Retroperitoneal invasive fibromatosis after laparoscopic radical resection of colon cancer: a case report and literature review
Tiantian Shan, Yiqi Zhang, Yang Yao, Min Li, Xiaoying Li

TL;DR
A rare case of retroperitoneal invasive fibromatosis occurring after colon cancer surgery is reported and reviewed.
Contribution
This case report adds to the limited literature on postoperative retroperitoneal invasive fibromatosis in colorectal cancer patients.
Findings
A 63-year-old male developed retroperitoneal invasive fibromatosis one year after colon cancer surgery.
Diagnosis was confirmed using enhanced CT, pathological examination, and Whole Exome Sequencing.
The case highlights the need for awareness of this rare condition in postoperative colorectal cancer patients.
Abstract
Invasive fibromatosis is a rare, locally invasive, benign fibrous tumor that mainly occurs in the anterior abdominal wall and limbs, with a lower incidence in the retroperitoneum. This article reports a case of retroperitoneal invasive fibromatosis in a 63-year-old male patient. The patient underwent resection for sigmoid colon cancer and was diagnosed with retroperitoneal invasive fibromatosis through enhanced CT, pathological examination and Whole Exome Sequencing one year after surgery. Given the rarity of postoperative surgery-related retroperitoneal invasive fibromatosis in patients with colorectal cancer, this article aims to provide a reference for clinical research on retroperitoneal invasive fibromatosis by reporting this case.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
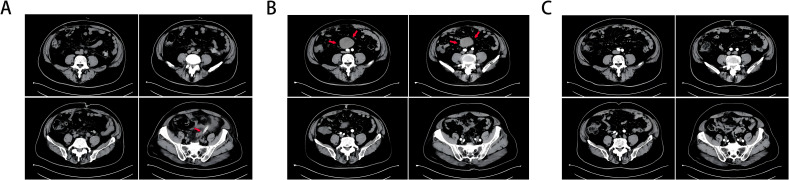 Figure 1
Figure 1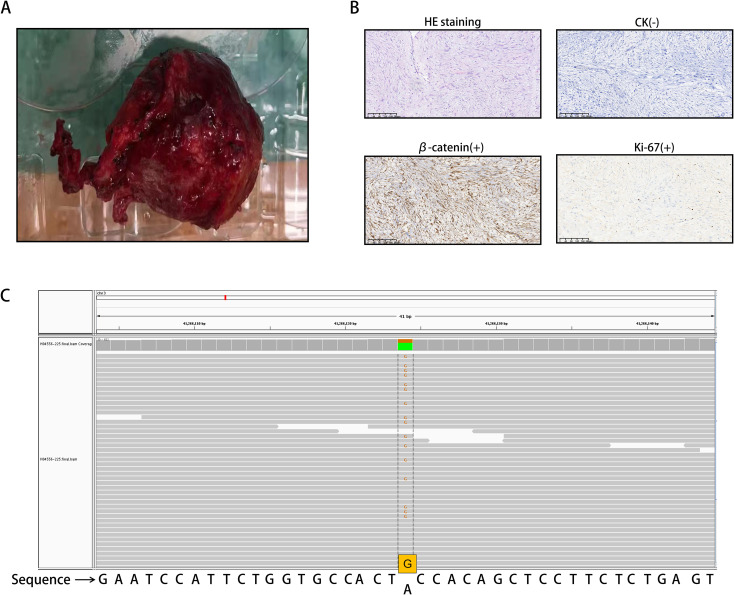 Figure 2
Figure 2| Type | Location | Treatment | Outcome | Reference |
|---|---|---|---|---|
| Extraabdominal fibromatosis | Shoulder | Surgical wide en bloc resection of the tumor | Uneventful recovery | ( |
| Pelvis | Surgical resection | Uneventful recovery | ( | |
| Chest | The modified Grunenwald method and Trap Door method; adjuvant radiation | Without recurrence at 14 months after surgery | ( | |
| Neck muscles | Function-preserving surgery followed by radiotherapy | Continuous close follow-up and no local recurrences in the past 7 years | ( | |
| Other muscle regions | En bloc excision with instrumented fusion followed by local radiotherapy | Successful treatment | ( | |
| Intraabdominal fibromatosis | Colon | Conservative therapy and physiotherapy | General improvement in signs and symptoms | ( |
| Jejunal mesentery | Exploratory laparotomy and en bloc resection of mesenteric mass, jejunum (with primary anastomosis), and antimesenteric part of 4th portion of duodenum (Heineke–Mikulicz strictureplasty) | Regular follow-up in the gastroenterology and surgery clinic | ( | |
| Ileal mesentery | Complete tumor resection | High5-year recurrence-free survival rate and careful follow-up | ( | |
| The retroperitoneal | Tumor resection, right salpingo-oophorectomy, ureterectomy, and ureterocystostomy; pharmacotherapy with tranilast | The mass disappeared | ( | |
| Abdominal wall | En bloc resection of the underlying musculature (right obliquus externus abdominis, obliquus internus abdominis, transverses abdominis, and rectus abdominis), right testis, and spermatic cord;abdominal wall defect repaired with a polypropylene mesh | Good health and shows no symptoms or imaging signs of recurrence at 20 months postoperative; physical examination revealed the swelling of the right lower extremity | ( |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSoft tissue tumor case studies · Neurofibromatosis and Schwannoma Cases · Sarcoma Diagnosis and Treatment
Introduction
Invasive fibromatosis, also known as desmoid-type fibromatosis (DF), is a rare, locally aggressive, benign fibrous tumor that originates from a mesenchymal cell line and is a subtype of mesenchymal tumor (1, 2). This tumor is a rare soft tissue sarcoma (STS), representing only 3% of all STSs and 0.03% of all tumors, with a high likelihood of recurrence without metastasis (3, 4). The local recurrence rate is high, ranging from 18% to 56% (5). DF usually occurs sporadically, but approximately 5% of cases are related to familial adenomatous polyposis (FAP); it most often occurs in the anterior abdominal wall and limbs and rarely occurs in the retroperitoneum (6, 7). The exact etiology is unclear. These tumors are rarely symptomatic, but when symptomatic, it is mainly due to the impact of the mass on the adjacent vasculature and organs. In most cases, they are found incidentally during imaging studies (7).
We report a case of a retroperitoneal invasive fibroma that was incidentally diagnosed. The patient is a 63-year-old man with a history of resection for sigmoid colon cancer who presented to the emergency department complaining of recurrent abdominal pain. In this case, we discuss the characteristics of this extremely rare tumor.
Case presentation
A 63-year-old man was found to have neoplastic polyps measuring approximately 2.21.41 cm in the sigmoid colon during routine gastrointestinal endoscopy. The polyps were removed via ESD. Pathology revealed moderately differentiated tubular adenocarcinoma with an SM invasion depth ≥ 1000 µm. The possibility of submucosal invasion was not excluded. Laparoscopic resection of colon cancer was performed at the Department of Gastroenterology, and approximately 24 cm of the sigmoid colon was removed. Pathology revealed that there was no atypical hyperplasia. Figure 1A shows the postoperative CT image.
(A) CT taken 1 day after colon cancer surgery, and an arrow marks the drainage tube. (B) A retroperitoneal tumor (marked with an arrow) was found on intensive CT 1 year after colon cancer surgery, and there was vascular nourishment in the tumor. (C) Abdominal CT 3 years after resection of colon cancer and 2 years after resection of invasive fibroids, and no obvious abnormalities were found.
Within six months postsurgery (February–August 2021), the patient developed persistent symptoms, including increased stool frequency, loose stools, and weight loss. Gastrointestinal endoscopy performed in August 2021 revealed normal gastrointestinal mucosa without tumor recurrence, polyps, or anastomotic stricture. By December 2021, the patient’s bowel habits and stool morphology had normalized. In February 2022, the patient experienced lower abdominal discomfort and mild abdominal pain. Contrast-enhanced CT (Figure 1B) revealed a retroperitoneal mass with a vascular supply, suggesting possible tumor recurrence.
Since the possibility of tumor recurrence could not be ruled out, the patient underwent laparoscopic exploration and retroperitoneal tumor resection. The tumor (Figure 2A) was excised intraoperatively and sent for histopathological analysis. Under the microscope, spindle cell tumor-like hyperplasia was observed on HE stained sections, and the boundary with the surrounding adipose tissue was unclear. The results of immunohistochemical staining revealed the following: β-catenin (+), vimentin (+), Ki-67 (2%), SMA (-), ALK (-), MDM2 (-), CDK4 (-), CD34 (-), Bcl-2 (-), STAT-6 (-), S-100 (-), SOX-10 (-), CD117 (-), DoG-1 (-), and CK (-). The HE staining and immunohistochemical results suggested that the mass was invasive fibromatosis and a borderline tumor (Figure 2B).
(A) Invasive fibroid surgery and excised tumor tissue. (B) Spindle cell neoplasia with ill-defined demarcation from surrounding adipose tissue on HE staining. The cells were sparse and dense and exhibited interstitial collagen degeneration, mucus degeneration, and high erythrocyte extravasation. The immunohistochemical staining results were as follows: Ki-67 (2%+), β-catenin (partial nucleus +), and CK (-). (C) The CTNNB1 gene mutation is located on chromosome 3, with mutation coordinates chr3:41266124 (hg19). The 121st nucleotide corresponding to exon 3 of the coding region changes from A to G (c.A121G). This was determined through the use of WES.
To confirm the diagnosis of tumor slices, whole exome sequencing (WES) was performed (Figure 2C). We found a CTNNB1 gene mutation on chromosome 3, with mutation coordinates chr3:41266124 (hg19). The 121st nucleotide corresponding to exon 3 of the coding region changes from A to G (c.A121G). This mutation is a missense mutation in all transcripts, causing the 41st amino acid of CTNNB1 encoded protein β-catenin to mutate from threonine to alanine (p.T41A). Based on the above results, the patient was diagnosed with DF.
The patient recovered uneventfully, with resolution of symptoms. During the 2-year follow-up period (March 2022–December 2024), the patient remained asymptomatic with normal bowel function, appetite, and weight restoration to preoperative levels. Serial abdominal CT scans (Figure 1C) confirmed that there was no recurrence of the retroperitoneal fibromatosis or colorectal carcinoma.
Discussion
Fibromatosis is a disease characterized by fibrous connective tissue hyperplasia and it can be divided into primary fibromatosis and invasive fibromatosis (8). Invasive fibromatosis, also known as desmoid-type fibromatosis (DF), is a type of interstitial neoplasm formed by adherent cells, fascia and aponeurosis. In terms of location, invasive fibromatosis can be divided into several groups: extraabdominal fibromatosis, which occurs in the shoulder (9), pelvis (10), chest (11) and neck muscles (12) and other muscle regions (13); intraabdominal fibromatosis, which involves the colon (14), small intestinal mesenteric connective tissue (15, 16), and retroperitoneal space (17); and fibromatosis, which can also occur in the abdominal wall (18) (Table 1). Two to six cases are newly diagnosed per million people worldwide every year, and more than 90% of DF cases are sporadic and associated with β-catenin gene (CTNNB1) mutations. A small number of DF patients are diagnosed with germline APC mutations, which present as familial adenomatous polyposis (FAP) (19). The incidence of DF in FAP patients is estimated to be 3–30% (20). However, approximately 8% of patients with sporadic DF have a family history of colon cancer, suggesting a genetic predisposition to both diseases (21).
Computed tomography (CT) and magnetic resonance imaging (MRI) are the main imaging examination methods for detecting DF (22). With respect to the underlying mechanism of DF, the constitutive activation caused by the mutation of the β-catenin oncogene CTNNB1 (in sporadic cases) (23) or the germline activation of the adenomatous polyposis coli (APC) gene (in FAP patients) (24) will activate the Wnt pathway, thus preventing the degradation of cytosolic β-catenin. Therefore, dysregulation of the Wnt pathway plays a key role in the development of a variety of DFs. Moreover, the Wnt pathway is directly related to the pathogenesis of DF, but crosstalk with the Notch signaling pathway is crucial. Notch receptors are transmembrane proteins that play key roles in cell formation, differentiation, and apoptosis (22). In FAP patients, β-catenin-mediated upregulation of jagged-1/2 (jag-1), a notch-specific ligand, has been shown to activate Notch signaling (25). Therefore, the Wnt pathway and the Notch signaling pathway can interact with each other, leading to the occurrence of DF.
The etiology and pathogenesis of retroperitoneal invasive fibromatosis are not fully understood, but it has been reported that, in addition to the activation of abnormal Wnt signaling at the molecular level, which is mediated by the APC/β-catenin pathway and the activation of the Notch signaling pathway, it is related to trauma (including previous surgery), long-term estrogen use, pregnancy or puerperium (26). Studies have revealed that when DF occurs in the retroperitoneum, it usually has a clinical background of familial polyposis coli/familial adenomatous polyposis (FAP), colon cancer or Gardner syndrome, especially when the patient has a history of abdominal surgery (4). Postoperative development of a fibroma may be mistaken for tumor recurrence, especially when the tumor appears at the previous surgical site. It can be local or regional but never metastasizes. The incidence of this type of invasive fibroma is extremely low, and its etiology is unknown (27). Studies have revealed that fibromatosis tends to exhibit local invasive growth and recurrence. The growth is not constant and may eventually subside, but it will also grow rapidly in some periods. It is generally believed that the invasive growth of these tumors is triggered during surgery, particularly during abdominal surgery (27, 28), but the specific mechanism is not clear.
Owing to the rarity of this disease, the clinical diagnosis of DF is not simple, and the misdiagnosis rate can be as high as 30% to 40% (1). On CT images, fibromas usually appear as dense soft tissue masses with clear boundaries and uniform enhancement, but in some cases, they may appear more aggressive with unclear margins (29). Histological diagnosis usually requires the exclusion of other possible mesenchymal tumors, such as gastrointestinal stromal tumors or low-grade leiomyosarcomas (30), and fibromas are characterized by monoclonal fibroblast proliferation, manifested as small bundles of spindle cells in abundant fibrous stroma with low cell density and no malignant characteristics (2). Different types of soft tissue tumors have different immunohistochemical markers, in addition to differences in imaging and histology. Distinct immunophenotypic markers aid in differentiating these tumor types. For example, aggressive fibromatosis (a fibroblastic/myofibroblastic tumor) is characterized by diffuse cytoplasmic and nuclear β-catenin positivity along with vimentin and Ki-67 expression (31). Notably, other fibroblastic tumors lack nuclear β-catenin expression.
The Ki-67 index, widely used as a proliferation marker in clinical practice, reflects tumor cell proliferative activity through its expression in the G1, S, G2, and M phases (absent in the G0 phase), with higher values indicating greater malignant potential (32, 33). SMA and desmin positivity is typically indicative of leiomyoma (34). ALK positivity typically suggests an inflammatory myofibroblastic tumor (35), whereas liposarcoma (the most common soft tissue sarcoma) frequently harbors MDM2 and CDK4 amplifications in chromosomal region 12q13–15 (36). Coexpression of CD34, Bcl-2, CD99, and STAT-6 supports the diagnosis of solitary fibrous tumor (SFT) (37), whereas peripheral nerve sheath tumors are positive for S-100 and SOX-10 (38). Gastrointestinal stromal tumors (GISTs) typically express CD117 and DoG-1 (39). Carcinosarcoma, a biphasic malignancy containing both epithelial and mesenchymal components, is characterized by concurrent CK and vimentin expression (40).
In this case, MRI examination was declined by the patient. We comprehensively summarize the following immunohistochemical profile of this case: β-catenin (+), vimentin (+), Ki-67 (2%), SMA (-), ALK (-), MDM2 (-), CDK4 (-), CD34 (-), Bcl-2 (-), STAT-6 (-), S-100 (-), SOX-10 (-), CD117 (-), DoG-1 (-), and CK (-). This immunoprofile strongly supports the diagnosis of aggressive fibromatosis.
Every year, there are 2 to 6 newly diagnosed cases per million people worldwide, with over 90% of DF cases being sporadic and related to mutations in the β-catenin gene (CTNNB1). To demonstrate the relationship between tumor occurrence and gene mutations, tumor slices were sent for testing and subjected to WES. These results were interpreted based on the 2015 Gene Sequence Interpretation Guidelines and genome coordinates published by the American Society for Medical Genetics and Genomics (ACMG). We have detected a mutation in the CTNNB1 gene, which is located on chromosome 3 at 3p22.1. The coordinates of the gene mutation are located at chr3:41266124 (hg19), and the nucleotide at position 121 of the gene coding region has changed from A to G (c.A121G). Affects four transcripts, namely NM_001098209, NM_001098210, NM_001904, and NM_001330729. This mutation is a missense mutation in all transcripts, causing the 41st amino acid of the CTNNB1 encoded protein β-catenin to change from threonine to alanine (p.T41A), disrupting the GSK3 β phosphorylation site (a key site in the degradation signaling pathway), preventing the normal degradation of β-catenin, leading to abnormal protein accumulation and sustained activation of the Wnt signaling pathway, promoting cell proliferation, and ultimately leading to cancer. According to the ACMG classification, this mutation is defined as PP5 (pathogenicity, ClinVAR database) and PM2 (extremely low population frequency, consistent with carcinogenic mutation characteristics). Therefore, we believe that this disease can enrich our understanding of this type of tumor.
This type of tumor is difficult to treat, and many factors, such as age, tumor location and size, affect the prognosis. Among the many types of DFs, abdominal wall DFs have the best prognosis, followed by intra-abdominal DFs and limb DFs, which are known to have a greater risk of progression. Retroperitoneal invasive fibromas can be divided into three categories: asymptomatic resectable tumors, symptomatic resectable tumors, and unresectable and recurrent tumors. For asymptomatic patients, a “watch and wait” approach may be the most appropriate treatment, as such an approach can avoid unnecessary morbidity caused by surgery or radiotherapy. Surgical resection may be required to prevent disease progression, suggesting that a personalized, multidisciplinary approach to treatment is needed (22). For symptomatic retroperitoneal fibromas, their sensitivity to chemotherapy and radiotherapy is limited, and surgery is still the only curative treatment; however, studies have revealed that incomplete resection of DFs is associated with postoperative progression (41).
In the third category of unresectable and recurrent tumors, treatment options include antihormone therapy, NSAIDs, tyrosine kinase inhibitors, cytotoxic chemotherapy, radiotherapy, and close observation (42). Regardless of the type, this type of fibroma grows slowly, and patients often recover well. Although the prognosis of invasive fibromas after treatment is good, there is no reliable measure for preventing the development of an invasive fibroma after abdominal surgery.
In this case, the patient had a history of colon cancer and abdominal surgery. The invasive fibroma developed within a very short time after surgery. β-catenin showed characteristic nuclear positivity. Meanwhile, the WES results showed a mutation in the CTNNB1 gene. After laparoscopic resection, the patient recovered well without any symptoms or discomfort after the operation. Moreover, we followed the patient, and 2 years later, abdominal computed tomography (CT) revealed no recurrence of the retroperitoneal tumor or the colon cancer. The patient had returned to his preoperative weight.
Conclusion
Since invasive fibromas in the retroperitoneum are rare, it is essential to report any cases encountered. In this study, we present follow-up data for a patient who developed an invasive fibroma after colon cancer resection surgery. The CT image of the patient showed fibroma formation, with characteristic nuclear positivity of β-catenin immunohistochemistry. At the same time, WES results confirmed a mutation in the CTNNB1 gene. Retroperitoneal invasive fibromatosis is a medium-sized soft tissue tumor characterized by monoclonal fibroblast proliferation, and its clinical course is variable and unpredictable. However, few clinical trials have focused on such patients, and most studies are case series with relatively small numbers of patients. Therefore, more research on such tumors is needed.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Shen C Wang C Yan J He T Zhou X Ma W . Clinicopathological characteristics, treatment, and survival outcomes of retroperitoneal desmoid-type fibromatosis: A single-institution experience in China. Med (Baltimore). (2019) 98:e 18081. doi: 10.1097/MD.0000000000018081, PMID: 31764841 PMC 6882633 · doi ↗ · pubmed ↗
- 2Aidid F Aichouni N Afilal I Abbou W Jabi R Miry N . Retroperitoneal desmoid tumor in a patient with familial adenomatous polyposis: A case report. Radiol Case Rep. (2022) 17:2910–4. doi: 10.1016/j.radcr.2022.05.013, PMID: 35755096 PMC 9218292 · doi ↗ · pubmed ↗
- 3Meazza C Bisogno G Gronchi A Fiore M Cecchetto G Alaggio R . Aggressive fibromatosis in children and adolescents: the Italian experience. Cancer. (2010) 116:233–40. doi: 10.1002/cncr.24679, PMID: 19950127 · doi ↗ · pubmed ↗
- 4Mishra DP Rout SS . Desmoid tumors: A clear perspective or a persisting enigma? A case report and review of literature. World J Oncol. (2016) 7:21–7. doi: 10.14740/wjon 961w, PMID: 28983359 PMC 5624685 · doi ↗ · pubmed ↗
- 5Peng PD Hyder O Mavros MN Turley R Groeschl R Firoozmand A . Management and recurrence patterns of desmoids tumors: a multi-institutional analysis of 211 patients. Ann Surg Oncol. (2012) 19:4036–42. doi: 10.1245/s 10434-012-2634-6, PMID: 22972507 PMC 3568525 · doi ↗ · pubmed ↗
- 6Keusch CF Bauer J . Mesenteric fibromatosis in Gardner’s syndrome. Mt Sinai J Med. (1989) 56:318–20., PMID: 2677697 · pubmed ↗
- 7El Charif MH Tarhini H Dushfunian D Al Harake H Khasawneh H Abi Saad G . Retroperitoneal desmoid-type fibromatosis: a case report. Ann Med Surg (Lond). (2023) 85:1258–61. doi: 10.1097/MS 9.0000000000000491, PMID: 37113969 PMC 10129236 · doi ↗ · pubmed ↗
- 8Ferenc T Sygut J Kopczyński J Mayer M Latos-Bieleńska A Dziki A . Aggressive fibromatosis (desmoid tumors): definition, occurrence, pathology, diagnostic problems, clinical behavior, genetic background. Pol J Pathol. (2006) 57:5–15., PMID: 16739877 · pubmed ↗