Case Report: Carotid cavernous fistula presenting as red eye: case illustration and comprehensive review
Qi-Bin Xu, Wen-Yan Sheng

TL;DR
This case report highlights a rare condition causing red eye, emphasizing the importance of accurate diagnosis to avoid delays in treatment.
Contribution
The report provides a detailed case illustration and comprehensive review of carotid cavernous fistula presenting as red eye.
Findings
CCF can present with red eye and proptosis, often misdiagnosed as conjunctivitis.
Pre- and postoperative photographs help in understanding ophthalmic features of CCF.
Early diagnosis and treatment are crucial for effective management of CCF.
Abstract
Carotid cavernous fistula (CCF) is a pathological condition where an abnormal connection forms between the carotid artery and the cavernous sinus. This condition can lead to a variety of ocular and neurological symptoms, often making it difficult to diagnose, especially when patients present with common ocular complaints such as red eye, which is often misdiagnosed as conjunctivitis. The subtle and diverse symptoms of CCF can lead to misdiagnosis, delaying appropriate treatment. This article reports a case of CCF that initially presented with red eye and proptosis, leading to an ophthalmology referral. By comparing pre- and postoperative ocular photographs, the article provides a detailed review of the ophthalmic features, classification, diagnostic methods, and treatment options for CCF. The aim is to enhance clinicians’ understanding of this condition, improve diagnostic accuracy at…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
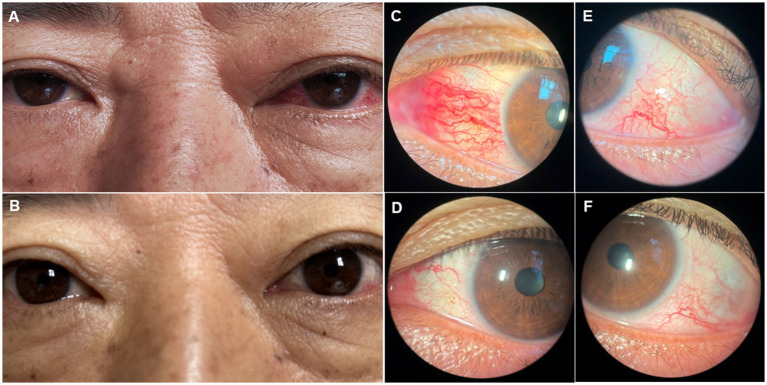 Figure 1
Figure 1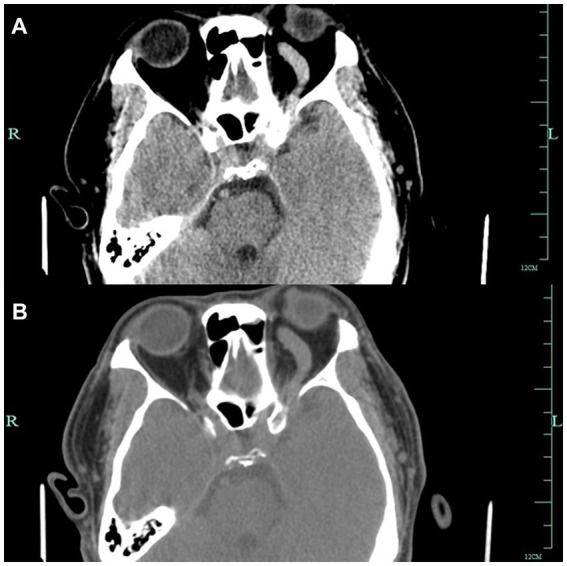 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVascular Malformations Diagnosis and Treatment · Intracranial Aneurysms: Treatment and Complications · Trigeminal Neuralgia and Treatments
Introduction
1
Carotid cavernous fistula (CCF) is a pathological condition where an abnormal connection forms between the carotid artery and the cavernous sinus. This condition can lead to a variety of ocular and neurological symptoms, often making it difficult to diagnose, especially when patients present with common ocular complaints such as red eye, which is often misdiagnosed as conjunctivitis. The subtle and diverse symptoms of CCF can lead to misdiagnosis, delaying appropriate treatment. This article reports a case of CCF that initially presented with red eye and proptosis, leading to an ophthalmology referral. By comparing pre- and postoperative ocular photographs, the article provides a detailed review of the ophthalmic features, classification, diagnostic methods, and treatment options for CCF. The aim is to enhance clinicians’ understanding of this condition, improve diagnostic accuracy at initial presentation, and promote timely and effective treatment.
Case report
2
A 52-year-old man presented to the ophthalmology department with a 3-month history of left eye redness and proptosis (Figure 1A). The patient reported no history of trauma or systemic diseases. Ophthalmic examination revealed significant tortuosity and dilation of conjunctival veins, particularly prominent in the nasal area (Figures 1C,E). Mild left eye proptosis was noted, but visual acuity and ocular motility were relatively intact. Intraocular pressure was within normal limits. Given the clinical findings, a cranial computed tomography was performed, which suggested a suspected a left carotid cavernous sinus fistula (Figures 2A,B). The patient was subsequently referred to the neurosurgery department for further management.
Figures A and B show clinical photos of the patient’s eyes before and after surgical treatment for left carotid cavernous sinus fistula. Figures C and D show the dilation and regression of the left eye nasal conjunctival blood vessels before and after surgery. Figures E and F show the dilation and regression of left temporal conjunctival blood vessels before and after surgery.
Figures A and B show Axial CT images showing left-sided proptosis with thickening of the sclera. The left optic foramen is enlarged, and the left cavernous sinus exhibits heterogeneous density. The left superior orbital vessels appear tortuous and dilated.
The patient was diagnosed with carotid cavernous sinus fistula. Subsequently, the patient underwent endovascular embolization, during which a detachable balloon was used to occlude the fistula. Post-procedure, the patient’s left eye proptosis improved significantly, and the conjunctival dilation and edema were notably alleviated (Figures 1B,D,F). Follow-up examinations at 1 month and 3 months post-treatment showed no recurrence of symptoms, and the patient remained asymptomatic.
Discussion
3
Clinical manifestations of CCF
3.1
CCF can present with a wide array of ocular symptoms, making it a diagnostic challenge. Common manifestations include conjunctival chemosis and congestion, proptosis, ocular motility impairments, and visual disturbances. In the presented case, the patient’s red eye and conjunctival vascular changes were typical early manifestations of CCF. Preechawat et al. (1) reported that a significant proportion of CCF patients present with multiple concurrent signs, such as proptosis in 84%, tortuous and dilated conjunctival veins in 93%, chemosis in 42%, cranial nerve palsy and related disorders in 52%, elevated intraocular pressure in 51%, optic neuropathy in 13%, and visual impairment in 43%. These data underscore the importance of a comprehensive ocular assessment in suspecting CCF, especially in patients with unexplained or persistent ocular symptoms.
Diagnosis of CCF
3.2
Imaging modalities
3.2.1
Imaging plays a crucial role in the diagnosis of CCF. Orbital color Doppler ultrasound is a non-invasive imaging modality that can detect dilated superior ophthalmic veins and thickened extraocular muscles. It can also observe the characteristic pulsation of the veins synchronous with the cardiac cycle, providing direct evidence of arterial blood flow into the venous system. Computed tomography (CT) and magnetic resonance imaging (MRI) are also important tools in CCF diagnosis (2), as they can reveal structural changes such as enlargement of the cavernous sinus and proptosis. However, digital subtraction angiography (DSA) remains the gold standard for CCF diagnosis. DSA can precisely localize the position, size, and vascular connections of the fistula, thereby guiding subsequent therapeutic strategies (3).
Differential diagnosis
3.2.2
The symptoms of CCF often mimic those of other ocular diseases, leading to potential misdiagnosis. Conditions such as conjunctivitis (4), thyroid eye disease, orbital inflammatory syndrome, and glaucoma can present with similar symptoms (5). Therefore, a meticulous medical history, comprehensive physical examination, and multimodal imaging analysis are essential to differentiate CCF from these conditions (6). For instance, in patients with suspected CCF, the presence of conjunctival vascular tortuosity and dilation, especially when accompanied by other ocular signs or abnormal imaging findings, should prompt further investigation for CCF.
Treatment of CCF
3.3
The treatment approach for CCF varies depending on factors such as the size and flow rate of the fistula, as well as the patient’s symptoms. Conservative management, including carotid compression or medication, may be considered for low-flow, asymptomatic fistulas to promote thrombosis and relieve symptoms (7). However, most high-flow fistulas require interventional treatment. With the advancement of endovascular techniques, embolization using coils, balloons, or liquid embolic agents has become the primary treatment modality, achieving high occlusion rates and favorable outcomes (8, 9). In some cases, surgical decompression may be necessary when complications persist after embolization.
Conclusion
4
CCF presenting with red eye can be easily overlooked or misdiagnosed, leading to delayed treatment and potential complications. Clinicians should maintain a high index of suspicion when encountering patients with unexplained ocular symptoms, especially those with persistent red eye accompanied by other ocular abnormalities. Timely utilization of appropriate imaging modalities and referral for further evaluation can significantly enhance diagnostic accuracy and ensure prompt treatment, thereby preventing potential visual impairment and neurological complications. Through this case report and comprehensive review, we aim to raise clinicians’ awareness and understanding of CCF, facilitating early and accurate diagnosis in clinical practice.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Preechawat P Narmkerd P Jiarakongmun P. Dural carotid cavernous sinus fistula: ocular characteristics, endovascular management and clinical outcome[J]. J Med Assoc Thai. (2008) 91:852–8., PMID: 18697384 · pubmed ↗
- 2Hsieh YH Weng TH Tai MC Chien KH. Amelioration of acute orbital compartment syndrome following transvenous embolization for an indirect carotid-cavernous fistula: a case report. Medicine (Baltimore). (2017) 96:e 9096. doi: 10.1097/MD.0000000000009096, PMID: 29245336 PMC 5728951 · doi ↗ · pubmed ↗
- 3Chen CC Chang PC Shy CG. CT angiography and MR angiography in the evaluation of carotid cavernous sinus fistula prior to embolization: a comparison of techniques[J]. AJNR Am J Neuroradiol. (2005) 26:2349–56. PMID: 16219844 PMC 7976166 · pubmed ↗
- 4Jacobs SM Arias EJ Derdeyn CP Couch SM Custer PL. Carotid cavernous sinus fistulas without superior ophthalmic vein enlargement. Ophthalmic Plast Reconstr Surg. (2015) 31:191–6. doi: 10.1097/IOP.0000000000000241, PMID: 25105521 · doi ↗ · pubmed ↗
- 5Agrawal M Kumari L Vichare N Shyamsundar K Avasthi A Gupta S. Carotid-cavernous fistula masquerading as thyroid associated orbitopathy: a diagnostic challenge. Rom J Ophthalmol. (2022) 66:168–72. doi: 10.22336/rjo.2022.33, PMID: 35935074 PMC 9289768 · doi ↗ · pubmed ↗
- 6Azzam DB Cypen SG Conger JR Tao JP. Carotid-cavernous sinus fistula masquerading as thyroid eye disease. Cureus. (2021) 13:e 14261. doi: 10.7759/cureus.14261, PMID: 33959444 PMC 8093110 · doi ↗ · pubmed ↗
- 7Texakalidis P Tzoumas A Xenos D Rivet DJ Reavey-Cantwell J. Carotid cavernous fistula (CCF) treatment approaches: a systematic literature review and meta-analysis of transarterial and transvenous embolization for direct and indirect CC Fs. Clin Neurol Neurosurg. (2021) 204:106601. doi: 10.1016/j.clineuro.2021.106601, PMID: 33774507 · doi ↗ · pubmed ↗
- 8Pal A Blanzy JGómez KJR Preul MC Vernon BL. Liquid embolic agents for endovascular embolization: a review. Gels. (2023) 9:378. doi: 10.3390/gels 9050378, PMID: 37232970 PMC 10217684 · doi ↗ · pubmed ↗