An 80-year-old female with multiple mononeuropathy: neuroleukemiosis a rare complication of chronic lymphocytic leukaemia
Caroline Morgan, Venkataramanan Srinivasan, Ute Pohl, Benjamin R Wakerley

TL;DR
An 80-year-old woman with chronic lymphocytic leukemia developed a rare nerve condition called neuroleukemiosis, confirmed through biopsy.
Contribution
This case highlights neuroleukemiosis as a rare complication of chronic lymphocytic leukemia.
Findings
The patient presented with painful footdrop and multiple mononeuropathy.
A nerve biopsy confirmed small lymphocyte infiltration in the epineurium and perineurium.
The diagnosis of neuroleukemiosis was established based on clinical and pathological findings.
Abstract
We report the case of an 80-year-old lady with chronic lymphocytic leukaemia who presented with painful footdrop. Nerve conduction studies and electromyography confirmed the presence of multiple mononeuropathy. Left superficial radial nerve biopsy revealed small lymphocytes infiltrating the epineurium and perineurium and confirmed a diagnosis of neuroleukemiosis.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
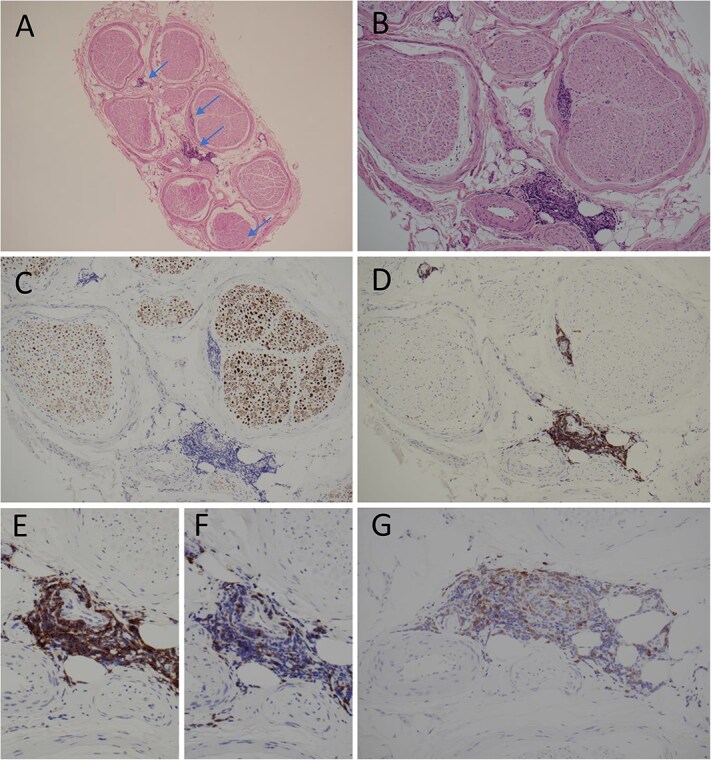 Figure 1
Figure 1| Sensory nerve | Lat | Amp | CV |
|---|---|---|---|
| ms | μV | m/s | |
| CTS Sensory Left | |||
| Med. Index—Wrist | 2.59 | 1.17 | 44.4 |
| CTS Sensory Right | |||
| Med. Index – Wrist | 2.75 | 4.6 | 41.8 |
| Dig plant med Sensory Left | |||
| Sole – Ankle | 2.65 | 3.1 | — |
| Dig plant med Sensory Right | |||
| Sole – Ankle | — | NR | |
| Peroneus superficial Sensory Left | |||
| Lower leg – Ankle | 2.00 | 4.2 | 50.0 |
| Peroneus superficial Sensory Right | |||
| Lower leg – Ankle | 1.44 | 20.3 | 59.0 |
| Suralis Sensory Left | |||
| Mid. Lower leg – Ankle | 1.92 | 15.9 | 49.5 |
| Suralis Sensory Right | |||
| Mid. Lower leg – Ankle | 1.85 | 17.5 | 48.6 |
| Nerve | Lat | Amp | CV | Dur |
|---|---|---|---|---|
| ms | mV | m/s | ms | |
| Median (Lumbricals) Motor Left | ||||
| Median(wrist)—2nd Lumbrical | 4.15 | 0.63 | 4.0 | |
| Median (Lumbricals) Motor Right | ||||
| Median(wrist)—2nd Lumbrical | 3.86 | 1.29 | 4.8 | |
| Medianus Motor Left | ||||
| Wrist—APB | 4.59 | 1.34 | 6.1 | |
| Medianus Motor Right | ||||
| Wrist—APB | 4.19 | 7.0 | 4.5 | |
| Peroneal TA Motor Left | ||||
| Fib. Head—TA | 5.77 | 0.47 | 9.4 | |
| Popliteal Fossa-Fib. Head | 9.95 | 0.14 | 12.0 | 10.2 |
| Peroneal TA Motor Right | ||||
| Fib. Head—TA | 2.77 | 10.1 | 13.4 | |
| Peroneus Motor Left | ||||
| Ankle—EDB | 3.79 | 6.1 | 6.0 | |
| Fib. head-Ankle | 10.9 | 5.7 | 43.6 | 6.5 |
| Peroneus Motor Right | ||||
| Ankle—EDB | — | — | — | |
| Fib. head-Ankle | — | — | — | — |
| Tibialis Motor Left | ||||
| Ankle—Abd hal | 4.78 | 9.8 | 5.0 | |
| Knee-Ankle | 5.13 | 9.6 | — | 4.9 |
| Tibialis Motor Right | ||||
| Ankle—Abd hal | 10.7 | 0.28 | 4.5 | |
| Ulnar FDI Motor Left | ||||
| Wrist—FDI | 3.85 | 5.6 | 5.4 | |
| Bl. Elbow-Wrist | 8.76 | 2.9 | 41.8 | 5.4 |
| Ab. Elbow-Bl. Elbow | 11.6 | 2.9 | 28.2 | 6.1 |
| Ulnar FDI Motor Right | ||||
| Wrist—FDI | 3.71 | 5.0 | 4.5 | |
| Bl. Elbow-Wrist | 8.60 | 4.6 | 41.9 | 4.2 |
| Ab. Elbow-Bl. Elbow | 10.5 | 4.7 | 42.1 | 4.6 |
| Muscle | IA | Fib | PSW | Fasc | Amp | Dur | Poly | Recruit |
|---|---|---|---|---|---|---|---|---|
| Right Abd dig min | 2+ | 2+ | None | + | + | None | Reduced | |
| Left Abd dig min | 1+ | 1+ | None | + | + | Few | Reduced | |
| Right Adductor hallucis | 2+ | 2+ | None | + | + | None | Reduced | |
| Left Flex dig longus | 1+ | 2+ | None | + | + | Few | Reduced | |
| Right Gastroc (med) | None | None | None | N/+ | N/+ | Few | Reduced | |
| Left Gastroc (med) | Incr | None | None | None | + | + | Few | Reduced |
| Right Peroneus longus | None | None | None | + | + | Many | Reduced | |
| Left Peroneus longus | 1+ | 1+ | None | + | + | None | Reduced | |
| Right Tibialis anterior | None | None | None | + | + | Many | Reduced | |
| Left Tibialis anterior | 2+ | 2+ | None | − | − | − | − |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsChronic Lymphocytic Leukemia Research · CNS Lymphoma Diagnosis and Treatment · Lymphoma Diagnosis and Treatment
Introduction
Neuroleukemiosis, defined as the infiltration of leukaemia in the peripheral nerve structures [1], is an extremely rare complication in leukaemia and when present, more common in acute leukaemia compared to chronic lymphocytic leukaemia (CLL). Decision for treatment of CLL depends on staging criteria and signs and symptoms of active disease [2]. Patients who are Rai stage 0 (low risk) or Rai stage I or II (intermediate risk) are often monitored without treatment.
Here, we report a case of neuroleukemiosis in CLL, causing multiple mononeuropathy.
Case presentation
An 80-year-old lady had a diagnosis of CLL—under 6 monthly surveillance. Rai stage I due to enlarged lymph nodes. She presented 20 months after diagnosis with painful left foot drop and left foot paraesthesia. She initially experienced paraesthesia in the right-hand fingertips 12 months following diagnosis. This was followed by reduced sensation on the dorsum of the right foot and pain. She then experienced left hand paraesthesia in the fingertips and inability to do fine motor tasks due to weak grip strength. At 18 months post diagnosis, she developed left painful foot drop which progressively worsened, prompting neurology assessment. Examination revealed reduced vibration sense in left thumb, power in left ankle dorsiflexion and toe extension 0/5, but normal eversion, inversion, and plantar flexion. On the right side, abductor hallucis was significantly weak although plantar flexion was reasonably well preserved. Submandibular lymphadenopathy was present with no organomegaly.
Investigations
B12, folate and HbA1c were normal. Blood borne virus screen was negative. Vasculitis screen revealed raised Myeloperoxidase- ANCA antibodies. Cerebrospinal fluid was unremarkable and flow cytometry revealed no evidence of clonal lymphoid cells. MRI head and whole spine revealed no abnormalities. CT Thorax-Abdomen-Pelvis revealed extensive thoracic, abdominal, pelvic and groin adenopathy in keeping with a lymphoproliferative disorder. PET-CT revealed mildly avid lymphadenopathy on both sides of the diaphragm without FDG avid bone or splenic involvement.
Nerve conduction studies (Tables 1 and 2) and electromyography (Table 3) were suggestive of bilateral median nerve dysfunction at the level of the wrist and ulnar nerve dysfunction across the left elbow and an axonal lesion of the left median nerve. All the motor and sensory responses distal to the ankle were significantly reduced on the right side with more pronounced ongoing denervation activity in the right foot muscles as compared to the left foot muscles or proximal tibial nerve-innervated muscle. Left superficial peroneal sensory and motor response from left TA response was significantly reduced on the left side, ongoing denervation activity and chronic neurogenic changes were noted in a patchy manner in left lower limb muscles. In summary, the findings supported a patchy asymmetric sensory-motor axonal neuropathy specifically in the clinically symptomatic regions of the lower limbs i.e. left hand, left common peroneal nerve and distal segment of the right tibial nerve (distal to ankle). This raised a strong possibility of multiple mononeuropathy secondary to leukemic infiltration.
Left superficial radial nerve biopsy revealed neither vasculitis nor significant axonal or demyelinating neuropathy. However, the epineurium and perineurium showed a patchy perivascular infiltration by small lymphocytes with a predominant B-cell component which stained positive for B-cell marker CD20, CD5 and CD23 (Fig. 1). The appearances were diagnostic of CLL infiltrating the peripheral nerves.
Histology of transected superficial radial nerve involved by CLL. (A and B); HE stains showing multifocal lymphocytic infiltrates (arrows; ×40 and ×100 mag. Respectively); (C), immunohistochemistry (IHC) for neurofilament reveals mild reduction of axons (x100 mag.); (D and E), IHC for CD20 highlights predominant B-cell component of perivenular infiltrates (×100 and ×200 mag., respectively); (F), IHC for CD3 shows scanty positive cells compatible with reactive T-cells (×200 mag.); (G), IHC reveals weak to moderate CD5 positivity in the majority of B-cells (x200 mag.) with coexpression of CD23 (the latter is not illustrated).
Discussion
Neuroleukemiosis in CLL is rare, with only 6 previous reports in the literature [3–7]. Of these case reports, five already had a diagnosis of CLL prior to identification of neuroleukemiosis [3–6] and one had neuroleukemiosis as the clinical presentation for CLL [7]. Four cases were identified by nerve biopsy [3, 5–7], one identified by a mass lesion on MRI, which further revealed avid uptake on PET [5] and one identified by autopsy [4].
Nerve biopsy remains the gold standard for confirmation of peripheral nerve infiltration. However, the results may be negative or non-specific due to the patchy nature of infiltration. Cases have been reported with negative sural nerve biopsy, despite sural nerve involvement, suggesting the focal infiltration of the nerve and requirement of biopsy of the specifically affected part of the nerve [8]. Case reports have suggested that a target for biopsy may be revealed by positive MRI or PET-CT findings [9]. However, in this case MRI and PET-CT were negative so the target for biopsy was identified by the neurophysiology results. The sural nerve was of normal amplitude so the superficial radial nerve was chosen, and biopsy was taken under the hand surgical team so an allograft could also be done.
In this case, the patient had a diagnosis of CLL, Rai stage 1 and was under 6 monthly surveillance. Her initial neurological symptoms of paraesthesia in the right hand started one year after her diagnosis of CLL. However, investigations for her progressively worsening peripheral neuropathy were 20 months after diagnosis of CLL. The initiation of chemotherapy shows positive recovery of neurological symptoms in previous case reports [3]. The patient had no negative haematological predictive factors, thus not requiring treatment. However, the rare complication of nerve infiltration challenges this notion and suggests these rare complications should be screened at diagnosis and during surveillance to initiate prompt treatment and avoid progression of disease.
Conclusion
Neuroleukemiosis is a rare complication of CLL. Clinicians should consider this diagnosis in patients with a new diagnosis of leukaemia or history of leukaemia who present with peripheral nerve damage suggestive of multiple mononeuropathy. Early recognition, diagnosis and treatment of this rare complication may reduce progression of neurological deficits. Nerve biopsy is invaluable in the accurate diagnosis of neuroleukemiosis and should be considered when clinical suspicion is high.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Aregawi DG, Sherman JH, Douvas MG. et al. Neuroleukemiosis: case report of leukemic nerve infiltration in acute lymphoblastic leukemia. Muscle Nerve 2008;38:1196–200. 10.1002/mus.2108918642385 · doi ↗ · pubmed ↗
- 2Hallek M, Cheson BD, Catovsky D. et al. iw CLL guidelines for diagnosis, indications for treatment, response assessment, and supportive management of CLL. Blood 2018;131:2745–60. 10.1182/blood-2017-09-80639829540348 · doi ↗ · pubmed ↗
- 3Vicino A, Cochet S, Pistocchi S. et al. A severe case of neuroleukemiosis caused by B cell chronic lymphocytic leukemia, presenting as mononeuritis multiplex. J Peripher Nerv Syst 2023;28:266–8. 10.1111/jns.1255237119473 · doi ↗ · pubmed ↗
- 4Grisold W, Jellinger K, Lutz D. Human neurolymphomatosis in a patient with chronic lymphatic leukemia. Clin Neuropathol 1990;9:224–30.2272142 · pubmed ↗
- 5Reddy CG, Mauermann ML, Solomon BM. et al. Neuroleukemiosis: an unusual cause of peripheral neuropathy. Leuk Lymphoma 2012;53:2405–11. 10.3109/10428194.2012.69148022571477 · doi ↗ · pubmed ↗
- 6Sommer C, Carroll AS, Koike H. et al. Nerve biopsy in acquired neuropathies. J Peripher Nerv Syst 2021;26:S 21–41. 10.1111/jns.1246434523188 · doi ↗ · pubmed ↗
- 7Briani C, Visentin A, Cavallaro T. et al. Primary neurolymphomatosis as clinical onset of chronic lymphocytic leukemia. Ann Hematol 2017;96:159–61. 10.1007/s 00277-016-2852-227761605 · doi ↗ · pubmed ↗
- 8van den Bent MJ, de Bruin HG, Bos GM. et al. Negative sural nerve biopsy in neurolymphomatosis. J Neurol 1999;246:1159–63. 10.1007/s 00415005053510653308 · doi ↗ · pubmed ↗