Safety and efficacy of aneurysms treated with endovascular devices (The SEATED Study)
Ahmed R Bassiouny, Anand Sastry, Alex Mortimer, Jeremy Lynch, Hemant Sonwalkar, Aaron Bleakley, Ahmed Iqbal, Ana Paula Narata, Tufail Patankar, Islim Fathallah, Naga Kandasamy, Parthiban Balasundaram, Sara Sciacca, Juveria Siddiqui, Thomas C Booth, Yaman Adi, Yaman Adi

TL;DR
This study aims to collect nationwide data on aneurysm treatments using endovascular devices to assess their safety and effectiveness in real-world settings.
Contribution
The study introduces a nationwide consortium to pool data on less commonly used endovascular devices, enabling pragmatic real-world analysis.
Findings
Centres using the same device showed variation in antiplatelet and follow-up protocols.
The study highlights the feasibility of a nationwide consortium to analyze data on recent endovascular devices.
Initial recruitment is expected to include around 5000 patients for comprehensive analysis.
Abstract
To create a nationwide consortium to gather all the data related to advanced devices used for aneurysm treatment and conduct pragmatic real-world studies despite the variations among all centres. The strength of this study will be in pooling data of the less commonly used recent devices where there is less evidence. The study will be prospective and retrospective where the initial recruitment figure is expected to be around 5000 patients. To assess how endovascular techniques vary among different UK centres, we illustrate the results of initial surveys that were sent to those centres across the United Kingdom using a single device, the pipeline embolization device with vantage technology (PEDV). Although the centres were using the same device, the antiplatelet protocol varied from one centre to another as well as follow-up protocols according to the local experience, patient clinical…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1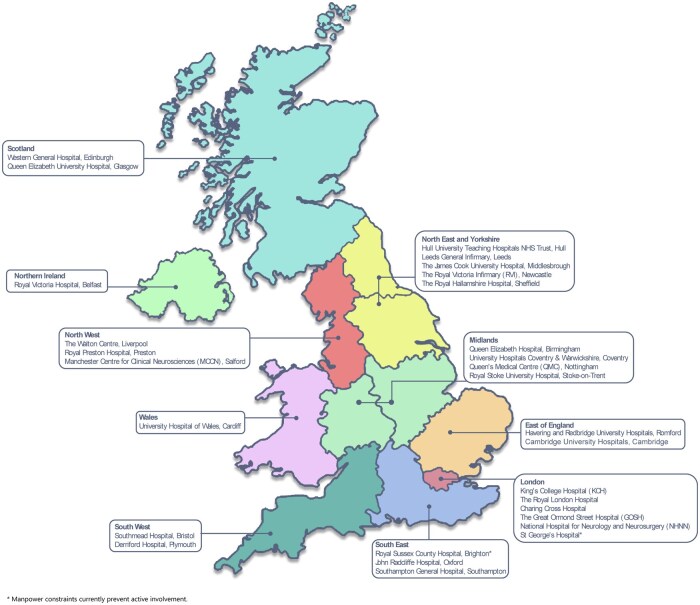 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIntracranial Aneurysms: Treatment and Complications · Cerebrovascular and Carotid Artery Diseases · Traumatic Brain Injury and Neurovascular Disturbances
Ruptured cerebral aneurysms (CAs) account for 85% of non-traumatic subarachnoid haemorrhage (aneurysmal SAH or aSAH). aSAH can be life threatening (with high mortality rate of 44%) and potentially disabling for the surviving groups.1 Aneurysms can also go unnoticed, discovered only incidentally on imaging for different indications given that unruptured aneurysms (UAs) are common with a prevalence of 3.2%. Aneurysms tend to occur more frequently and have a higher risk of rupture in females, smokers, older age groups, alcohol and cocaine abuse, those with uncontrolled hypertension and certain genetic medical conditions.2 Aneurysms that are larger than 10 mm, located in the posterior circulation, arising from the anterior communicating arterey (ACOM) or the posterior communicating artery (PCOM), or have a daughter sac are more likely to rupture.3
Management of aneurysms consists of conservative management or treatment. Treatment is either craniotomy and clipping, or endovascular treatment.4
The mainstay of endovascular treatment of aneurysms for over two decades has been coiling which has been used to treat both ruptured and UAs.5^,^6 However, coils may not be suitable for every aneurysm. For example, wide neck aneurysms can carry the risk of prolapse of coils into the parent vessel which might cause thrombus and ischaemic stroke. These led to the development of balloon-assisted coiling (BAC) as well as stent-assisted coiling (SAC).7^,^8 Recently developed devices also include intrasaccular devices, which are inserted inside the aneurysm sac, for example, the Woven EndoBridge (WEB) device (Microvention, Aliso Viejo, California, USA)9 and Contour neurovascular system (Stryker Neurovascular, Kalamazoo, Michigan, USA).10 High mesh-density stents have also been developed as a standalone treatment for aneurysms.11 Flow diverters are the name given to these groups of stents that are designed to divert blood flow away from the aneurysm. There are several different flow diverters available, including the pipeline embolization device (PED) (Medtronic, Minneapolis, Minnesota, USA), Surpass (Stryker Neurovascular, Kalamazoo, Michigan, USA), Flow Redirection Endoluminal Device (FRED) (MicroVention, Tustin, California, USA), SILK (Balt, Montmorency, France), and p64 (Phenox GmbH, Bochum, Germany).12
There is limited high-level evidence regarding the safety and efficacy of devices. For example, the pivotal international subarachnoid aneurysm trial (ISAT) randomized controlled trial (RCT) comparing safety outcomes after clipping or coiling of ruptured aneurysms, and using Guglielmi detachable coils (GDC),5 is now more than 2 decades old and coils, devices, delivery systems, and fluoroscopic equipment have all improved substantially since then. The RCT needed to replicate ISAT for UAs failed to recruit to target. In the decade following ISAT, other RCTs of UA efficacy have been largely limited to endovascular comparisons without including clipping as a comparator. In the last decade, the era of world-leading UK RCTs has receded. Instead, the vast majority of aneurysm treatment studies are not RCTs and are single-arm prospective or retrospective studies from across the world (e.g., stent-coil, flow diverters, intrasaccular). There are a variety of reasons why RCTs have become less common. One reason may be that practitioners are reluctant to randomize, another may be that government funding bodies do not want to fund studies that they think can be funded by industry, and another may be the considerable logistic barriers and costs required to run an RCT, thereby putting it beyond the reach of many funding schemes. Furthermore, industry has led many single-arm studies which are cheaper to run than RCTs and appear to be providing sufficient evidence to allow their devices to be used in current practice.
While high-level evidence is incontrovertibly needed, there is an opportunity for lower-level evidence to be obtained in pragmatic multicentre observational studies at a national level (Box 1). An example is the understanding of outcomes in real-world settings when devices are used outside of limited inclusion criteria from initial studies (Box 2). For example, devices may initially be marketed or approved for certain indications, for example, PED and Food and Drug Administration (FDA) approval for limited cerebral anatomy in USA13; or WEB marketed for bifurcations worldwide. Pooling data from these scenarios of extended use contributes to improvements in safety and efficacy in the field of interventional neuroradiology (INR), especially for devices that are used less commonly and have no or little evidence for extended use.
Data mining is the process of discovering patterns, trends, and useful insights from large datasets using statistical, machine learning, and computational techniques. Another opportunity for multicentre observational studies at a national level is therefore to mine data surrounding the determinants contributing to safety and efficacy, for example, the predictors of aneurysm occlusion, alternatively described as risk factors for failure of occlusion. Failure of aneurysm occlusion manifests as recurrence which can be seen on follow-up imaging. Risk factors related to aneurysm recurrences might vary according to the device used and technical factors related to each device (e.g., using a different sized device), or aneurysm factors (e.g., site and size of the aneurysm) or clinical factors (e.g., blood pressure control). If the risk factors are fully understood, it would help reduce recurrences through a modification of risk factors. However, many of these factors are poorly understood particularly for more recent devices. Understanding is compounded by those predictor studies that do attempt to understand risk factors, having methodological limitations. For example, predictor studies analysing the WEB device may be single centre,14^,^15 or assessed using short-term (6 months) follow-up.16^,^17 Indeed, this is on the background of there being multiple large WEB studies without a single study being a published RCT. In summary, the opportunity for multicentre pragmatic observational studies of all endovascular devices at a national level will not only contribute to safety and efficacy, especially for devices used less commonly or in extended use, but also will allow determinants of safety and efficacy (e.g., predictors of occlusion etc.) to be better understood. To achieve these broad aims, the Safety and Efficacy of Aneurysms Treated with Endovascular Devices (SEATED) study (HRA IRAS 287395 REC 25/WA/0008) will run initially over a 10-year period allowing all UK centres to perform analyses prospectively and retrospectively in up to 5000 aneurysm cases. The study gathers a wide range of real-world data on both an intention-to-treat and per protocol basis, including patient demographics and aneurysm risk factors, aneurysm characteristics, treatment details including device type and antiplatelet protocols, follow-up imaging outcomes, and clinical follow-up outcomes including complications. The UK INR community are encouraged to develop sub-studies which investigate a particular device. Once a protocol has been established, including inclusion and exclusion criteria, all sites can respond to an expression of interest. Local site Principal Investigators and the central Chief Investigator will share data among themselves (within the limits of the approved over-arching protocol) to deliver the research outcomes.
Success in achieving these broad aims through SEATED is possible because endovascular treatment of aneurysms generates a rich resource of imaging data during follow-up. This is in contrast to many UK non-radiological surgical specialties including neurosurgery where there is often limited follow-up. While it is acknowledged that there is little evidence as to whether extensive imaging follow-up is effective in terms of reducing morbidity and mortality, an important sequela is that interventional neuroradiologists typically have contact with patients for around 4 years after treatment which allows for some limited clinical contact and some limited clinical outcome (safety) data.
A recent UK multicentre observational pragmatic study which was the catalyst for SEATED was a safety and efficacy outcome study of the pipeline embolization device with vantage technology (PEDV) and involved a third of UK sites. Not only was safety and efficacy quantified in a pragmatic setting, but additional real-world insights were inevitably seen for the first time that will influence UK practice.18 For example, PEDVU(R) showed that short-term imaging follow-up for UAs using PEDV was performed using DSA in 12.6%, MRA in 84.7%, and CTA in 8%, or a combination of these modalities. The pooled data showed that MRA was considered suitable for the estimation of accurate occlusion rates alongside DSA, but not considered accurate for estimating in-stent stenosis due to susceptibility artifact from the metallic components of the device.18 Yet in older studies analysing previous generation PEDs, there had been only limited susceptibility due to different metals used in the device and so MRA was a suitable follow-up modality. These findings show that pooled real-world data are different to data from initial industry-sponsored single (or multi) centre studies where new devices are assessed with intra-arterial (IA) DSA (which is considered by some to be the reference standard for aneurysm follow-up). PEDVU(R) also showed that an effective real-word solution to overcoming the limitations of MRA was to use intravenous (IV) DSA which is less invasive than IA DSA.
We also show additional data to that published in PEDVU(R) demonstrating how UK practice has developed following initial industry-sponsored studies with limited protocols (Table 1). The results show that although the centres were using the same device, the antiplatelet protocol varied from one centre to another. It can also be seen that follow-up protocols varied from one centre to another, and in some centres, this was guided by the adjuncts uses (e.g., adjunctive coiling).
DSA: Digital Subtraction Angiography, MRA: Magnetic Resonance Angiography, TOF: Time-of-Flight, CEMRA: Contrast Enhanced Magnetic Resonance Angiography, CTA: Computerized Tomographic Angiography
We can conclude that real-world data are heterogenous and understanding this is another advantage of SEATED. Objectives include gathering the heterogenous data obtained from various INR practices across the United Kingdom, process and clean these data, and provide results that will play an important role in improving the INR practice (Figure 1). There are multiple research questions where SEATED might contribute and lead to a better understanding of INR practice, including how variability in antiplatelet and follow-up protocols influence aneurysm occlusion rates, and whether there are there significant differences in outcomes between newer and older endovascular devices.
SEATED will be prospective and retrospective (like PEDVU(R)), and while the initial recruitment figure is expected to be around 5000 patients, this figure is expected to increase by the end of the recruitment period. The participating centres are illustrated in Figure 2. Two other UK centres have joined provisionally, but currently do not have the capacity to contribute data. Therefore, 93.1% 27/29 UK centres are included representing the majority of UK practice and allowing comprehensive data collection.
We reiterate that high-level evidence is incontrovertibly needed in addition to SEATED. SEATED is not a replacement for that. However, given that all UK centres are participating in SEATED, with many practitioners contributing to rigorous analysis of practice within their departments, we are already seeing that the network is becoming more receptive to participating in, and leading, high-level evidence studies including RCTs. We also take this opportunity to advocate that the UK neurosurgical community and the INR community must not be reluctant to randomize patients based on weak evidence, or worse still, disincentivized by potential scientific results which would not support their practice. We also advocate that government funding bodies must fund RCTs acknowledging that invariably they are expensive but are the most effective mechanism to be free of bias. Finally, we advocate that industry must fund RCTs as opposed to single-arm studies wherever this is affordable, or where not affordable, support RCTs.
In summary, we are creating a nationwide network to collect data regarding advanced devices for aneurysm treatments to facilitate analysis of safety and efficacy (as primary objectives) and assess factors affecting predictors of safety and efficacy such as aneurysm recurrence after treatment (as a secondary objective). Another secondary objective is far reaching and include determining the best imaging modality for follow-up of particular devices. One particular strength of this study will be in obtaining data for the less commonly used advanced devices where there is less global evidence. Our HRA/REC approved study will run for a decade and allow UK practice to be analysed in depth and ultimately improve patients’ outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Din M , Agarwal S, Grzeda M, et al Detection of cerebral aneurysms using artificial intelligence: a systematic review and meta-analysis. J Neurointerv Surg. 2023;15:262-271.36375834 10.1136/jnis-2022-019456 PMC 9985742 · doi ↗ · pubmed ↗
- 2Vlak MH , Algra A, Brandenburg R, Rinkel GJ. Prevalence of unruptured intracranial aneurysms, with emphasis on sex, age, comorbidity, country, and time period: a systematic review and meta-analysis. Lancet Neurol. 2011;10:626-636.21641282 10.1016/S 1474-4422(11)70109-0 · doi ↗ · pubmed ↗
- 3Cebral JR , Raschi M. Suggested connections between risk factors of intracranial aneurysms: a review. Ann Biomed Eng. 2013;41:1366-1383.23242844 10.1007/s 10439-012-0723-0PMC 3628920 · doi ↗ · pubmed ↗
- 4Ajiboye N , Chalouhi N, Starke RM, Zanaty M, Bell R. Unruptured cerebral aneurysms: evaluation and management. Sci World J. 2015;2015:1–10.10.1155/2015/954954 PMC 447140126146657 · doi ↗ · pubmed ↗
- 5Molyneux AJ , Kerr RSC, Yu L-M, et al; International Subarachnoid Aneurysm Trial (ISAT) Collaborative Group. International subarachnoid aneurysm trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 patients with ruptured intracranial aneurysms: a randomised comparison of effects on survival, dependency, seizures, rebleeding, subgroups, and aneurysm occlusion. Lancet. 2005;366:809-817.16139655 10.1016/S 0140-6736(05)67214-5 · doi ↗ · pubmed ↗
- 6Coley S , Sneade M, Clarke A, et al Cerecyte coil trial: procedural safety and clinical outcomes in patients with ruptured and unruptured intracranial aneurysms. AJNR Am J Neuroradiol. 2012;33:474-480.22207299 10.3174/ajnr.A 2836 PMC 7966418 · doi ↗ · pubmed ↗
- 7Chalouhi N , Starke RM, Koltz MT, et al Stent-assisted coiling versus balloon remodeling of wide-neck aneurysms: comparison of angiographic outcomes. AJNR Am J Neuroradiol. 2013;34:1987-1992.23639562 10.3174/ajnr.A 3538 PMC 7965428 · doi ↗ · pubmed ↗
- 8Adamou A , Alexandrou M, Roth C, Chatziioannou A, Papanagiotou P. Endovascular treatment of intracranial aneurysms. Life. 2021;11:335.33920264 10.3390/life 11040335 PMC 8070180 · doi ↗ · pubmed ↗