An unusual distal tibial metastasis from urothelial carcinoma: A case report
Tran Ngoc An Huynh, Darren Trinh, Janan Chandrananth, James Sewell

TL;DR
This case report describes a rare instance of bladder cancer spreading to the tibia, highlighting the importance of considering unusual metastatic locations.
Contribution
The report presents a rare case of distal tibial metastasis from urothelial carcinoma, expanding the known patterns of cancer spread.
Findings
Bladder cancer metastasized to the distal tibia in an 84-year-old patient.
Surgical fixation and radiotherapy were used to manage the metastasis.
Unusual bone metastasis locations should be considered in cancer patients with unexplained bone pain.
Abstract
Bladder cancer (BCa) frequently metastasizes to bones, typically affecting the spine and pelvis. Presented here is a case of rare extensive distal tibia metastasis in an 84-year-old female with invasive high-grade urothelial carcinoma, who suffered from rapidly progressive ankle pain and reduced mobility. Imaging and biopsy confirmed metastatic urothelial carcinoma in the tibia, which was managed with surgical fixation and palliative radiotherapy. Although bone metastases in BCa commonly affect other sites, clinicians should consider atypical locations like the tibia in patients with unexplained bone pain. Early diagnosis and intervention are essential for improving patient outcomes and quality of life.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
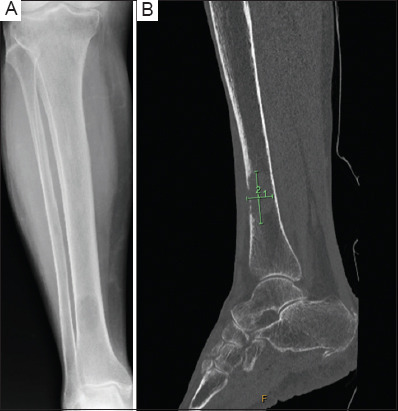 Figure 1
Figure 1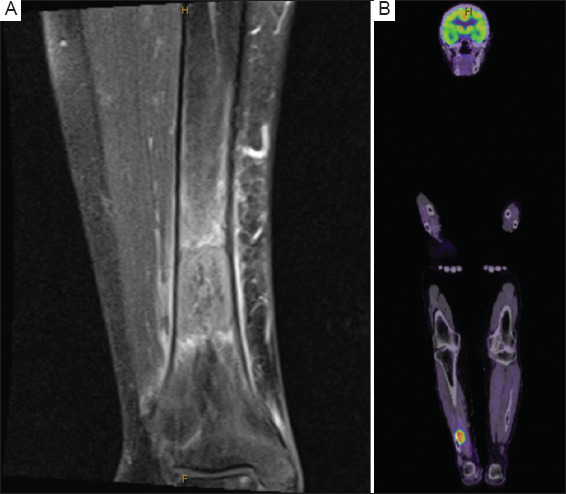 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer Diagnosis and Treatment · Medical Imaging and Pathology Studies · Urinary and Genital Oncology Studies
1. Background
Bladder cancer (BCa) is a prevalent urological malignancy that results in roughly 213,000 deaths worldwide each year.1 The most common sites of metastasis are the lymph nodes and bones, with the pelvis and spine being common locations for bone metastasis (BM).2,3 This was the first case report, to our knowledge, to describe a BM in the distal tibia from BCa.
2. Case presentation
An 84-year-old female was referred by an urologist to a secondary urologist for consideration of a robotic partial cystectomy following the diagnosis of invasive high-grade urothelial carcinoma within a bladder diverticulum. The diagnosis was made based on a transurethral resection of bladder tumor (TURBT) performed after she presented with hematuria. Her hemoglobin levels and renal function were within normal limits. A computed tomography (CT) scan of the chest, abdomen, and pelvis revealed thickening of the left bladder wall, with no hydronephrosis and no evidence of metastatic disease.
A repeat rigid cystoscopy performed 4 weeks after the initial TURBT showed multifocal recurrence along the left posterior and lateral bladder wall. The patient then underwent a TURBT, which revealed invasive (pT1) high-grade papillary urothelial carcinoma with 30% glandular differentiation.
Perioperatively, she reported worsening pain in her right ankle and left buttock over 4 weeks, leading to reduced mobility. X-ray of her right leg demonstrated a lesion in her distal tibia (Figures 1A). Magnetic resonance imaging (MRI) of her right ankle and further a CT scan revealed a 41-mm intramedullary lobulated mass in the distal tibia with contrast enhancement (Figures 1B and 2A). In addition, a fludeoxyglucose F18 positron emission tomography (PET) identified BM in the left distal sacrum and the distal right tibia (Figure 2B). A CT-guided biopsy of the tibial lesion confirmed metastatic carcinoma of urothelial origin.
The patient, with a Mirels score of 11, underwent prophylactic embolization and surgical fixation of the distal tibia. In addition, she received palliative radiotherapy to both the sacrum and tibia, which initially provided pain relief and improved mobility for 3 weeks. Unfortunately, a follow-up X-ray taken after 6 weeks showed that the lesion had grown to 150 mm. Due to the patient’s frailty, systemic chemotherapy was deemed unsuitable, and she transitioned to palliative care.
3. Discussion
BM in BCa occurs through several processes, including epithelial-to-mesenchymal transition, angiogenesis, intravasation, extravasation, and interactions with the bone microenvironment.4 The common sites of BCa-related BM are the spine, pelvis, ribs, skull, femur, and proximal end of the humerus.4
According to the European Association of Urology 2024 guidelines, integrating multimodal imaging enhances diagnostic accuracy for detecting BCa metastases.5 Plain radiographs are useful for identifying compression fractures and osteolytic metastases but are less reliable for spotting osteoblastic lesions. CT and MRI provide superior accuracy for identifying metastases and differentiating benign from malignant lesions. PET is valuable for assessing early tumor formation and metabolism, offering greater differentiation between benign and malignant lesions; however, it lacks precise anatomical resolution.4
The management of BM focuses on inhibiting disease progression and alleviating symptoms. Radiotherapy serves as a palliative, non-invasive treatment and typically improves pain within 2 – 6 weeks following therapy.4 Surgical intervention prevents or stabilizes fractures, preserves mobility, and relieves bone pain.4 Mirels proposed a scoring system that assesses the risk of fracture based on four factors: the location of the lesion, the nature of the lesion (lytic vs. blastic), its size, and the presence of pain.6 According to Mirels’ criteria, prophylactic fixation is recommended when a lesion scores 9 or higher, indicating a high risk of fracture.6
Brennan et al.7 described a 61-year-old male with a proximal tibial metastasis secondary to BCa, which was successfully managed with a total knee replacement and chemotherapy. Similarly, Kastanis et al.8 reported a 58-year-old male with metastasis to the tibial shaft, treated with intramedullary nailing for structural stabilization. To our knowledge, the present case is the first reported instance of a distal tibia BM from BCa.
4. Conclusion
Although bone is a common site for metastasis in BCa, clinicians should maintain a high index of suspicion for atypical sites of BM in patients presenting with unexplained pain and impaired daily functioning. As these sites are outside the standard imaging template for staging scans, recognizing the possibility of tibial BM in BCa is crucial for timely diagnosis and intervention.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Zhang Y Rumgay H Li M Yu H Pan H Ni J The global landscape of bladder cancer incidence and mortality in 2020 and projections to 2040. J Glob Health. 2023;1304109. doi:10.7189/jogh.13.0410937712386 10.7189/jogh.13.04109 PMC 10502766 · doi ↗ · pubmed ↗
- 2Shinagare AB Ramaiya NH Jagannathan JP Fennessy FM Taplin ME Van den Abbeele AD Metastatic pattern of bladder cancer:Correlation with the characteristics of the primary tumor. AJR Am J Roentgenol. 2011;196(1):117–122. doi:10.2214/AJR.10.503621178055 10.2214/AJR.10.5036 · doi ↗ · pubmed ↗
- 3Taher AN Kotb MH Bone metastases in muscle-invasive bladder cancer. J Egypt Natl Canc Inst. 2006;18(3):203–208 17671529 · pubmed ↗
- 4Yi L Ai K Li X Li Z Li Y Bone metastasis in bladder cancer. J Pers Med. 2022;13(1):54. doi:10.3390/jpm 1301005436675715 10.3390/jpm 13010054 PMC 9864951 · doi ↗ · pubmed ↗
- 5EAU Guidelines. 2024. Available from: https://uroweb.org/guidelines/muscle-invasive-and-metastatic-bladder-cancer/chapter/introduction. [Last accessed 2024 Dec 16]
- 6Jawad MU Scully SP In brief:Classifications in brief:Mirels'classification:Metastatic disease in long bones and impending pathologic fracture. Clin Orthop Relat Res. 2010;468(10):2825–2827. doi:10.1007/s 11999-010-1326-420352387 10.1007/s 11999-010-1326-4PMC 3049613 · doi ↗ · pubmed ↗
- 7Brennan D Kelly ME Nason GJ Collins-Smyth C Mc Guire BB Lennon GM Tibial metastasis from muscle invasive bladder carcinoma:An unusual site. Curr Urol. 2013;7(3):160–162. doi:10.1159/00034355624917780 10.1159/000343556 PMC 4024504 · doi ↗ · pubmed ↗
- 8Kastanis G Bachlitzanaki M Pantouvaki A Magarakis G Spyrantis M Unusual tibial site metastases from a muscle invasive urothelial carcinoma:A rare case report. Int J Innov Res. Med Sci. 2020;5(9):382–384. doi:10.23958/ijirms/vol 05-i 09/948