Co-Infection of Pulmonary Aspergillosis and Cryptococcal Meningitis in an HIV-Positive Patient: A Case Report
Marjan Hemmatian, Sadegh Khodavaisy, Hossein Kazemizadeh, Behnaz Jahanbin, Reza Ershadi, Maryam Moradi, Mohammadreza Salehi, Jianping Xu, Megan Hitchcock, Kazem Ahmadikia, Ali Ahmadi, Seyed Ali Dehghan Manshadi

TL;DR
This case report describes an HIV patient with a very low immune cell count who developed two serious fungal infections at the same time.
Contribution
The novelty lies in documenting a rare co-infection of pulmonary aspergillosis and cryptococcal meningitis in a late-diagnosed HIV patient.
Findings
The patient had both pulmonary aspergillosis and cryptococcal meningitis.
The infections occurred in an HIV-positive individual with a CD4 count below 100.
This case highlights the risk of multiple opportunistic fungal infections in late-diagnosed HIV patients.
Abstract
Opportunistic fungal infections (OFIs) are common among human immunodeficiency virus (HIV) –positive patients, especially in those with delayed diagnosis and treatment. Patients with severe HIV/AIDS with clusters of differentiation 4 (CD4) counts less than 100 are significantly prone to develop multiple OFIs. In the current study, we present a case of co-infection of pulmonary aspergillosis and cryptococcal meningitis in a late-diagnosed HIV patient with a low CD4 count.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1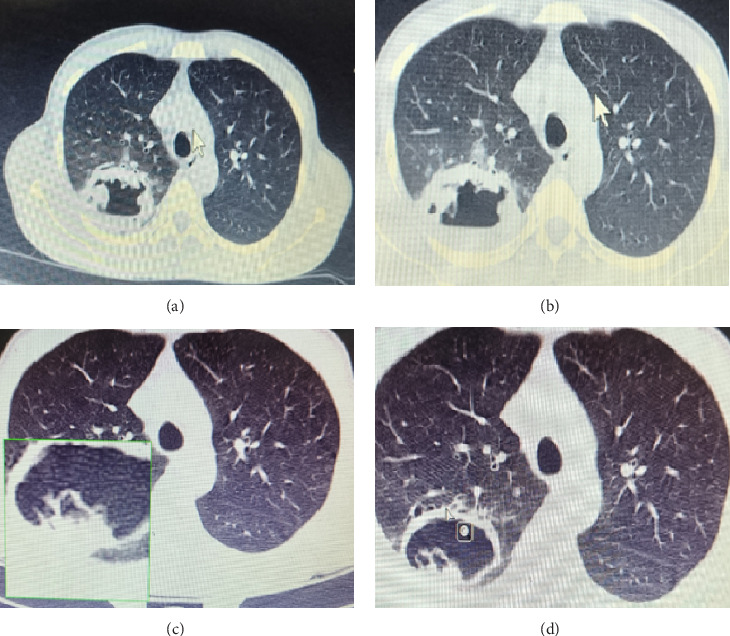 Figure 2
Figure 2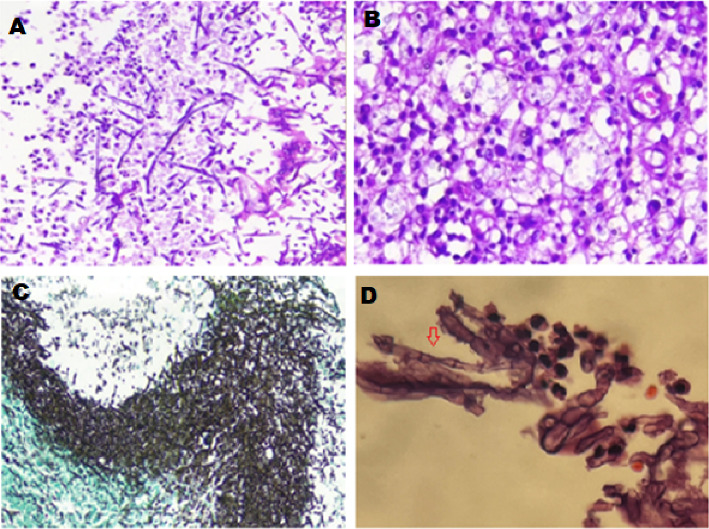 Figure 3
Figure 3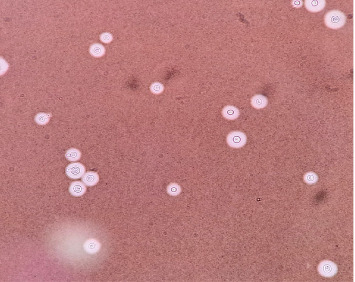 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFungal Infections and Studies · Antifungal resistance and susceptibility · Pneumocystis jirovecii pneumonia detection and treatment
1. Introduction
Human immunodeficiency virus (HIV) substantially predisposes patients to a variety of opportunistic infections, including fungal infections. Pneumocystosis, candidiasis, cryptococcosis, and histoplasmosis are the most frequent fungal infections observed among HIV-positive patients. Although the incidence of opportunistic infections is declining in response to the broad adoption of highly active antiretroviral therapy (HAART), fungal infections are still a great concern among immunocompromised patients [1, 2]. Cryptococcosis is an invasive fungal infection estimated to be the second-leading cause of death among HIV/AIDS patients [3]. This infection is caused by yeasts in the pathogenic Cryptococcus species complex, which was recently classified as a critical priority fungal pathogen by the World Health Organization (WHO) [4, 5]. Though often fatal, aspergillosis, an infection most frequently caused by the mold Aspergillus fumigatus, has not been considered a major opportunistic infection among HIV/AIDS patients since 1984. Nonetheless, aspergillosis and other invasive mold infections are observed among HIV-positive patients who undergo neutropenia or chronic corticosteroid therapy [6, 7]. Although opportunistic fungal infections (OFIs) are common among HIV-positive patients, co-fungal infections are rarely reported. In this report, we describe the clinical and paraclinical characteristics of an HIV-positive patient without a history of neutropenia, who developed both pulmonary aspergillosis (PA) and cryptococcal meningitis within 1 month.
2. Case Presentation
A 46-year-old homosexual man was presented to the emergency ward with a productive cough, fever, weight loss, and oral candidiasis reported in the three months before his visit. Considering the risk factors, an infectious disease specialist was consulted, and a rapid lateral flow assay (LFA) HIV test was requested and returned positive. HIV infection was confirmed with a fourth-generation ELISA. Initial immunologic staging showed a cluster of differentiation 4 (CD4) count of 41 cells/μL. The patient was conscious and oriented for baseline physical examination with the following vital signs: a fever with 38 °C body temperature, a heart rate of 100/min, a respiratory rate of 20/min, a blood pressure of 90/60 mmHg, and an oxygen saturation level of 94%. The chest computed tomography (CT) findings were clear, and no lymphadenopathy, hepatosplenomegaly, or skin lesions were found. The baseline laboratory test results of the patient's blood are summarized in Table 1. On the first day of admission, intravenous piperacillin-tazobactam 4.5 mg every 6 h alongside a 4-drug regimen of antituberculosis (TB) was initiated (isoniazid 300 mg/daily, rifampin 600 mg/daily, pyrazinamide 1500 mg/daily, and ethambutol 800 mg/daily). A chest X-ray and CT scan of the chest revealed a cavitary lesion in the posterior segment of the right upper lobe (Figures 1 and 2(a), 2 (b), 2 (c), and 2(d)). Therefore, a 3x sputum smear for TB diagnosis, TB GeneXpert, and serum cryptococcal antigen (CrAg) test were requested, all of which tested negative. Nonetheless, because of the cavitary lesion in the lung, bronchoscopy and bronchoalveolar lavage (BAL) were performed alongside TB-specific PCR to further rule out TB and other microbial etiologies. The tests were negative for both bacterial and fungal agents in the BAL specimen (Table 2). Despite anti-TB and antibiotic therapy, the patient's clinical condition did not show improvement. Therefore, the chest CT scan was repeated. Based on the second CT scan and radiologic consultation, a hydatid cyst was suspected. The serum Echinococcus antigen and antibody were both reported as negative. Nineteen days after admission, intravenous piperacillin-tazobactam and anti-TB regimen were discontinued, and Truvada (a combination of emtricitabine and tenofovir disoproxil fumarate), dolutegravir, and albendazole were started.
In the following days, a gradual deterioration with the onset of new respiratory signs was observed. Based on this decline, the decision for the patient to undergo a thoracotomy and segmentectomy was made. Surgery found the macroscopic appearance of the lesion not consistent with a hydatid cyst. Pathological examination with hematoxylin and eosin (H&E) of the lung biopsy revealed nonpigmented narrow branching septate hyphae and yeast with budding cells in alveolar macrophages. Also, Grocott–Gomori's methenamine silver (GMS) stain was used to indicate septate hyphae character and whether the yeast forms could represent Cryptococcus or another yeast pathogen in the lung biopsy. Stepwise differential diagnoses of aspergillosis, fusariosis, and Pseudallescheria species were performed (Figures 3(A), 3(B), 3(C), and 3(D)). The first step in fungal differential diagnosis used Aspergillus-specific PCR, which presented positive. Therefore, albendazole was discontinued, and treatment shifted to oral voriconazole 200 mg every 12 h. After 1 month of hospitalization, the patient was discharged and continued with HAART therapy and voriconazole treatment. After 2 weeks, the patient reported severe headache, restlessness, shivering, fever, and blurred and double vision. Neurological and ophthalmological exams were all normal. The patient underwent a brain CT scan with and without contrast to rule out brain abscesses or mass lesions, followed by a lumbar puncture (LP) (Table 3 and Figure 4). Encapsulated yeast cells were detected on direct examination stained with Indian ink (Figure 4). CrAg detection using LFA and direct molecular detection by the 21-plex PCR method on CSF samples was positive for cryptococcosis, which all yielded consistent proof for cryptococcal meningitis. The isolated Cryptococcus strain (TMML 3988) underwent multilocus sequence typing, which is a common method used to identify Cryptococcus by analyzing portions of seven housekeeping genes (CAP59, GPD1, LAC1, PLB1, SOD1, URA5, and IGS1) [8]. Examination of the URA5 gene identified the isolate as Cryptococcus neoformans [9]. Due to antigen properties, this species of Cryptococcus is commonly referred to as Serotype A and is the most clinically relevant species of Cryptococcus worldwide [10]. This isolate was further designated as C. neoformans molecular type VNI. This specific group of Cryptococcus is reportedly responsible for ∼95% of all cryptococcal infections worldwide [11]. The allele type (AT) at each of the seven MLST loci was determined (CAP59 = AT7, GPD1 = AT5, LAC1 = AT3, PLB1 = AT3, SOD1 = AT1, URA5 = AT1, and IGS1 = AT1). Based on these results, the complete MLST profile was matched to sequence type (ST) ST69 [12]. Accordingly, 5 mg/kg of liposomal amphotericin B plus 800 mg of fluconazole was started for the patient due to the lack of 5-fluorocytosine access in Iran. The patient's clinical condition deteriorated, and 24 h later, the patient unfortunately died.
3. Discussion
HIV-positive patients, specifically those with a CD4 count less than 200, are at manifold risk of developing fungal infections. In this population, fungal infections are the major cause of morbidity and mortality. The clinical form of OFI in HIV-positive patients ranges from superficial involvement such as oral candidiasis to disseminated forms such as cryptococcosis [13]. Among fungal infections, aspergillosis is a rare complication in HIV-positive patients and is primarily associated with HIV-positive individuals experiencing co-factors, including neutropenia, chronic corticosteroid use, pneumocystis, CMV infection, CD4 count < 100 cells/mm3, and delayed treatment. The most common presentation of HIV-associated aspergillosis occurs in the lungs. However, involvement has also been reported with the central nervous system (CNS), heart, kidneys, and sinuses [14]. Our patient who presented with a cavitary lesion, productive cough, and fever responded well to voriconazole. Therefore, in HIV-positive patients, specifically those with a profoundly diminished CD4 count, cough, fever, and cavitary lung lesion, aspergillosis should be considered in the differential diagnosis [7]. To our knowledge, this is the first report of ST69 within Iran and the second report within the Middle East, with a previous report of ST69 identified in Kuwait. In addition, ST69 is the ninth most commonly reported ST worldwide, identified in parts of Europe, Asia, Africa, and South America [15]. The incidence of aspergillosis in a large-scale study of HIV-infected patients was observed to be 3.5 cases per 1000 person-years. AIDS-associated aspergillosis is typically accompanied by a low CD4 count (less than 100 cells/mm^3^), and in about half of the HIV-associated aspergillosis cases, there is concurrent neutropenia or use of corticosteroid therapy. In the remaining cases, advanced AIDS is the only apparent risk factor. Since the isolation of Aspergillus from respiratory secretions does not reliably indicate invasive PA in AIDS patients, a histopathological diagnosis is usually necessary to verify the condition. Unfortunately, the prognosis for HIV-infected patients with PA is generally poor, with a median survival time of 3 months following diagnosis. As observed in this case, an increase in size or number of lesions detected by chest radiographs/CT, elevated serological biomarkers (antibody or antigen), and large volume hemoptysis are often associated with poor prognosis of PA [14]. CM is a critical neurological infection typically associated with advanced HIV/AIDS and is responsible for 15% of mortality among HIV/AIDS patients [16, 17]. Based on the time of HAART initiation and the disease presentation, we believed that unmasking immune reconstitution inflammatory syndrome (IRIS) was responsible for our patient's cryptococcal meningitis. Despite the low probability, it is necessary to consider co-infection in HIV-positive patients who do not show any improvement with standard treatments or patients who present new symptoms or exacerbation [18]. The local stigma that exists toward homosexual patients and the lack of awareness lead to late diagnosis and treatment of HIV and put the patients at manifold risk for serious complications such as life-threatening opportunistic infections. Therefore, it is essential to identify and educate these susceptible groups of patients. The WHO and IDSA guidelines highly urge CrAg screening for HIV-positive individuals with CD4 levels of ≤ 100 cells/μL [19, 20]. Preemptive CrAg screening remains a critical strategy to reduce mortality, but in some settings, such as Iran, implementation is limited due to resource constraints and the lack of routine screening in national HIV programs.
In conclusion, the detection of several systemic mycoses demonstrates the vulnerability of advanced HIV-positive patients. The introduction of HAART and primary prophylaxis for opportunistic infections has improved the quality of life in these individuals.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Almeida-Silva F. Damasceno L. S. Serna M. J. Multiple Opportunistic Fungal Infections in an Individual With Severe HIV Disease: A Case Report Revista Iberoamericana De Micologia 201633211812110.1016/j.riam.2015.09.0012-s 2.0-8495857675626896884 · doi ↗ · pubmed ↗
- 2Limper A. H. Adenis A. Le T. Harrison T. S. Fungal Infections in HIV/AIDS The Lancet Infectious Diseases 20171711 e 334e 34310.1016/s 1473-3099(17)30303-12-s 2.0-8502651647228774701 · doi ↗ · pubmed ↗
- 3Rajasingham R. Smith R. M. Park B. J. Global Burden of Disease of HIV-Associated Cryptococcal Meningitis: An Updated Analysis The Lancet Infectious Diseases 201717887388110.1016/s 1473-3099(17)30243-82-s 2.0-8501878682228483415 PMC 5818156 · doi ↗ · pubmed ↗
- 4WHOWHO Fungal Priority Pathogens List to Guide Research, Development and Public Health Action WHO 20221148
- 5Negroni R. Cryptococcosis Clinics in Dermatology 201230659960910.1016/j.clindermatol.2012.01.0052-s 2.0-8486758792223068147 · doi ↗ · pubmed ↗
- 6Klapholz A. Salomon N. Perlman D. C. Talavera W. Aspergillosis in the Acquired Immunodeficiency Syndrome Chest 199110061614161810.1378/chest.100.6.16142-s 2.0-00264095671959405 · doi ↗ · pubmed ↗
- 7Miller W. T.Jr. Sais G. J. Frank I. Gefter W. B. Aronchick J. M. Miller W. T. Pulmonary Aspergillosis in Patients With AIDS Chest 19941051374410.1378/chest.105.1.372-s 2.0-00280493578275779 · doi ↗ · pubmed ↗
- 8Meyer W. Aanensen D. M. Boekhout T. Consensus Multi-Locus Sequence Typing Scheme for Cryptococcus Neoformans and Cryptococcus Gattii Medical Mycology 200947656157010.1080/136937809029538862-s 2.0-7084910146019462334 PMC 2884100 · doi ↗ · pubmed ↗