Effective Management of Familial Erythrokeratoderma Using Topical Calcipotriol
Tamilmalar Kulandaivelavan, Manu Vidhya Harikumar, Leena Dennis Joseph, Adikrishnan Swaminathan

TL;DR
This paper reports two cases of a rare skin condition where topical calcipotriol effectively treated symptoms without additional medications.
Contribution
The novelty lies in demonstrating calcipotriol monotherapy as an effective treatment for familial erythrokeratoderma.
Findings
Topical calcipotriol resolved skin lesions in two PSEK patients.
Recurrences responded well to calcipotriol without needing corticosteroids or oral drugs.
Abstract
Progressive symmetrical erythrokeratoderma (PSEK) is a rare genodermatosis that is inherited in an autosomal dominant pattern. It is clinically characterized by the insidious onset of well-defined, non-migratory, erythematous, hyperkeratotic plaques in a symmetrical distribution over the extremities. Hereby, we describe two cases of PSEK in a father and daughter, who presented with bilaterally symmetrical hyperpigmented scaly plaques, with skin biopsy findings suggestive of erythrokeratoderma. The skin lesions resolved with topical calcipotriol monotherapy, without the use of topical corticosteroids or oral medications. During telephonic follow-up, the patients reported that recurrences also responded well to topical calcipotriol, without the need for additional medication. This case report highlights the use of topical calcipotriol as a safe and effective therapeutic alternative for…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1 Figure 2
Figure 2 Figure 3
Figure 3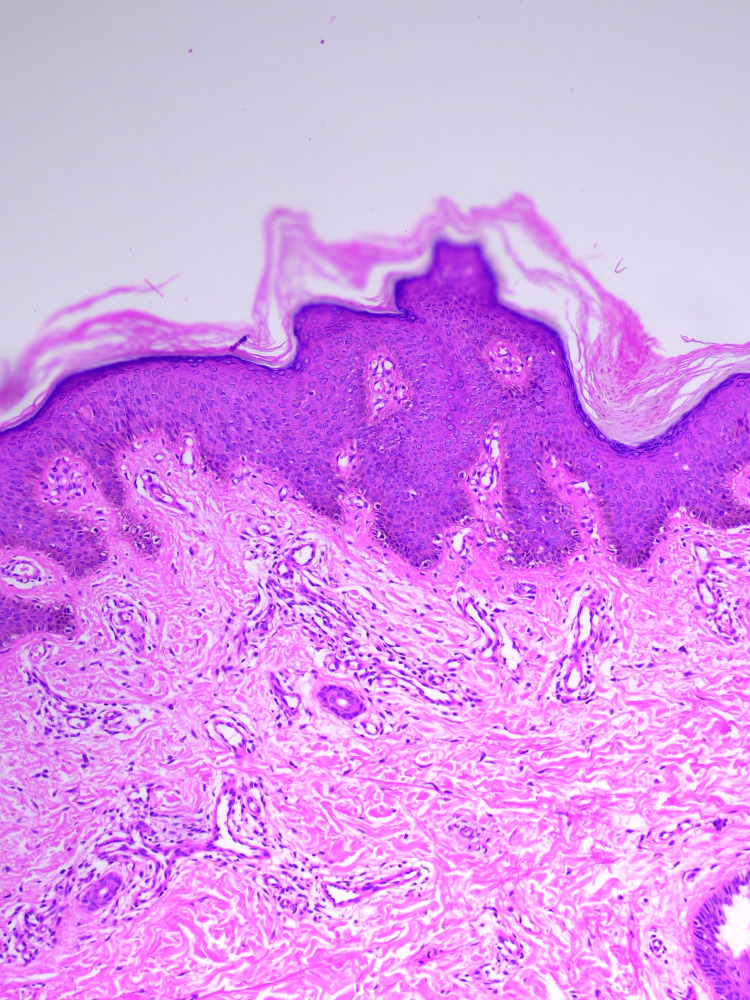 Figure 4
Figure 4 Figure 5
Figure 5 Figure 6
Figure 6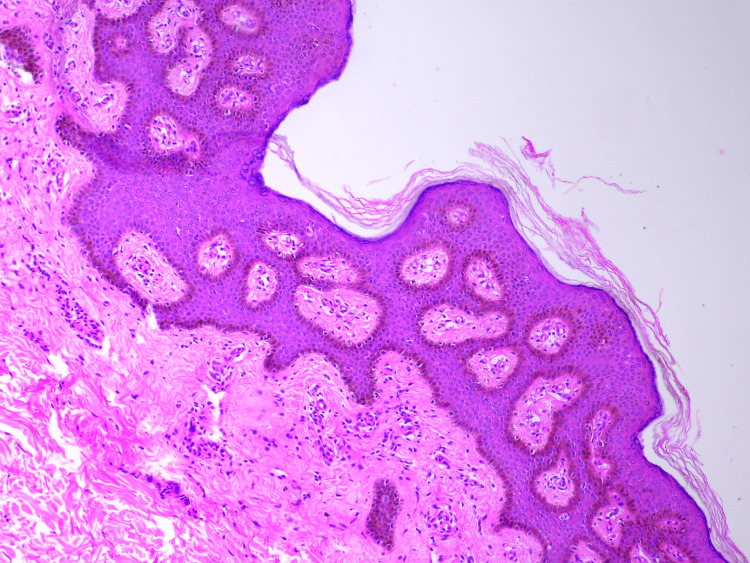 Figure 7
Figure 7Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMarine Invertebrate Physiology and Ecology · Sympathectomy and Hyperhidrosis Treatments · Dermatologic Treatments and Research
Introduction
Erythrokeratodermas are rare genodermatoses that belong to the diverse group of keratinization disorders, characterized by erythematous, hyperkeratotic plaques on the skin [1]. They have an estimated prevalence of approximately one in 2,000,000 individuals [2]. They are categorized into two non-syndromic forms: erythrokeratoderma variabilis (EKV) and progressive symmetrical erythrokeratoderma (PSEK), and two syndromic forms: keratitis ichthyosis deafness syndrome and hystrix-like ichthyosis with deafness syndrome [3]. PSEK is an uncommon autosomal dominant disease with reduced penetrance and variable expressivity [4]. To date, fewer than 100 cases have been reported worldwide [5]. Here, we report two cases of PSEK within the same family.
Case presentation
Case 1
A 13-year-old female child, the firstborn of a non-consanguineous marriage, presented with persistent, asymptomatic, dark, raised skin lesions over both underarms, forearms, and knees, with peeling of skin over feet for five years. There was a history of similar complaints in her father. Examination revealed well-defined, hyperpigmented, mildly scaly plaques in symmetrical distribution over the bilateral axilla, cubital fossa, and knees (Figures 1-2).
Well-defined hyperpigmented plaques over the bilateral cubital fossa
Hyperpigmented plaques with mild scaling over the bilateral knees
Exfoliation of skin was noted over the face and dorsum of the feet (Figure 3).
Exfoliation of the skin over the dorsum of the feet
Scalp, oral cavity, palms, soles, nails, and genitalia were normal. Based on these clinical findings, a provisional diagnosis of PSEK was made, and a skin biopsy was performed, which revealed basket-weave hyperkeratosis, focal parakeratosis, acanthosis, and prominent papillomatosis, consistent with erythrokeratoderma (Figure 4).
Histopathology image of the biopsy from the left kneeBasket weave hyperkeratosis, focal parakeratosis, acanthosis and prominent papillomatosis (hematoxylin and eosin stain, 10x)
She was started on moisturizer and topical calcipotriol and was planned for oral retinoids, but her skin lesions resolved in two months.
Case 2
A 42-year-old male, father of the above-mentioned child, second-born of a non-consanguineous marriage, presented with similar lesions over the bilateral axilla and cubital fossa since childhood (Figures 5-6).
Hyperpigmented plaque with mild scaling over the right cubital fossa
Well-defined hyperpigmented scaly plaque over the left cubital fossa
A skin biopsy revealed hyperkeratosis, acanthosis with mild papillomatosis, consistent with erythrokeratoderma (Figure 7).
Histopathology image of the biopsy from the right armHyperkeratosis, acanthosis with mild papillomatosis (hematoxylin and eosin stain, 10x)
He was also diagnosed with PSEK and was started on topical calcipotriol. Although oral retinoids were considered, he showed a good clinical response to topical calcipotriol alone.
Discussion
PSEK, otherwise known as Gottron syndrome or Darier-Gottron syndrome, was initially described by Darier in 1911 and subsequently named by Gottron in 1923 [1]. It is generally an autosomal dominant genodermatosis caused by negative mutations in the GJB4 gene, which encodes connexin 30.3. A homozygous loss-of-function mutation of KRT83 has been encountered in its recessive form [6]. Studies have demonstrated that a mutation in the loricrin gene, located on chromosome 1q21.3, results in the accumulation of abnormal loricrin in the nucleus, thereby perturbing the normal process of keratinocyte apoptosis and contributing to the pathological thickening of the stratum corneum. Sporadic cases account for approximately 50 percent of the total diagnosed patients. In this case, the condition appears to follow an autosomal dominant pattern of inheritance. Research indicates that high mitotic activity is observed in the affected skin [1]. There is no gender predilection for this disease [4].
The skin is not affected at birth. The disease presents in infancy with large, fixed, erythematous, fine, scaly plaques in a symmetrical distribution, most commonly over the cheeks, shoulders, elbows, knees, dorsum of the hands and feet, and gluteal region, associated with mild pruritus [6,7]. Lesions increase in size and number with time and become stable after puberty. Palmoplantar keratoderma is observed in approximately 50 percent of patients [1]. Unlike EKV, which is characterized by migratory lesions that may be provoked by mechanical pressure and shows seasonal exacerbations, PSEK tends to present with symmetrical, fixed lesions and shows a higher prevalence of facial involvement and palmoplantar keratoderma [3,7]. Macfarlane et al. have described two sisters from the same family with erythrokeratoderma, where the younger sister had EKV and the elder one had PSEK, implying that they may be diverse presentations of a spectrum of disorders [8].
Existing literature shows an association of PSEK with high-arched palate, fissured tongue, pectus excavatum, symmetric syndactylism, keratosis pilaris, delayed intellectual milestones, ataxia, convulsions, narcolepsy, bilateral cortical cataract, deafness, peripheral neuropathy, and nephrotic syndrome [3,9]. Still, none of these features were observed in our patients. Autosomal recessive KDSR variants have been reported in association with collodion membrane, a harlequin ichthyosis-like presentation, and thrombocytopenia, as well as progressive myelofibrosis, thereby emphasizing the clinical variability and the importance of genetic evaluation [10]. Due to financial constraints, genetic analysis was not possible in our cases.
Traditional management of erythrokeratoderma includes the use of emollients, topical retinoids, corticosteroids, and keratolytics such as salicylic acid [1,6]. Oral retinoids, primarily acitretin at a dose of 0.5 to 1 mg/kg, are considered the treatment of choice. However, recurrence is common upon discontinuation, and potential side effects, particularly in pediatric patients, must be carefully considered. Phototherapy has also been tried [1]. A review of the existing literature revealed reports of significant improvement with topical calcipotriol, which acts by inhibiting keratinocyte proliferation and promoting differentiation [4,11]. Hence, it was tried in our patients. Although oral retinoids were initially planned, both patients demonstrated significant improvement with topical calcipotriol alone; therefore, oral retinoids were not initiated. These findings suggest that topical calcipotriol is an effective and safer alternative for managing hyperkeratotic lesions in erythrokeratoderma.
Conclusions
PSEK is a chronic genodermatosis without a definitive cure. Enhancing clinical awareness is essential to prevent misdiagnosis, as early recognition can significantly improve the quality of life for patients and enable appropriate genetic counseling for affected family members. Considering the chronic and relapsing nature of the disease, topical calcipotriol may offer a safer, more cost-effective, and efficacious alternative to conventional therapies for the management of exacerbations.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Progressive symmetrical erythrokeratodermia -- case report An Bras Dermatol Guaraldi Bde M Jaime TJ Guaraldi Rde M Melo DF Nogueira OM Rodrigues N 10911288201310.1590/S 0365-05962013000100016 PMC 369994123539014 · doi ↗ · pubmed ↗
- 2Erythrokeratoderma variabilis progressiva 2024 https://www.orpha.net/en/disease/detail/308166?name=Erythrokeratoderma%20variabilis%20progressiva&mode=name
- 3Progressive symmetric erythrokeratoderma: a rare case report Indian J Paediatr Dermatol Patro N Panda M Dash M Jena SS Mohapatra M 309310172016
- 4Progressive symmetrical erythrokeratoderma - response to topical calcipotriol J Dermatol Case Rep Bilgin I BozdağKE Uysal S Ermete M 5052520112218758010.3315/jdcr.2011.1075 PMC 3184781 · doi ↗ · pubmed ↗
- 5Progressive symmetrical erythrokeratoderma Cosmo Derma Syiemlieh A Sethi JK 552025
- 6Rook's Textbook of Dermatology Hoboken (NJ) John Wiley & Sons, Ltd.2024 https://onlinelibrary.wiley.com/doi/book/10.1002/9781119709268
- 7Progressive symmetric erythrokeratoderma: report of a Chinese family Indian J Dermatol Venereol Leprol Yan HB Zhang J Liang W Zhang HY Liu JY 5976007720112186016110.4103/0378-6323.84070 · doi ↗ · pubmed ↗
- 8Is erythrokeratoderma one disorder? A clinical and ultrastructural study of two siblings Br J Dermatol Macfarlane AW Chapman SJ Verbov JL 4874911241991182817510.1111/j.1365-2133.1991.tb 00632.x · doi ↗ · pubmed ↗