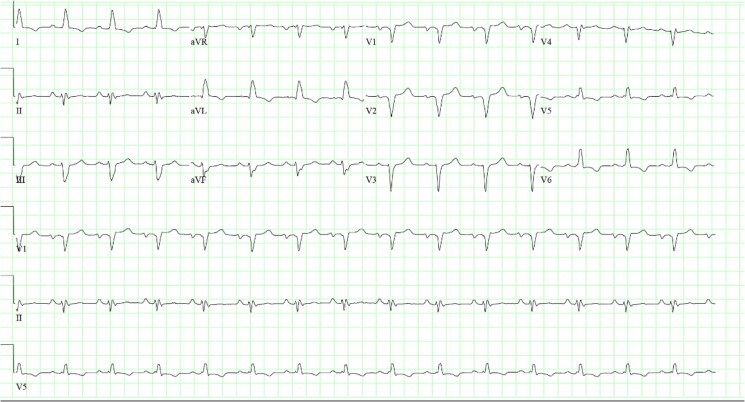 Figure 1
Figure 1 Figure 2
Figure 2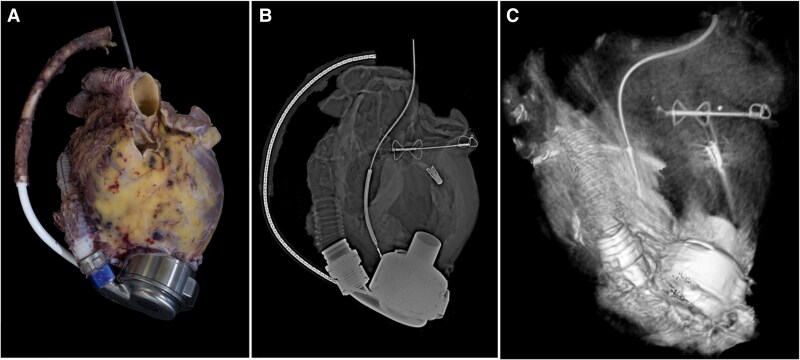 Figure 3
Figure 3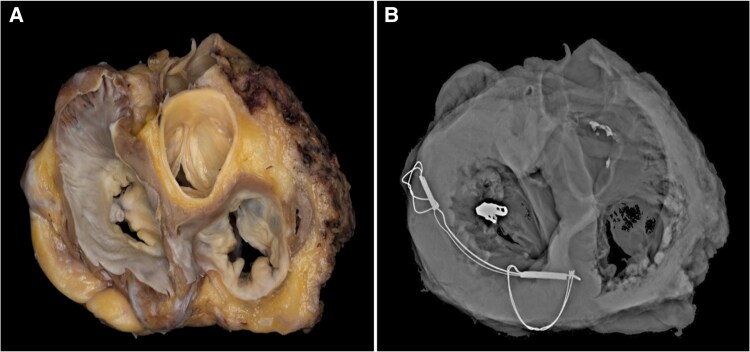 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac pacing and defibrillation studies · Cardiac Structural Anomalies and Repair · Acute Myocardial Infarction Research
Introduction
Modern cardiovascular practice utilizes various devices and procedures to treat functional and structural heart disease. We report an interesting case of a female patient with advanced heart failure with reduced ejection fraction (HFrEF) and severe mitral regurgitation (MR) who received the full spectrum of available device-based therapies including mitral transcatheter edge-to-edge repair (TEER), percutaneous mitral annuloplasty with the Carillon^©^ device, temporary mechanical circulatory support (MCS), durable left ventricular assist device (LVAD), and eventually cardiac transplantation.
Summary figure
**
Case presentation
A 68-year-old Caucasian woman with a history of ischaemic heart disease presented with one month of worsening New York Heart Association (NYHA) class III dyspnoea, orthopnoea, and palpitations. The patient had a past medical history of hypertension, premature ventricular contractions, and a large anteroseptal myocardial infarction (MI) at the age of 36 which was attributed to coronary vasospasm. Six months following MI, her left ventricular ejection fraction (EF) was 35%. She was followed intermittent by her primary care physician and maintained on medical therapy consisting of metoprolol succinate and losartan. She reported infrequent palpitations and dyspnoea on exertion, but had no other emergency department visits or hospitalizations in the 32 years since her MI.
On presentation to our facility, the patient had normal jugular venous pulsations, clear lungs, 1+ peripheral oedema, normal S1/S2 heart sounds, and a laterally displaced point of maximal intensity. ECG revealed sinus rhythm with left atrial enlargement and left bundle-branch block with QRS duration 122 ms (Figure 1). The patient underwent transthoracic echocardiography (TTE) which revealed reduced EF 24% with LV end-diastolic dimension (LVEDD) 7.0 cm and moderate-to-severe (3+) secondary MR. Left heart catheterization showed mild, non-obstructive coronary artery disease. Right heart catheterization revealed normal filling pressures [mean right atrial pressure 5 mmHg, pulmonary artery (PA) 42/12 (mean 22) mmHg, and mean pulmonary artery wedge pressure 10 mmHg] and severely reduced cardiac index (1.61 mL/min/m^2^). PA pulsatility index was normal at 6.0. She had additional optimization of guideline-directed medical therapy (GDMT) with maximally tolerated doses of metoprolol succinate (50 mg daily), transition to sacubitril–valsartan (24/26 mg twice daily), and initiation of spironolactone (25 mg daily) and dapagliflozin (10 mg daily). These medication changes led to improvement in symptoms, and she was discharged from the hospital with regular outpatient follow-up. Three months after medical optimization, TTE was repeated and showed interval improvement in EF to 45%.
ECG upon presentation. Normal sinus rhythm with LBBB with QRS duration 122 ms.
The patient remained stable for 24 months prior to worsening symptoms prompting hospitalization. Transthoracic echocardiography at that time revealed reduction of EF to 20%, RV mildly dilated with normal systolic function, severe left atrial enlargement, and severe secondary MR due to apical tethering of the mitral leaflets in the setting of severe LV enlargement (LVEDD 7.8 cm). Transoesophageal echocardiogram showed structurally normal mitral leaflets with 4+ secondary MR (effective regurgitant orifice area 0.42 cm^2^) and holosystolic flow reversal in all pulmonary veins. After optimization of volume status with intravenous diuretics and appropriate adjustment of GDMT, a single-chamber implantable cardiac defibrillator (ICD) was placed for primary prevention of sudden cardiac death as EF remained <35%. Given these findings and after multidisciplinary heart team approach, she underwent mitral TEER with the deployment of 1 MitraClip (Abbott®) grasping the A2/P2 scallops of the mitral valve. The MR improved from 4+ to 1–2+ but worsened again a few months later leading to recurrent HF admissions. Transthoracic echocardiography showed a well-seated MitraClip device with moderate–severe MR and progressive mitral annular dilatation and LV enlargement. She then underwent compassionate percutaneous indirect mitral annuloplasty with placement of 80 mm Carillon mitral contour system (Cardiac Dimensions) in the coronary sinus, with the goal to reduce the dimensions of the mitral annulus and improve the LV geometry and MR. Echocardiographic images included in Supplementary material section, Videos S1 and S2.
Despite temporary improvement in symptoms and MR following percutaneous mitral annuloplasty, she had progression of LV size and MR severity leading to stage D heart failure. Metabolic testing revealed adequate effort with respiratory exchange ratio (RER) 1.52 with peak oxygen uptake (pVO2) of 10.1 mL/kg/min (52% predicted) and minute-ventilation to carbon dioxide production ratio (VE/VCO2) slope 42. She was subsequently listed for cardiac transplantation or bridge-to-transplant LVAD. Prior to acceptable organ offer, she was admitted with cardiogenic shock and pulmonary artery catheter placement revealed RA 7 mmHg, pulmonary capillary wedge pressure (PCWP) 23 mmHg with pronounced v waves to >40 mmHg, and reduced CO (2.8) and CI (1.72).
She was stabilized with intra-aortic balloon pump (IABP) and subsequently underwent LVAD placement during admission. Thirteen months later, she underwent orthotopic heart transplantation (OHT). Please see Figure 2 for clinical timeline. The explanted heart with its hardware underwent routine analysis and processing by the pathology department. Pathologic examination confirmed remote anteroseptal MI without significant coronary atherosclerosis. The mitral valve demonstrated one intact clip at A2/P2 scallops and a well-endothelialized Carillon device present in the coronary sinus. Pathologic specimens with corresponding gross, radiographic, and tomographic imaging are shown in Figures 3 and 4.
Summary figure with clinical timeline.
Gross anatomy of removed heart and associated supportive devices following heart transplantation. Image A is the gross pathologic images with corresponding radiographic (B) and CT reconstruction (C).
Short-axis view of gross anatomic specimen and corresponding radiographic image showing the three-dimensional relationship of cardiac anatomy and support devices.
The patient recovered well after the OHT, with significant clinical improvement and improvement in quality of life. Routine surveillance endomyocardial biopsies showed subclinical 2R cellular rejection without any evidence of graft dysfunction at 1 week and 6 months post-transplant. The patient is having routine post-OHT follow-up.
Discussion
This case highlights the contemporary device therapies for patients with severe cardiomyopathy/HFrEF and concomitant functional mitral regurgitation, which are provided within the context of a multidisciplinary heart team consisting of heart failure cardiologists, cardiac imagers, interventional cardiologists, and cardiac surgeons. It also provides a visual demonstration and understanding of the anatomic relationship between the different devices that can be used to treat advanced heart failure and prevent sudden cardiac death in the contemporary era, such as the ICD, the MitraClip device, the Carillon mitral contour system, and the LVAD.
Although the cornerstone of HFrEF management is optimization of GDMT, the response to GDMT remains variable, with progression of heart failure and increased morbidity and mortality in certain cases. With the exponential growth of structural heart interventions, minimally-invasive, device-based therapies have been developed and established for the treatment of HFrEF. Despite maximally tolerated GDMT, our patient continued to demonstrate clinical deterioration and progression of functional mitral regurgitation, leading to mitral TEER.
The 2022 AHA/ACC/HFSA guidelines denote a class IIa recommendation for transcatheter edge-to-edge MV repair (TEER) in patients with persistent NYHA class II–IV symptoms despite optimal GDMT and appropriate valvular anatomy with EF 20%–50%, LV end-systolic diameter (LVESD) ≤ 70 mm, and PA systolic pressure ≤ 70 mmHg.^1^
Despite initial improvement after TEER, continued LV dilation and MR progression may eventually ensue. The Carillon device (Cardiac Dimensions®) is a mitral annular reduction system which is implanted percutaneously in the coronary sinus with the goal to achieve reverse LV remodelling and MR reduction. The Carillon device was initially studied in the Titan I and Titan II trials to demonstrate device safety and efficacy.^2–4^ The randomized, sham-control, double-blinded REDUCE FMR Trial showed a reduction in MR and LV volumes with percutaneous mitral annuloplasty as assessed by echocardiography at 12 months.^5^ The ongoing, randomized, sham-controlled EMPOWER clinical trial will assess the effect of the Carillon mitral contour system in cardiovascular outcomes and LV remodelling in ∼300 patients with dilated cardiomyopathy and at least 1+ MR. The device was implanted via compassionate use in our patient and as a potential bridge to advanced heart failure therapies. Ultimately, and despite all the pharmacologic and device therapies, our patient progressed to stage D heart failure, requiring temporary MCS (IABP), LVAD placement, and eventually OHT.
The management of patients with HFrEF and secondary MR remains a challenge and requires the utilization of pharmacologic and device-based therapies within the context of the multidisciplinary heart team. A thorough understanding of the anatomy and mechanism of action of the available percutaneous and surgical devices is required for the timely selection of the appropriate therapy. Detailed examination of explanted hearts from patients undergoing heart transplantation may facilitate further understanding of function and anatomical relationships of current devices.
Supplementary Material
ytaf371_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Heidenreich PA, Bozkurt B, Aguilar D, Allen LA, Byun JJ, Colvin MM, et al 2022 AHA/ACC/HFSA guideline for the management of heart failure: a report of the American College of Cardiology/American Heart Association Joint Committee on clinical practice guidelines. Circulation 2022;145:e 895–e 1032.35363499 10.1161/CIR.0000000000001063 · doi ↗ · pubmed ↗
- 2Schofer J, Siminiak T, Haude M, Herrman JP, Vainer J, Wu JC, et al Percutaneous mitral annuloplasty for functional mitral regurgitation: results of the CARILLON Mitral Annuloplasty Device European Union Study. Circulation 2009;120:326–333.19597051 10.1161/CIRCULATIONAHA.109.849885 PMC 3954526 · doi ↗ · pubmed ↗
- 3Siminiak T, Wu JC, Haude M, Hoppe UC, Sadowski J, Lipiecki J, et al Treatment of functional mitral regurgitation by percutaneous annuloplasty: results of the TITAN trial. Eur J Heart Fail 2012;14:931–938.22613584 10.1093/eurjhf/hfs 076PMC 3403476 · doi ↗ · pubmed ↗
- 4Krishnaswamy A, Kapadia SR. Indirect mitral annuloplasty using the carillon device. Front Cardiovasc Med 2020;7:576058.33330643 10.3389/fcvm.2020.576058 PMC 7715026 · doi ↗ · pubmed ↗
- 5Witte KK, Lipiecki J, Siminiak T, Meredith IT, Malkin CJ, Goldberg SL, et al The REDUCE FMR trial: a randomized sham-controlled study of percutaneous mitral annuloplasty in functional mitral regurgitation. JACC Heart Fail 2019;7:945–955.31521683 10.1016/j.jchf.2019.06.011 · doi ↗ · pubmed ↗