Male breast cancer following complete remission of acute myeloid leukemia: A case report and literature review
Weiqiang Qiao, Peng Li, Chang Chang, Mengnan Fan, Miao Deng

TL;DR
A 51-year-old man developed male breast cancer after being in remission from acute myeloid leukemia, offering new insights into rare cancer cases.
Contribution
This is the first documented case of male breast cancer following complete remission of acute myeloid leukemia.
Findings
The patient achieved favorable outcomes with neoadjuvant chemotherapy, surgery, radiotherapy, and endocrine therapy.
The case suggests a potential link between prior chemotherapy for AML and somatic gene mutations leading to breast cancer.
This case highlights the need for long-term monitoring of cancer survivors for secondary malignancies.
Abstract
Male breast cancer (MBC) is a rare clinical entity. The concurrent development of MBC and leukemia is particularly rare. A 51-year-old male patient developed MBC following a 1-year complete remission of acute myeloid leukemia (AML). The patient underwent neoadjuvant chemotherapy, followed by surgical resection and adjuvant radiotherapy, and is currently receiving endocrine therapy with tamoxifen (10 mg twice daily, orally), with favorable outcomes observed during recent follow-up evaluations. MBC is predominantly diagnosed as locally advanced disease. Reported cases include MBC following acute lymphoblastic leukemia (ALL) and therapy-related AML post-chemotherapy for female breast cancer, whereas our case exhibits novel distinctions compared to prior reports. This case report describes the first documented occurrence of MBC in a patient who achieved complete remission from AML,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
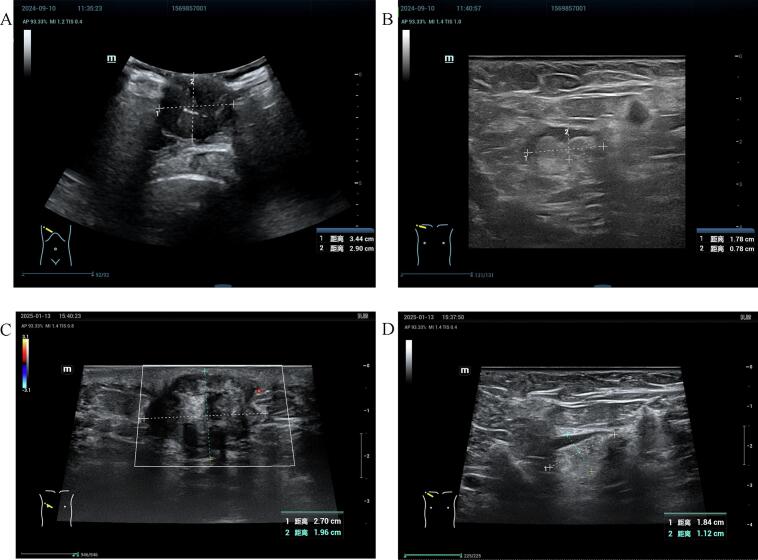 Figure 1
Figure 1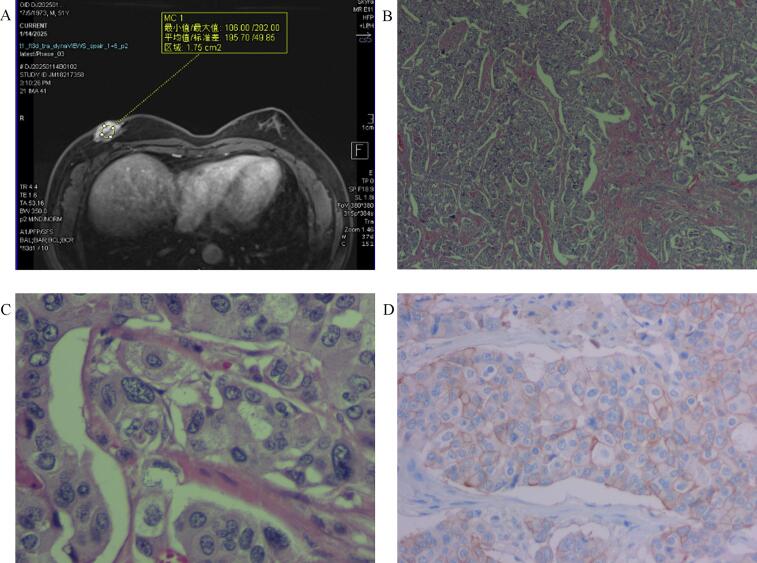 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMale Breast Health Studies · Cancer and Skin Lesions · BRCA gene mutations in cancer
Introduction
1
Male breast cancer (MBC) represents a rare clinical entity, accounting for less than 1 % of all breast cancer cases [1]. The concurrent development of MBC and leukemia is particularly rare, with existing evidence predominantly documented in case reports [2,3]. Here, we report a case of MBC emerging post-complete remission in an acute myeloid leukemia (AML) patient. This case report has been reported in line with the SCARE checklist [4].
Case presentation
2
In February 2006, a 33-year-old male patient was diagnosed with AML in the Department of Oncology. Prior to the diagnosis of AML, the patient was in good health with no significant abnormalities detected during routine physical examinations. There was no notable family history of malignant tumors or hematologic disorders. The patient was diagnosed with AML with increased granules, classified as the M3 subtype (AML-M3a) according to the French-American-British (FAB) classification system. The patient achieved remission following induction chemotherapy with a arsenic trioxide and retinoid regimen. From 2006 to 2010, the patient underwent sequential chemotherapy regimens (daunorubicin and cytarabine, mitoxantrone and cytarabine, homoharringtonine and cytarabine, pirarubicin and cytarabine, etoposide and cytarabine), which resulted in sustained complete remission.
In September 2024, the patient was admitted to the Department of Oncology with a primary complaint of a right breast mass, which had been present for three years. Breast ultrasound identified a subareolar mass (34 mm maximal diameter) with ill-defined margins and heterogeneous echogenicity (Fig. 1A). An axillary lymph node (17 mm long-axis) showed cortical thickening and effaced hilum (Fig. 1B). Whole-body CT revealed no distant metastases. A pathological biopsy of the right breast mass revealed invasive ductal carcinoma of non-special type, with a histological grade of 2. Immunohistochemical analysis demonstrated estrogen receptor (ER) (90 % +), progesterone receptor (PR) (80 % +), human epidermal growth factor receptor 2 (HER-2) expression (2+, and fluorescence in situ hybridization (FISH) -), and Ki-67 (10 % +). Pre-chemotherapy clinical staging was cT4N2M0 (Stage IIIB). The patient underwent 6 cycles of neoadjuvant chemotherapy with a docetaxel and carboplatin regimen, achieving a clinical response assessed as partial remission. The patient was subsequently transferred to the Department of Breast Surgery for surgical intervention. Preoperative breast ultrasound identified the mass (27 mm maximal diameter) (Fig. 1C), and an axillary lymph node (18 mm long-axis) (Fig. 1D). Preoperative breast magnetic resonance imaging (MRI) identified a mass-like lesion adjacent to the nipple, measuring approximately 41 mm × 24 mm × 21 mm. The lesion displayed lobulated margins, and a washout pattern observed on the time-intensity curve (Fig. 2A). Post-chemotherapy clinical stage was confirmed as ycT4N2M0 (Stage IIIB). On January 17, 2025, the patient underwent a modified radical mastectomy for right breast cancer. Pathological examination confirmed invasive ductal carcinoma of the right breast, measuring 40 mm in diameter, with the Miller-Payne (MP) grade of I and the Residual Cancer Burden (RCB) grade of III. The tumor involved the skin and nipple-areolar complex, while the basal and skin surgical margins were negative for carcinoma. Metastatic carcinoma was found in 11 of 18 right axillary lymph nodes. Final pathological stage was ypT4N3M0 (Stage IIIC). Immunohistochemical analysis showed ER (80 % +), PR (80 % +), HER-2 (2+, and FISH -), and Ki-67 (10 % +) (Fig. 2B, C, D). The patient subsequently received radiotherapy and endocrine therapy with tamoxifen (10 mg twice daily, orally). Favorable outcomes were observed during recent follow-up evaluations.Fig. 1. Ultrasonography of primary right breast mass (A) and right axillary lymph node (B) prior to neoadjuvant chemotherapy. Ultrasonography of the right breast mass (C) and right axillary lymph node (D) post-neoadjuvant chemotherapy.Fig. 1. Fig. 2MRI image of the right breast (A). Clinicopathological examination of the resected breast tissue, immunohistochemical staining of the invasive ductal carcinoma; (H&E staining; magnification × 40) (B); (H&E staining; magnification × 400) (C); (HER-2 staining; magnification × 400) (D).Fig. 2
Discussion
3
Clinical studies have demonstrated that male patients with breast cancer tend to present with more advanced disease at diagnosis compared to their female counterparts, characterized by larger tumor size and higher rates of axillary lymph node involvement [5]. The present study reports a case of a male patient diagnosed with breast cancer, staged as T4 according to the tumor-node-metastasis (TNM) classification system, and presenting with concurrent multiple lymph node metastases. Gao et al. [6] reported that a case of MBC received neoadjuvant chemotherapy and achieved pathological complete response (pCR). However, the patient in the present study exhibited partial remission, which may be associated with low Ki-67 expression. The occurrence of dual primary malignancies involving MBC and another primary malignant tumor is exceptionally rare, particularly in cases involving leukemia. Previous studies have documented rare instances in which patients, following complete remission of acute lymphoblastic leukemia (ALL), were subsequently diagnosed with MBC several years thereafter [7,8]. Besides, several studies have documented the development of AML in female breast cancer patients following chemotherapy [9,10]. The present study reports the first documented case of a patient with AML-M3a who, following multiple chemotherapy regimens and sustained complete remission, subsequently developed primary MBC. We hypothesize that the series of chemotherapy regimens administered for this patient's AML treatment may have induced somatic gene mutations, potentially leading to the development of MBC. However, comprehensive genomic profiling via next-generation sequencing (NGS) to validate the presence of such mutations was not performed due to prohibitive financial constraints. Consequently, analysis of a potential causal relationship between these two malignancies in this patient was precluded. Although the occurrence of leukemia and primary MBC is rare, it is imperative to prioritize routine clinical breast examinations in male patients with a history of hematologic malignancies to ensure early detection and timely intervention.
Conclusion
4
This case report presents the first documented occurrence of MBC in a patient who achieved sustained complete remission of AML, highlighting the need for long-term surveillance of secondary malignancies in AML survivors. The findings may inform clinical decision-making regarding multidisciplinary management strategies for such rare dual malignancies.
Author contribution
Miao Deng: The conception and design of the study. Weiqiang Qiao: Data curation, Writing-Original draft preparation. Peng Li: Writing-Reviewing and Editing. Chang Chang: Supervision, Software. Mengnan Fan: Visualization, Investigation.
Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Ethical approval
This study was approved by the Ethics Committee of the First Affiliated Hospital of Henan University of Science and Technology.
Guarantor
Miao Deng.
Research registration number
Not applicable.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare that there is no conflict of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1van den Bruele A.B.Williams A.Weiss A.Commentary and updates on the management of male breast cancer Ann. Surg. Oncol.322025226522703980604710.1245/s 10434-024-16756-x PMC 12279442 · doi ↗ · pubmed ↗
- 2Wang X.Jia Z.Li J.Yang H.Sun X.Liu Y.A case of ALK-positive anaplastic large cell lymphoma of the male breast Int. Med. Case Rep. J.1620237477553802057710.2147/IMCRJ.S 434109 PMC 10663166 · doi ↗ · pubmed ↗
- 3Acostamadiedo M.A.Avendaño-Capriles C.A.Lemos J.A.Gorman E.Acostamadiedo J.M.Metastatic breast cancer presenting as pulmonary nodules and right axillary lymph node in a male with chronic lymphocytic leukemia Case Rep. Oncol.142021160816153495000410.1159/000519744 PMC 8647123 · doi ↗ · pubmed ↗
- 4Kerwan A.Al-Jabir A.Mathew G.Sohrabi C.Rashid R.Franchi T.Nicola M.Agha M.Agha R.A.Revised surgical case report (SCARE) guideline: an update for the age of artificial intelligence Premier J. Sci.102025100079
- 5Gao Y.Zhang M.Sun G.The features of male breast cancer in China: a real-world study BREAST 76202410376210.1016/j.breast.2024.103762 PMC 1125995738924994 · doi ↗ · pubmed ↗
- 6Gao W.An A.Yang L.Wang Q.Neoadjuvant chemotherapy for male breast cancer: a case report Asian J. Surg.472024373037313870426510.1016/j.asjsur.2024.04.100 · doi ↗ · pubmed ↗
- 7Lowe T.Luu T.Shen J.Male breast cancer 15 years after allogeneic hematopoietic cell transplantation including total body irradiation for recurrent acute lymphoblastic leukemia Onkologie 3120082662691849751710.1159/000121395 · doi ↗ · pubmed ↗
- 8Latz D.Alfrink M.Nassar N.Beyerle C.Breast cancer in a male patient after treatment of acute lymphoblastic leukemia including total body irradiation and bone marrow transplantation Onkologie 2720044774791558597910.1159/000080369 · doi ↗ · pubmed ↗