The prognosis of pain and function in people with hand and thumb base osteoarthritis: a systematic review
Victoria Jansen, Anna Selby, Suzanne Toft, Joanne Greenway, Michelle Marshall, Elaine Nicholls, Danielle A. van der Windt

TL;DR
This study reviews how hand and thumb osteoarthritis affects pain and function over time and identifies factors that predict worsening symptoms.
Contribution
A systematic review of longitudinal studies to identify prognostic factors for pain and function in hand osteoarthritis.
Findings
Over 10 years, hand function and grip strength tend to deteriorate while pain changes little on average.
Baseline pain and diabetes are moderately associated with worsening function and pain.
Individual variation in symptom progression is evident, with limited evidence for other prognostic factors.
Abstract
This systematic review has summarized evidence regarding the course of hand pain, hand function, and prognostic factors that predict changes in symptoms in people with hand and thumb base osteoarthritis . A systematic search of electronic databases was conducted for longitudinal studies on hand osteoarthritis. Two reviewers assessed eligibility quality appraisal, and extracted data on pain, function and prognostic factors. A narrative synthesis was undertaken, and the strength of the evidence was appraised using a modified Grading of Recommendations, Assessment, Development, and Evaluations approach. Of 9523 articles identified, 24 papers with 8,496 patients met the inclusion criteria. Twelve studies reported on the course of hand pain and 13 on hand function. 25–29% of participants reported worsening pain and 23–59% a deterioration in hand function over 10 years. There is moderate…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
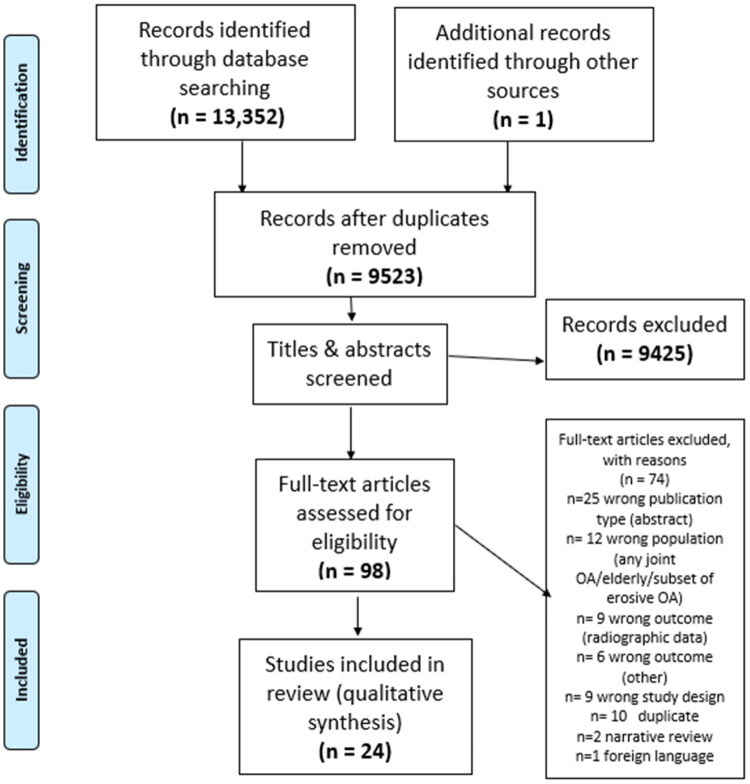 Figure 1
Figure 1| Inclusion | Exclusion | |
|---|---|---|
| Participants | Adult (over 18 years) with a diagnosis of hand OA or primary TBOA confirmed clinically (American College of Rheumatology (ACR) criteria for hand OA, or clinical diagnosis of TBOA and/or radiographic (Kellgren Lawrence ≥2 for hand OA or TBOA or Eaton Littler ≥1 for TBOA). | Traumatic, congenital, or hormonal abnormalities. |
|
| Prospective or retrospective observational studies describing the change in hand pain and functional difficulty. | Assessment of the presence of hand pain or functional difficulty only by (yes/no). |
|
| Hand pain and hand function. | Radiographic only. |
| Study and cohort | Country | Sample size and setting | Age in years (SD/ range) | % Female | Proportions meeting diagnostic criteria for hand OA | Measures of hand pain and hand function |
|---|---|---|---|---|---|---|
| Allen [ | USA | 67.7 (8.2) | 80% | 100% rHOA | AUSCAN (scale not stated), | |
| Bjisterbosch [ | Netherlands | 59.5 (7.4) | 83% | 100% ACR HOA or rHOA | AUSCAN pain (0–20) | |
| Courties [ | France | 63.8 (7.1) | 69% | 100% rHOA | AUSCAN pain, function and stiffness (altered scale 0–300) | |
| Haugen [ | Norway | 67.9 (5.5) | 90% | 100% clinical diagnosis HOA | AUSCAN pain (0–20) | |
| Haugen [ | Norway | 61.5 (5.7) | 91% | 100% clinical diagnosis HOA | AUSCAN pain (0–20 | |
| Meersseman [ | Belgium | 62.2 (45–84) | 86% | 100% ACR HOA and rHOA | VAS (0–100) | |
| McQuillan [ | USA | 56.4 (7.6) | 53% | 100% clinical diagnosis CMCJ OA | AUSCAN pain (0–20) | |
| Damman [ | Netherlands | 60.9 (8.4) | 84% | 100% ACR HOA | FIHOA (0–30) | |
| Gil [ | USA | NR | NR | 100% clinical diagnosis of CMCJ OA | PRWHE pain (0–50) | |
| Van Beest [ | Netherlands | 59.2 (7.3) | 81% | 89% ACR HOA, 100% clinical assessment | AUSCAN pain (0–20) | |
| Botha Scheepers [ | Netherlands | 59.2 (7.3) | 79% | 75% ACR HOA, 100% clinical diagnosis | AUSCAN pain (0–20) | |
| Liu [ | Netherlands | 61.4 (8.9) | 88% | 91% ACR HOA, 100% clinical diagnosis | Pain on palpation (0–90) | |
| Magnusson [ | Norway | 61.6 (5.6) | 91% | 80% ACR HOA, 100% clinical diagnosis | AUSCAN pain (0–20) | |
| Vanhaverbeke [ | Belgium | 62.9 (8.0) | 85% | 100% ACR HOA and rHOA. | VAS pain (0–100) | |
| Neuprez [ | Belgium | 69 (61–75) | 90% | 100% rHOA and clinical HOA | VAS pain (0–100) | |
| Snyder [ | USA | 63.1 (7.4) | 72% | 100% rHOA and clinical HOA | Number of symptomatic hand joints | |
| Studies below also included participants without a diagnosis of hand OA | ||||||
| Dieppe [ | UK | 59 (9.4) hand alone, | 86% | 53% rHOA and symptomatic HOA | Self-report hand pain intensity (none/mild/moderate severe) | |
| Cvijetic [ | Croatia | 54.9 (9.5) males 56.4 (8.4) females | 56% | rHOA 36% males, 32% females. | Grip strength (kilopounds) | |
| Ding [ | Finland | 54.5 | 100% | 19% rHOA | Joint pain hand diagram (no pain = 0/mild = 1/moderate = 2/ severe= 3) | |
| Marshall [ | UK | 64.2 (8.2) | 62% | 30% ACR HOA, 76% rHOA in 1jt | AUSCAN pain (0–20) | |
| Marshall [ | UK | 64.8 (8.3) | 60% | 65% rHOA and symptomatic HOA, 35% unclassified as symptomatic with KL ≤ 2 | AUSCAN pain (0–20) | |
| Scherzer [ | USA | 59.5 (7.4) | 68% | 8% rHOA GOGO criteria* | AUSCAN pain (0–20) | |
| Siviero [ | Italy/Europe | 73.7 (5.0) | 52% | 17% clinical HOA | AUSCAN pain (0–20) | |
| Van Beest [ | Netherlands | 60.7 (8.3) | 83% | 92% ACR HOA | VAS right hand pain (0–100) | |
|
|
|---|
| QUIPS Quality in prognosis studies tool |
| Baseline | Follow up | Y/N | Detail | |||
|---|---|---|---|---|---|---|
|
| ||||||
| Allen [ | 4.1 (1.1) | Hand pain and function | Y | Small average deterioration pain and function (may not be clinically significant). 43–49% rated as globally had worsened. | ||
| AUSCAN 34.0 (12.3) | 35.3 (13.0) | AUSCAN 1.3 (10.4) | ||||
| Grip and pinch strength (Kg) | ||||||
| L: 46.9 (24.0) | L: 47.5 (20.6) | R: −0.4 (15.4) | ||||
| L: 12.0 (6.1) | L: 11.4 (4.7) | R: −0.4 (6.3) | ||||
| Haugen [ | 4.7 (0.4) | Hand pain | N | Improvements in pain (likely clinically significant as median is 20% change, MCII used elsewhere is 1.4) | ||
| NR | NR | AUSCAN Median change (IQR) −4.0 (–6.0, −2.0) | ||||
| Haugen [ | 7 | Hand pain | Y | Variable: average small deterioration in pain, function, and strength, clinically significant in 47%, but 32% improved. | ||
| AUSCAN 0.8 (3.4) Improvements beyond MCII pain 21.1%, worsening beyond MCII pain 28.9% | ||||||
| Hand function | ||||||
| AUSCAN 1.2 (6.3) | ||||||
| Grip strength | ||||||
| R −0.7 (6.9), | ||||||
| Variable: pain and number of tender joints reduced. Function and strength deteriorated. Authors felt disease progressed more rapidly early on, focus on erosive OA. | ||||||
| Meersseman [ | 5.8 | Hand pain | N | Variable: pain and number of tender joints reduced. Function and strength deteriorated. Authors felt disease progressed more rapidly early on, focus on erosive OA. | ||
| VAS 41.6 (25.0) | 33.3 (28.2) | |||||
| Hand function | ||||||
| FIHOA 8.7 (6.4) | 9.8 (6.5) | |||||
| Grip strength (kg) | ||||||
| Dominant 19.1 (8.6) | 15.9 (8.3) | |||||
| No. painful joints | ||||||
| 3.4 (3.3) | 2.8 (3.4) | |||||
| No. tender hand joints | ||||||
| 3.0 (3.1) | 4.8 (3. 8) | Median (IQR) −2.0 (–5.0 to 1.0) | ||||
| Damman [ | 2 | NR | NR | Hand function proportions given are those with worsening function/ total followed up | Y | Deteriorating function, BUT better understanding and less emotions and consequences perceived because of their OA. |
| FIHOA 3.7 (2.6), 50% (157/311) | ||||||
| Disability | ||||||
| HAQ 0.4 (0.2) | ||||||
| Van Beest [ | 2 | NR | NR | Pain: Joint level changes | N | 65% of joints with pain at baseline had reduced pain |
| 65% (76/116) of painful joints at baseline had less pain at FU. | ||||||
| Liu [ | 1 | Hand pain NR | NR | NR | Y | Function deteriorated (over half the sample is missing) |
| Hand function | ||||||
| FIHOA 8.0 (range 0–24) | 9.0 (0–28) | |||||
| McQuillan [ | 1.5 | Hand pain | NR | N | Pain reduced, and function improved. Early-stage radiographic disease, surgical treatments provided, and those cases excluded from FU. | |
| AUSCAN (+ range) 6.6 (4.1; 0–18) | 6.4 (4.0; 0–19) (19.7; 0–19) | |||||
| Hand function | NR | |||||
| AUSCAN (+ range) 10.9 (7.7; 0–31) | 10.3 (6.5; 0–33) | |||||
| Gil [ | 3 | Hand pain | NR | N | Pain and function improved. | |
| PRWHE 17.2 (11.5) | 18mo 15.6 (10.6) | |||||
| Hand function | NR | |||||
| PRWHE 13.0 (13.4) | 18mo 10.8 (12.1) | |||||
| Magnusson [ | 7 | NR | NR | Hand pain | Y | Average changes not clinically significant |
| AUSCAN 0.7 (3.6) | ||||||
| Hand function | ||||||
| AUSCAN 1.1 (6.4) | ||||||
| Change in no. Symptomatic hand joints | ||||||
| 0.9 (3.1) | ||||||
| Vanhaverbeke [ | 9.7 | Hand pain | N | Pain and number of tender joints reduced, MCII for AUSCAN. | ||
| AUSCAN 19.6 (10.9) | T1: 17.2 (10.8) | Over 10 years mean differences AUSCAN −1.84 (NS) | ||||
| Hand function | ||||||
| AUSCAN T0: 39.3 (21.3) | T1: 40.2 (20.0) | 4.52 ± 19.91 | ||||
| Grip strength (kg) | ||||||
| T0: 19.0 (9.0) | T1: 15.9 (8.3) | Dominant hand ( | ||||
| No. Swollen hand joints | ||||||
| T0: 1.4 (1.8) | T1:2.6 (2.7) | Nos swollen joints increased ( | ||||
| No. tender hand joints | ||||||
| T0: 3.1 (3.4) | T1: 4.8 (3.8) | No. tender joints decreased ( | ||||
| Neuprez [ | 2, 13% | Hand pain | N | Average changes not significant. Radiological progression was not associated with changes in self-reported pain and function. | ||
| VAS 44.2 (23.7) AUSCAN 44.3(27.4) | 42.9 (27.7) | 25% deterioration >8 MCID AUSCAN pain | ||||
| Hand function | ||||||
| AUSCAN 45.9 (27.0) | 48 (28.2) | 34.7% deterioration >15 MCID total AUSCAN score | ||||
| No. painful hand joints | ||||||
| 3.57 (6.2) | 3.34 (5.7) | |||||
| No. tender hand joints | ||||||
| 7.9 (8.6) | 7.8 (8.6) | |||||
| Bjisterbosch [ | 6.1 (range 5–7.8) 19% | Hand pain | Y | Yes: small average deterioration (may not be clinically significant) | ||
| AUSCAN 6.7 (4.8) | 7.4(4.9) | 0.7 95% CI (0.3–1.2) | ||||
| Hand function | ||||||
| AUSCAN 11.8 (8.9) | 13.9 (8.9) | 2.1 95% CI (1.3–2.9) | ||||
| Hand Joint palpation | ||||||
| NR | NR | NR | ||||
| Botha Scheepers [ | 2, | Hand pain | Y | Yes: small deterioration in pain and function may not be clinically significant. | ||
| AUSCAN 6.2 (4.6) | 7.2 (4.8) | 1.0 (4.0), 95% CI 0.4 to 1.6, SRM 0.25 | ||||
| Hand function | ||||||
| AUSCAN 11.1 (8.8) | 12.5 (9.1) | AUSCAN 1.4 (6.1) 95% CI 0.5 to 2.3, SRM 0.23 | ||||
| Snyder [ | 12, | Hand pain | N | No: Majority did not experience symptoms in additional joints. No measures of severity of pain. | ||
| NR | NR | 31% experienced symptoms in additional joint(s) over 12 years. Change in no. symptomatic joints was median (IQR) 0(0–1). | ||||
| Courties [ | 2.6 (0.7) | Hand pain | N | Small average improvement FIHOA (may not be clinically significant – over half the sample are missing). rHOA not symptomatic. | ||
| Reports AUSCAN score worsened (no follow-up data presented) | NR | |||||
| Hand function | ||||||
| FIHOA 3.9 (4.8) | 3.2 (4.4) | 23% ( | ||||
|
| ||||||
| Dieppe [ | 8 | Hand pain and change in hand pain and overall condition. | Y | Proportions with severe pain have increased and those with no pain have reduced at both time points. | ||
| Hand only: | 3 years: none 5%, | Self-reported change index joint hand OA only: | ||||
| Hand and knee OA: none 3%, mild 23%, moderate 38%, | 3year: none 2%, mild 22%, moderate 46%, severe 29% | Self-reported change index joint hand and knee OA: | ||||
| Van Beest [ | 2 | Hand pain | N | Reports on thumb base pain only, not hand pain or hand function at 2 yrs. MRI and radiographic scores also remained stable in the majority. | ||
| NR | NR | Self-report thumb base: | ||||
| Cvijetic [ | 10 | Strength Grip (Kp) | Y Deterioration in grip strength | Over 10 years males lost an average of 5 kp/ 7% and females an average of 1.5–3 Kp or 4–9% of their grip strength. | ||
| Males | R 65 (24.3) | NR | ||||
| Females | R 32.7 (13.2) | |||||
| Ding [ | 5 | Hand pain | Unclear | High probability of persistent pain but severity not described (some may have worsened some stayed the same). 8.3% improved right hand and 12% left. | ||
| 8.3% had pain at baseline (severity not reported) | ||||||
| Marshall [ | 7 | Hand pain | Global perceived change in hand problem | Y | Variable but majority (56%) deteriorated. | |
| AUSCAN baseline scores not presented only scores within photographic change groups so unusable | improved: 17%, no change: 26%, deteriorated: 56% | |||||
| Marshall [ | 3 | Hand pain | Y | Yes: with OA meeting subgroup criteria | ||
| AUSCAN (and 95% CI) | AUSCAN (and 95% CI) | Unclassified group little or no change in pain in 3 years, all other groups showed small increases pain (0.5–1.5) | ||||
| Hand function | ||||||
| AUSCAN IPJ and thumb: 9.9 (8.1, 11.7) Thumb: | AUSCAN IPJ and thumb: | Unclassified group little or no change in disability in 3 years | ||||
| Scherzer [ | 12 | Hand pain | N | Variable small numbers in the change groups, majority not in high or low pain groups and unchanged (all numbers increased included incident hand OA over follow up) | ||
| GOGO low pain AUSCAN: 37 (4.4%) | 6yrs 85 (10.4%) | Low pain to high pain 36 | ||||
| Siviero [ | 1.5 | Hand pain | N | Unclear – only 16.7% met ACR criteria for hand OA (the average AUSCAN hand pain score indicates hand problems). | ||
| NR – reports weighted baseline AUSCAN pain whole group 7.6 (15.2) | NR | |||||
| Hand function | ||||||
| AUSCAN worsening group 10.4 (±14.73) | 24.5 (±18.1), | MCID score of AUSCAN function +4 ‘worse’ identified 453 (24.4%) with physical function decline at 12–18 months. MCID −2 ‘improved’ identified 23.5% (432) | ||||
| 1 | 2 | 3 | 4 | ||||
|---|---|---|---|---|---|---|---|
| Outcome | Evidence base (no. studies; relevant sample size) | Range of effect | Quality of studies for this outcome | Inconsistency | Indirectness | Imprecision | Strength of evidence (amended GRADE) |
| Change in hand pain (1–3 years) | 6 prospective studies [7, | At person level average AUSCAN pain changed very little increased 0.5–1.5 (0–20 scale) or decreased. Estimate for proportion with worsening pain are 25%. | −1 | −1 | +1 | −1 | ⊕□□□ |
| Change in hand pain (4–10 years) | 5 prospective studies [ | At person level average AUSCAN pain changed very little increased 0.7–0.8 (0–20 scale) or decreased. Estimate for proportion with worsening pain 29%. | −1 | −1 | +1 | +1 | ⊕⊕□□ |
| Change in hand function (1–3 years) | 9 prospective studies, [7, | At person level change scores for function deteriorated from an average of 1.4–5.6 on AUSCAN (0–36 scale). Estimates for proportion with worsening function were 23–42%. | −1 | −1 | +1 | +1 | ⊕⊕□□ |
| Change in hand function (4–10 years) | 5 prospective studies [ | Small average deterioration in function, average change score between 1.1 and 2.1 (0–36 scale) Estimates for proportion with worsening function were 47–59%. | −1 | +1 | +1 | +1 | ⊕⊕⊕□ |
| Changes in grip or pinch strength (4–10 years) | 5 prospective studies [ | Small mean changes in grip short- term (–1.1– +0.4 kg) with a trend for greater deterioration over longer time periods. | −1 | +1 | +1 | +1 | ⊕⊕⊕□ |
| Prognostic factor | Study: author year | Follow up (years) | Risk of bias | Definition of progression | Results of univariable/multivariable analyses | Univariable/ multivariable analyses | Association with OA prognosis |
|---|---|---|---|---|---|---|---|
|
| Dieppe [ | 8 | HIGH | Patient reported outcomes for pain and overall condition (better, same, worse) | Descriptive data (chi squared and significance at 5% level) NS | Univariable analysis | (o) |
| Vanhaverbeke [ | 9.7 | HIGH | AUSCAN function (0–90), change ≥ 7.2 or | OR (95% CI) 1.94 (0.32,11.9) | Univariable analysis | (o) | |
| Neuprez [ | 2 | HIGH | AUSCAN (0–300) change > MCID 15, | Not statistically significant estimate not provided. | Multivariable analysis | (o) | |
| Snyder [ | 12 | HIGH | Change in number of symptomatic joints (0–30), (pain/ tenderness and radiographic OA in the same joint) | OR (95% CI) 1.25 (0.72,2.16) | Multivariable: age, sex, race, education, BMI, weight gain >5%, HOA baseline values (KLG, nos radiographic and symptomatic joints) | (o) | |
|
| Dieppe [ | 8 | HIGH | patient reported outcomes and overall condition (better, same, worse) | Descriptive data (chi squared and significance at 5% level) NS | Univariable analysis | (o) |
| Ding [ | 5 | HIGH | Incident/persistent pain: ≥1 joint thumb, index, or middle finger or separately ring or little finger, vs reference group of no pain at either time point radial or separately ulnar digits | PR (95% CI) (Dentist vs teacher [teacher = ref]) 1.34(0.89, 2.02) | Multivariable: age, occupation, BMI, smoking, leisure hand activity, work status, radiographic joint OA | (o) | |
|
| Dieppe [ | 8 | HIGH | patient reported outcomes for pain and overall condition (better, same, worse) | Descriptive data (chi squared and significance at 5% level) NS | Univariable analysis | (o) |
| Vanhaverbeke [ | 9.7 | HIGH | AUSCAN function (0–90), change ≥ 7.2 or | OR (95% CI) 0.93 (0.87, 0.99) | Univariable analysis | (–) | |
| Ding [ | 5 | HIGH | Incident/persistent pain: ≥1 joint thumb, index or middle finger or separately ring or little finger, vs reference group of no pain at either time point radial or separately ulnar digits | PR (95% CI) 1.01(0.96, 1.08) | Multivariable: age, occupation, BMI, smoking, leisure hand activity, work status, radiographic joint | (o) | |
| Neuprez [ | 2 | HIGH | AUSCAN (0–300) change > MCID 15, | Not statistically significant, estimate not provided. | Multivariable analysis | (o) | |
|
| Ding [ | 5 | HIGH | Incident/persistent pain: ≥1 joint thumb, index or middle finger or separately ring or little finger, vs reference group of no pain at either time point radial or separately ulnar digits | PR (95% CI) smoking ever 0.97(0.62, 1.54) | Multivariable: age, occupation, BMI, smoking, leisure hand activity, work status, radiographic joint OA | (o) |
| Courties [ | 2.6 | HIGH | Deterioration from baseline scores AUSCAN/FIHOA | OR (95% CI) 1.41 (0.39, 5.09) | Univariable analysis | (o) | |
| Neuprez [ | 2 | HIGH | AUSCAN (0–300) change > MCID 15, | Not statistically significant, estimate not provided. | Multivariable analysis | (o) | |
|
| Courties [ | 2.6 | HIGH | Deterioration from baseline scores AUSCAN/FIHOA | OR (95% CI) 1.01 (0.64, 1.9) | Univariable analysis | (o) |
| Neuprez [ | 2 | HIGH | AUSCAN (0–300) change > MCID 15, | Not statistically significant, estimate not provided. | Multivariable analysis | (o) | |
|
| Courties [ | 2.6 | HIGH | Deterioration from baseline scores AUSCAN/FIHOA | OR (95% CI) 0.75 (0.4,1.44) | Univariable analysis | (o) |
| Neuprez [ | 2 | HIGH | AUSCAN (0–300) change > MCID 15, | Not statistically significant, estimate not provided. | Multivariable analysis | (o) | |
|
| Courties [ | 2.6 | HIGH | Deterioration from baseline scores AUSCAN/FIHOA | OR (95% CI) 1.38 (0.79, 2.39) | Univariable analysis | (o) |
| Dieppe [ | 8 | HIGH | patient reported outcomes for pain and overall condition (better, same, worse) | Descriptive data (chi squared and significance at 5% level) NS | Univariable analysis | (o) | |
| Vanhaverbeke [ | 9.7 | HIGH | AUSCAN function (0–90), change ≥ 7.2 or | OR (95% CI) 0.99(0.93, 1.05) | Univariable analysis | (o) | |
| Ding [ | 5 | HIGH | Incident/persistent pain: ≥1 joint thumb, index, or middle finger or separately ring or little finger, vs reference group of no pain at either time point radial or separately ulnar digits | PR (95% CI) 1.23(0.86, 1.76) | Multivariable: age, occupation, BMI, smoking, leisure hand activity, work status, radiographic joint OA | (o) | |
| Siviero [ | 1.5 | LOW | MCID score of >4 AUSCAN function | RR (95% CI) 0.95 (0.79, 1.15) | Multivariable: sex, age, country, education level | (o) | |
| Neuprez [ | 2 | HIGH | AUSCAN (0–300) change > MCID 15, | Not statistically significant, estimate not provided. | Multivariable analysis | (o) | |
|
| Siviero [ | 1.5 | LOW | MCID score of >4 AUSCAN function | RR (95% CI) 1.01 (0.83, 1.21) | Multivariable: sex, age, country, education level | (o) |
| Dieppe [ | 8 | HIGH | patient reported outcomes and overall condition (better, same, worse) | Descriptive data (chi squared and significance at 5% level). Patients using NSAIDs were more likely to report improvement (24%) than those not using NSAIDs (12%) | Univariable analysis | (–) | |
|
| |||||||
| Bijsterbosch [ | 6 | LOW | Poor outcome not fulfilling PASS for AUSCAN (>8.2, 16.1) | RR (95% CI) ∞ | Multivariable: baseline scores of the clinical outcome measure, follow-up time, family effects | (+) | |
| Siviero [ | 1.5 | LOW | MCID score of >4 AUSCAN function | RR (95% CI) pain score ≥5 1.11 (0.89, 1.37) | Multivariable: sex, age, country, education level | (o) | |
| Vanhaverbeke [46] | 9.7 | HIGH | AUSCAN function (0–90), change ≥ 7.2 or | OR (95% CI) VAS >33mm 1(0.34, 2.94) | Univariable analysis | (o) pain | |
| Courties [ | 2.6 | HIGH | Deterioration from baseline scores AUSCAN/FIHOA | OR (95% CI) 0.956 (0.88, 1.038) | Multivariable: no adjustment, FIHOA, CHD and depression | (o) | |
| Neuprez [ | 2 | HIGH | AUSCAN (0–300) change > MCID 15, | OR (95% CI) AUCAN score <74.5 1.02 (1.01,1.03) | Multivariable analysis | (+) | |
|
| |||||||
|
| Bijsterbosch [ | 6 | LOW | Poor outcome not fulfilling PASS for AUSCAN (>8.2, 16.1) | RR (95% CI) ∞ | Multivariable: baseline scores of the clinical outcome measure, follow-up time, family effects | (o) |
| Courties [ | 2.6 | HIGH | Deterioration from baseline scores FIHOA | radiographic scores OR (95% CI) 0.99 (0.97, 1.01) p 0.24 | Univariable analysis | (o) | |
| Neuprez [ | 2 | HIGH | AUSCAN (0 | Not statistically significant, estimate not provided. | Multivariable analysis | (o) | |
| Van Beest [ | 2 | HIGH | increased thumb base pain on palpation (0–3) | (osteophytes) | Multivariable analysis adjustments for other imaging scores. | (o) | |
| Vanhaverbeke [ | 9.7 | HIGH | AUSCAN function (0–90), change ≥ 7.2 or | OR (95% CI) Function total R joints 1.06 (0.85,1.32) | Univariable analysis | (o) | |
| Neuprez [ | 2 | HIGH | AUSCAN (0–300) change > MCID 15, | OR (95% CI) ∞ | Multivariable analysis | (+) | |
|
| |||||||
|
| Bijsterbosch [ | 6 | LOW | Poor outcome not fulfilling PASS for AUSCAN (>8.2, 16.1) | RR (95% CI) Poor outcome pain >8: 2.11 (1.25, 3.08) | Multivariable: baseline scores of the clinical outcome measure, follow-up time, family effects | (+) |
| Neuprez [ | 2 | HIGH | AUSCAN (0–300) change > MCID 15, | Not statistically significant, estimate not provided. | Multivariable analysis | (o) | |
| Bijsterbosch [ | 6 | LOW | Poor outcome not fulfilling PASS for AUSCAN (>8.2, 16.1) | RR (95% CI) ∞ | Multivariable: baseline scores of the clinical outcome measure, follow-up time, family effects | (o) | |
| Neuprez [ | 2 | HIGH | AUSCAN (0–300) change > MCID 15, | Not statistically significant, estimate not provided. | Multivariable analysis | (o) | |
|
| Vanhaverbeke 2020 [ | 9.7 | HIGH | AUSCAN function (0–90), change ≥ 7.2 or | OR (95% CI) 0.9 (0.9,1.06) | Univariable analysis | (o) |
| Siviero [ | 1.5 | LOW | MCID score of >4 AUSCAN function | RR (95% CI) Grip [ref >35kg] | Multivariable: sex, age, country, education level | (+) | |
|
| |||||||
|
| Dieppe [ | 8 | HIGH | patient reported outcomes and overall condition (better, same, worse) | Descriptive data (chi squared and significance at 5% level) NS | Univariable analysis | (o) |
| Courties [ | 2.6 | HIGH | Deterioration from baseline scores AUSCAN/FIHOA | OR (95% CI) 1.1 (0.64,1.9) | Univariable analysis | (o) | |
| Neuprez [ | 2 | HIGH | AUSCAN (0–300) change > MCID 15, | Not statistically significant, estimate not provided. | Multivariable analysis | (o) | |
|
| Courties [ | 2.6 | HIGH | Deterioration from baseline scores AUSCAN/FIHOA | OR (95% CI) 2.91 (1.02,8.26) | Multivariable: not specified which adjustments were made. | (+)* |
| Siviero [ | 1.5 | LOW | MCID score of >4 AUSCAN function. | RR (95% CI) 1.05 (0.88,1.25) | Multivariable: sex, age, country, education level | (o) | |
| Scherzer [ | 12 | HIGH | Transitions from AUSCAN pain categories ≤6 ‘low’ or AUSCAN >6 ‘high’ | HR (95% CI) 0.99 (0.63,1.55) | Multivariable: age, sex, race, education level, BMI, symptomatic KOA, NSAID use | (o) | |
| Neuprez [ | 2 | HIGH | AUSCAN (0–300) change > MCID 15, | Not statistically significant, estimate not provided. | Multivariable analysis | (o) | |
|
| Courties [ | 2.6 | HIGH | Deterioration from baseline scores AUSCAN/FIHOA | OR (95% CI) 0.84 (0.35,2.01) | Univariable analysis | (o) |
| Scherzer [ | 12 | HIGH | Transitions in AUSCAN pain categories ≤6 ‘low’ or AUSCAN >6 ‘high’ | No. with diabetes/number without, HR (95% CI) worsening AUSCAN pain: | Multivariable: age, sex, race, education level, BMI, symptomatic KOA, NSAID use | (+) | |
| Siviero [ | 1.5 | LOW | MCID score of >4 AUSCAN function. | Adj RR (95% CI) 0.86 (0.65,1.12) | Multivariable: sex, age, country, education level | (o) | |
| Neuprez [ | 2 | HIGH | AUSCAN (0–300) change > MCID 15, | Not statistically significant, estimate not provided. | Multivariable analysis | (o) | |
|
| |||||||
|
| Siviero [ | 1.5 | LOW | MCID score of >4 AUSCAN function | RR (95% CI) | Multivariable: sex, age, country, education level | (o) |
| Courties [ | 2.6 | HIGH | Deterioration from baseline scores AUSCAN/FIHOA | OR (95% CI) 0.44 (0.18,1.05) | Univariate analysis | (o) | |
| Neuprez [ | 2 | HIGH | AUSCAN (0–300) change > MCID 15, | Not statistically significant, estimate not provided. | Multivariable analysis | (o) | |
- —University Hospitals of Derby & Burton NHS Foundation Trust, Pump Prime Grant Scheme
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOrthopedic Surgery and Rehabilitation · Osteoarthritis Treatment and Mechanisms · Shoulder Injury and Treatment
Introduction
Osteoarthritis (OA) is common and frequently affects the hands, with a population prevalence estimate of 42% (radiographic hand OA), which is higher than estimates for the knees (24%) and hips (11%) [1]. Hand OA is often painful and has significant functional and psychological impacts, such as loss of independence or inability to perform a caring role, and can result in early retirement [2]. Hand OA can be divided into different subsets depending on the joints affected: nodal OA, thumb base OA (TBOA), and erosive hand OA [3]. These subsets are described in more detail elsewhere, but essentially the presence of Bouchard and Heberden nodes on the proximal and distal interphalangeal joints of the hand defines nodal OA; thumb base OA is defined as OA in the first carpometacarpal joint and can include the scaphotrapezial trapezoid joint; erosive OA is characterised radiographically by central erosions and collapse of the subchondral bone, and is most commonly seen in the distal interphalangeal joints [4,5].
A previous systematic review on the course of hand OA conducted ten years ago [6] concluded that the literature at that time was predominantly concerned with radiographic progression; further research is needed to understand both the clinical progression of hand OA and the factors associated with poor long-term outcomes. This review intends to focus on TBOA, which is the most common subset of hand OA and frequently occurs in isolation [7]. Patients with TBOA complain of severe pain and difficulty completing everyday essential tasks because of the thumb’s unique role in providing opposition for pinch and dexterity. They feel it is important to know the course of their condition, as they fear losing the use of their hands. Treatment for hand and TBOA includes pharmacological, non-pharmacological and surgical options, and should be tailored to the individual [8]. Non-pharmacological multi-modal treatments are recommended as a first step including education to support self-management, ergonomic task modification, exercises to improve movement, proprioception and strength, and hand splints [8,9].
Understanding the disease course and prognostic indicators is essential for clinicians managing chronic conditions. For example, it has informed models of stratified care and enhanced treatments for those at risk of persistent low back pain [10]. Stratified or personalized care is endorsed by expert working groups as ideal for OA, where the disease course varies [11] and is especially important in conditions with a high prevalence to ensure treatment is targeted at those who need it [12].
Radiographic progression of existing TBOA occurs in 64–71% of patients over 9 years [13]. Visible deformity and significant loss of strength, movement, and hand function are observed in patients with TBOA compared to healthy controls [14,15]. However, weak associations have been reported between the severity of radiographic hand OA and patient-reported measures of pain and function over time [16], indicating that other factors may explain the variation in pain and function outcomes [17]. TBOA is considered more biomechanically driven than finger OA; thus, progression and risk factors may differ [18,19]. Therefore, the aim of this systematic review was to summarize and critically appraise evidence regarding the course and prognosis of symptomatic TBOA, (rather than all subsets of hand OA). Anticipating only a few cohort studies where the prognostic factors for TBOA have been assessed separately from the hand, it is important to consider all research on the course and prognostic factors for hand OA that includes all subtypes (TBOA, nodal and erosive) and, where possible, separate the review evidence that is specific to the thumb base. Therefore, the proposed systematic review considers the following questions.
- What is the course of pain and functional difficulties in patients with hand OA and TBOA over time?
- What are the potential prognostic factors associated with pain and function identified in the literature for hand OA and TBOA?
Methods
The review protocol is registered in the PROSPERO database (CRD42020196725). It has been reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [20].
Search strategy
The search used keywords and subject-indexed search terms related to the domains of diagnosis (OA), hand, and study design (cohort/prognosis) applicable to each database. The full strategy for the databases searched are presented in Supplementary Tables 1.1 − 1.6.
The following databases were searched on April 13, 2023,: MEDLINE (1946–present), AMED (1995–present), EMBASE (1947–present), PsycINFO (1806–present), CINAHL via EBSCO (1937–present), and AgeLine (1978–present). Web-based repositories producing evidence syntheses were also searched using the same keywords in the title or abstract: SIGN, NICE, the TRIP database, and Epistemonikos. Web of Science core databases were searched to identify any further key articles that were not included in the main search. The search was supplemented by a bibliographic screening of relevant systematic reviews identified by the searches.
Selection criteria
This review included longitudinal studies of adults with a diagnosis of hand OA (including all subtypes) or specifically thumb base OA, where measures of pain and function were collected at a minimum of two time points, at least 12 months apart. Outcomes were examined over the short term (follow-up duration, 12 months to 3 years) and longer term (>3 years). A complete list of the selection criteria is presented in Table 1.
Study selection
After the removal of duplicates, titles, abstracts, and full texts were uploaded to Rayyan [21]. Using a pre-specified checklist studies were screened separately by two reviewers (VJ and JG). Any disagreements regarding the inclusion of studies at both stages were discussed and resolved by a third person (MM).
Data extraction and management
Data were independently extracted by two reviewers (JG and VJ) and verified by a third reviewer (AS) using a bespoke data extraction form. Disagreements were resolved through discussion and consensus among the three reviewers. The data extracted were cohort, country, study setting, population characteristics (age and sex), diagnostic OA criteria used, proportions meeting the criteria, follow-up duration, retention rate, outcome measures (for symptomatic course e.g. hand pain, and function), results, definitions and amount of progression, risk factors, and estimates of their association with pain and function.
Methodological quality
Methodological quality was assessed by two reviewers (VJ and AS) using the Quality In Prognostic Studies (QUIPS) tool [22]. The QUIPS tool assesses the validity and risk of bias over six domains (participation, attrition, prognostic factor assessment, outcome measurement, confounding factors, statistical analysis, and reporting) to evaluate the overall risk of bias (ROB). Judgements of the overall risk of bias for a study were made as follows: if all domains were classified as low risk, or up to one moderate risk, then this paper was classified as low risk of bias; if one or more domains were classified as high risk, or more than three moderate risk, then this paper was classified as having a high risk of bias [23]. On the prompting items relating to ‘participation and attrition’, cut-offs were used to ensure consistency, with at least 67% for both participation and retention rates considered acceptable [23].
Evidence synthesis
The following analyses were planned: (1) analysis to pool estimates of change in pain function and any secondary outcomes such as grip strength over time, and to estimate the strength of association between a change in symptoms and individual prognostic factors; (2) An assessment of publication bias using funnel plots to look for bias from ‘small-study effects’; (3) A best evidence narrative synthesis to describe the overall prognosis (outcomes with hand OA) and the value of prognostic indicators for outcome. The latter was conducted using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) method, modified for prognosis research [24], using the recommended four factors that might lessen confidence in the evidence: risk of bias, inconsistency, indirectness, and imprecision [24–26]. Studies were grouped for synthesis by follow-up length and outcome measured. The study inclusion criteria purposely allowed a broad range of hand OA patients (recruited from a range of settings, with differing diagnostic criteria) to make the results generalizable to all hand and thumb base OA patients, which narrowed our definition of indirectness (Supplementary Table 2). Therefore, indirectness was considered and excluded (as not applicable) as a reason for downgrading the prognostic factor evidence in this review.
Results
The search strategy identified 13,352 articles. The systematic reviews retrieved were not included in data analysis, but screened for references and one additional study was added. After removal of duplicates 9523 article remained and the titles and abstracts were screened. This resulted in the exclusion of 9425 articles, and 98 were retained for full-text review where a further 74 articles were excluded. Common reasons for exclusion on full-text review were articles published solely as conference abstracts (n = 25), studies of OA in which hand data were not presented separately (n = 12), cross-sectional studies (n = 9), duplicate studies (n = 10), and studies providing only baseline outcome data on pain and function (n = 6), or follow-up data were exclusively radiographic) (n = 9). In total, 24 studies met the selection criteria and were included in the systematic review (Figure 1).
Flowchart of study selection process.
Study characteristics
The 24 studies included came from 13 different cohorts, and their characteristics are presented in Table 2. Where data from the same cohorts were reported, this was mostly concerned with data from different follow-up time points. Exceptions to this were studies that reported changes in joint-level symptoms versus person-level data for the course of disease or course of disease versus prognostic factor analysis [16,27–29]. The studies were conducted in Europe and the USA with follow-up periods ranged from 1 to 12 years. All studies were prospective observational cohorts, except for one placebo group in a randomized controlled trial of interventions for knee OA [30].
Participants
The total number of participants included in the 13 cohorts was n = 8,699 [7,28–39], with sample sizes ranging between 91 [40] and 2942 [40] (Table 2). The average age of the samples ranged from 54.5 to 73.7 years [36,37], with predominantly female populations of 52 to 100% [36,37]. Participants were recruited from the community [7,31,35,37,41,42], from those attending primary [39,43], secondary [16,27–29,31,33,40,44,45] and tertiary [32,46] healthcare settings, and in one study from teachers’ and dentists’ professional associations [36]. Four cohorts used clinical criteria to determine a diagnosis using the American College of Rheumatology (ACR) [47] or clinician-diagnosed hand OA [28,29,33,37]. Four studies used specified radiographic criteria alone [30,31,35,36], and five used a combination of the ACR criteria or specified clinical signs and radiographic criteria [7,34,38,39,46].
When considering the different subgroups of hand OA, most cohorts did not report any data on the different subgroups of hand OA, three studies provided data on the proportion of a subtype in the study population [38,39,48] and one study provided outcome data separated by the different subtypes [7]. One cohort included exclusively people with TBOA [33,40], one study presented only the data for those with TBOA who had a magnetic resonance imaging (MRI) scan [49] and two hand OA studies presented separate data for those with TBOA [7,39].
Methodological quality
Five studies (24%) had an overall low risk of bias [7,27,28,37,39] the majority (n = 15, 71%) were rated as having an overall high risk of bias (Table 3). The domain most considered to have a high risk of bias was the confounding factor domain (n = 11), where confounding factors were not measured [33,35,40], well described [29,30,34,36,41,43,44,46] or accounted for in the study design or analysis [36,43]. Four studies without any domains scored as having a high risk of bias had a moderate risk of bias in three domains, giving them an overall high risk of bias [31,38,45,49].
Publication bias
Publications were assessed to confirm that the data presented were complete, as described in the methods section of the publication. The number of studies reporting the same outcome or assessing the same prognostic factor was too small to allow a more formal analysis of reporting bias using funnel plots [50].
Measures of hand pain and function
The Australian Canadian Hand OA Index (AUSCAN) was the most commonly used measure to assess pain and function [51]. The AUSCAN pain and function subscales were reported in 15 studies [7,16,27,29,32,33,37–43,46,49] (Table 2). The severity of pain on palpation of individual joints was reported in six studies [16,27,39,44,45,49]. Pain intensity was assessed using the Visual analogue scale VAS (0–100 mm) in five studies [27,32,38,46,49]. Patient-rated wrist and hand evaluation (PRWHE) for pain and function [52] was used in two studies from the same cohort [33,40]. The functional Index for Hand OA (FIHOA) [53] was collected in five studies [28,30,32,45,46]. Grip strength was measured in six studies [16,27,31,32,35,37] using various definitions and methods of reporting results. Pinch strength was reported in only one study [31].
The data presented for all measures of hand pain and function varied widely. For example, with patient-rated outcome measures, some studies used total scores, others subscale scores, some presented change scores rather than follow-up scores, and some categorized data such as those who had improved, remained stable, or deteriorated. For those studies that grouped participants into categories of improving, stable, or worsening, the way in which this was done also varied as follows: a patient global rating of change question [34,41]; a change in the number of symptomatic joints [29]; the change from baseline regardless of magnitude [30]; a change from baseline score that exceeded the minimum clinically important difference for the patient-rated outcome measure [16,28,37,39,46]; and grouping patients as low or high pain or function and describing the proportions who transitioned between groups during follow up [42].
Clinical course of hand pain
Twelve studies reported the course of hand pain at the person level over time [7,16,29,32–34,38–40,43,44,46] (Table 4). The data were unsuitable for meta-analysis owing to variability in the outcome measures used, the way data were presented, length of follow-up, and heterogeneity in terms of study setting and participants. When considering the course of hand OA pain, six studies showed average reductions in hand pain [32,33,38,40,44,46] and an equal number of average increases in hand pain [7,16,29,34,39,43]. The average change over time reported in most studies was small, despite the time frame examined [32,44,46]. For example, the mean deterioration in the AUSCAN pain subscale score was reported as 1.0 (SD 4.0, 95% CI 0.4 − 1.6) on a 0 to 20 scale over 3 years [43] and another study reported 0.7 (95% CI 0.3–1.2) [39] over four to seven years (Table 4). Two studies presented the proportions of participants with improvements or deterioration in pain scores, over two years 25% had deteriorated [38], over seven years 29% had deteriorated and 21% had improved [16]. The global rating of change for hand pain and stiffness was assessed, with 49% reporting worse symptoms after four years [31]. One study [41] assessed changes in ‘hand problem’ rather than hand pain and found that 56% of participants had a worsening problem over seven years. Another study [34] assessed the change in hand pain with a change in the overall condition, finding deterioration in similar proportions at three (48%) and eight years (54%).
Only four studies assessed thumb base OA as a separate phenotype. Two studies from the same cohort of clinically diagnosed early thumb base OA suggested that, on average, hand pain was reduced by small amounts. AUSCAN Scores on 0–20 scale were reduced from 6.6 (4.1) to 6.4 (4.0) over both 18 months [33] and three years [40] with large standard deviations and a wide range in pain scores (Table 4). Another study with small mean changes in pain in hand OA stated that over six years pain scores remained above the patient’s acceptable symptom state in 54.4% of those with clinical and radiographic thumb base OA [39]. A final study reported on the presence or absence of pain in thumb base OA over two years, pain decreased in 16%, remained stable in the majority (73%), and worsened in 11% [49].
Five studies reported on the course of hand pain at the joint level. A study found that 65% of the joints with pain at baseline had reduced pain at two years and 16% of the joints had increased pain [27]. Over eight years 23% reported improvement, and 54% had worsened pain in an index hand joint [29,46]. Two studies found that on average over seven to ten years the severity of pain did not change [29,46] and the number of painful joints reduced from an average of 3.1 (SD 3.4) to 2.3 (SD 3.5) (p = 0.035) but the number of swollen joints increased from an average of 1.4 (SD 1.8) to 3.6 (SD 2.9) (p < 0.001) [46]. A third study found that 31% of participants experienced symptoms in additional joints (s) over 12 years, with little change in the overall number of symptomatic joints (median, IQR) 0(0–1) [48].
The GRADE assessment of 11 prospective studies with 3051 participants found low and very low-level evidence for an average change in hand pain over both the short and long term (Table 5). The evidence was downgraded as most of the studies had a high risk of bias, inconsistency between studies for the direction of mean pain changes, the short-term studies also had small sample sizes, and the longer-duration studies had different approaches to reporting pain scores.
Clinical course of function in hand OA
Thirteen studies reported changes in function at the person-level over time [7,16,28–30,32,33,37–40,43–46], with variations in the magnitude of change (Table 4). Heterogeneity between studies precluded meta-analysis of the results. Over the short term (up to three years), three studies showed average improvements in function [30,33,40], and five deterioration [7,28,38,43,45]. The reported magnitude of the change in the short term varied from small mean change scores [7,43] for example, AUSCAN function mean change on a 0–36 scale 1.4 (6.1) [7,43] to larger mean changes of 5.6 (3.6) and for FIHOA mean change on a 0–30 scale of 3.7 (2.6) [28]; (increased scores represent a deterioration). Estimates from four studies for proportions of participants with deterioration in function in less than three years ranged from 23–42% [28,30,37,38], with functional improvement in 24% [37]. Over four to ten years of follow-up, the estimates for the proportions with deterioration in function were between 47 and 59% [16,46], and improvements were seen in 32% [16] of the participants.
The GRADE assessment found low-level evidence of small changes in hand function in the short term. This included nine prospective studies with 6179 participants, the level of evidence was downgraded due to the number of studies at high risk of bias and inconsistency due to different: directions of change; outcome measures; and reporting of outcome data. Moderate-level evidence for small changes in hand function over long-term follow-up was found in five studies with 1296 participants. Three studies had a high risk of bias, leading to downgrading in one domain. These studies demonstrated an average worsening function score in most patients with hand OA (Table 5).
Baseline and follow-up grip strength scores were reported in five studies [16,31,32,35,46] (Table 4). These demonstrated that small changes in grip strength occurred, in one study over four years mean change grip right −0.4 kg (SD 15.4), left 0.4 kg (SD 16.3) [31], with greater reductions in grip strength over time (at seven years mean change −0.7 kg (SD 6.9) in right, and −1.1 kg in the left hand (SD 6.9) [16] and over ten years mean change from a baseline score of 19.0 kg (SD 9.0) to 15.8 kg (SD 8.0)) [32] at follow-up.
On GRADE assessment of the five prospective studies with 1893 participants, a moderate level of evidence was found for small mean reductions in grip strength with a trend for greater deterioration over longer time periods (Table 5). Three studies had a high risk of bias, which led to a downgrading in a single domain.
Candidate prognostic factors
Twelve studies assessed 46 potential prognostic factors, which were grouped under the following six headings: demographic and social characteristics, symptom severity, clinical signs, investigations, comorbidities, and psychological factors (Supplementary Table 3). Eighteen prognostic factors were assessed in at least two studies (Table 6). The factors that were reported to have an association with deteriorating pain or function in any study were as follows: disease duration of greater than 5 years [34]; high hand load for leisure [36]; low baseline grip strength [37]; high baseline level of pain and functional difficulty [38,39,46]; a greater number of painful hand joints [39] or erosive hand joints [38], a single comorbidity of heart disease [30] or diabetes [42] multiple co-morbidities [42], certain illness perceptions [28] and the use of certain coping strategies [45]. Additionally, some studies identified prognostic factors for different outcomes, including ethnicity with an increase in the number of symptomatic joints [48], and the presence of coexisting knee OA [34] to worsening global assessment of OA. Lack of deterioration was associated in single studies with older age at the onset of osteoarthritis [46] and the use of non-steroidal anti-inflammatory medications [34].
The GRADE assessment found that the prognosis of persistent or worsening pain and worsening function conclusions were limited by having only single studies for a given factor (providing only exploratory evidence for their value as a prognostic factor). Where prognostic factors were assessed in multiple studies, there was variation in the direction of the effects, follow-up periods, outcome assessments, data analysis, and data presentation. These factors affected the consistency and precision of the judgements. Finally, most judgements were downgraded for quality because most studies had a high risk of bias. Moderate-level evidence of persistent or worsening hand pain was found for the presence of diabetes as a prognostic factor. Low-level evidence was found for the following prognostic factors: self-reported baseline pain, self-reported baseline function, age, and number of painful hand joints. For the outcome of worsening hand function moderate level evidence was found for the prognostic factor of self-reported pain, and low-level evidence for the prognostic factors of: self-reported function; number of painful hand joints; number of erosive hand joints; grip strength; presence of coronary heart disease; income; and certain illness perceptions (Table 6; Supplementary Table 4).
Discussion
This review summarizes and critically appraises evidence regarding the course and prognosis of symptomatic hand OA including subtypes of TBOA, nodal OA, and erosive OA). Evidence from this review suggests that individuals with hand OA experience different symptom courses, ranging from improvement to deterioration. On average, there is little change in the hand pain experienced over both short and long time periods, and hand function and grip strength do deteriorate, but, on average, by small amounts. Forty-six prognostic factors of persistent or worsening hand pain and worsening hand function have been examined, but the majority have only been investigated in a single study or where replicated studies show contradictory results. However, our evidence indicates that deterioration in hand pain and function is associated with diabetes and baseline pain severity, respectively.
The different symptom courses of hand and thumb pain are evidenced by the varying proportions of individuals whose pain worsened and those whose pain improved in nine different studies, but also by the wide standard deviations around the mean for baseline, follow-up, and change scores. There is no certainty regarding the estimates for the proportions with worsening pain over the short and long term due to variations in the outcome measures used and different definitions of worsening hand pain. Additionally, the outcome of pain in hand OA can be assessed in different ways, which do not necessarily correlate, but are each valid. For example, the number of tender joints on palpation may be affected by inflammation, but it cannot be used interchangeably with patient reported pain severity. The latter may relate more to central pain sensitization, as well as coping skills and illness perception [54].
In comparison, moderate evidence was found for changes in hand function over the longer term, which, on average, deteriorated by a small amount. Again, the evidence from the studies suggests that this was variable among individuals, with approximately 50% who experienced deterioration. There was also moderate evidence that grip strength deteriorated over time, and the greater the length of time, the greater the deterioration that was observed. Aging could explain some of this change [55], but in this review, it was not possible to consider strength relative to expected age-related norms. However, grip strength in hand OA is reduced early in the radiographic disease course [56] and may be most affected in TBOA [56–58]. In this review, the four-to-seven-year average changes in grip strength did not meet the 0.84–1.12 kg minimum clinically important difference [59] but over 10 years the deterioration exceeded this and would impact on an individual’s hand function [60], suggesting that strengthening grip could be an important longer-term treatment target, especially in early onset hand and TBOA.
Few studies have examined TBOA separately from hand OA. Two low-quality studies were found in one cohort assessing TBOA [33,40], but the data at baseline represented only those with early radiographic disease and excluded those who underwent surgery during follow-up. It is uncertain whether the improved symptomatic course observed in these studies may be representative of TBOA in general. Another study assessed changes in pain on thumb base palpation, finding over two years that 16% improved and 11% worsened [49], if pain on palpation corresponded to the pain levels experienced, then the proportions might suggest that fewer participants experience worsening of their TBOA pain than with hand OA (25%) [38]. However, two studies presented data for hand OA subsets separately; one community population found no significant differences between the subsets for hand pain and function at 3-years adjusted for baseline [7], while the other found that TBOA was associated with a reduction in grip strength over time [16], suggesting that TBOA impacts not only pinch and dextrous tasks but also whole hand grip strength more than other subgroups. While this review is interested in progression, it is important to point out that even with little progression, studies suggest that pain levels can be high for some individuals and remain high over time. One study found that 54.4% of patients with clinical and radiographic TBOA had symptoms above the patient acceptable symptom state [39].
To date, only one systematic review has examined the prognostic factors for progression of hand OA [6]. This study adds to the previous systematic review by summarizing the data from more recent studies and is focused specifically on the course of symptoms and associated prognostic factors. As with the previous literature, most of the studies can be viewed as exploratory studies that identify new and promising factors, which require further confirmatory research. Four studies were judged by the reviewers as confirmatory studies [28,29,42,45], which examined the added prognostic value of an identified factor after adjusting for established, prognostic factors [61]. From a broad range of factors assessed, this review identified low evidence for a relationship between deteriorating hand pain or hand function and five prognostic factors (baseline function, negative illness perceptions, the number of painful hand joints, number of erosive hand joints, and the presence coronary heart disease). Two prognostic factors were assessed as having a moderate level of evidence: diabetes for persistent or worsening hand pain, and high levels of baseline hand pain as prognostic factors for poor functional outcome. However, all studies assessing both factors differed in the direction of the effect of this relationship. The different analytical techniques and assumptions used are a possible cause for this inconsistency, for example, the use of an unadjusted model in one study and a very different cut-off point for high baseline level of hand pain in all studies.
A better understanding of the characteristics that indicate which patients will deteriorate or will not respond to current treatment could be used to improve pathways of care and develop new treatments targeting modifiable prognostic factors. Passive coping strategies and negative illness perceptions are potentially modifiable and are not current treatment targets for hand and TBOA. Self-reported pain severity is known to be strongly related to psychological factors [62], suggesting that new treatments could be considered to improve pain coping skills and illness perceptions.
Limitations
This systematic review had several limitations. There was large heterogeneity in the data studied; hence, this review provides the best evidence narrative summary, rather than a pooled summary estimate meta-analysis. Future studies would benefit from describing their populations by hand OA subtype, and assessing outcomes according to subtype, as the differing subtypes may have differing symptomatic course and prognostic factors. Additionally, future research would benefit from an agreed definition of worsening or improving symptoms, a consistent approach to presenting outcome data, and a standardized length of follow-up for short- and long-term studies. Additionally, the quality of prognostic factor studies could be improved by collecting and providing data on study participation (source population and adequate participation by eligible individuals) and confounding factors (details on the factors assessed, their measurement method, and how they have been accounted for in the analysis). This review intentionally included a broad spectrum of hand OA in terms of the diagnostic criteria used and the setting of the research. This means that all levels of severity of condition are included, but this could be considered a limitation, as the stage of advancement at baseline or severity of symptoms may impact the symptomatic course.
Future research and clinical implications
This review suggests that the course of symptoms in hand and TBOA is variable between individuals. Further research is required into the prognostic factors that might indicate those at risk of persistent pain and poor function as this review found either limited evidence or contradictory results.
This review demonstrates that grip strength and hand function in people with hand and thumb base OA does deteriorate by small but increasing amounts over time. It would be important to consider this as a potential target for interventions and when looking at longer-term results of interventions, e.g. over three years. Halting deterioration by maintaining strength and hand function should be seen as a positive outcome, alongside any gains achieved.
Results from two randomized controlled trials [63,64], suggest the outcome of non-operative care is also variable. Prognostic factors for the outcomes of symptom course and response to treatment may overlap. The prognostic factors identified from this review for symptom course should also be explored as potential predictors of treatment effect, which will require analysis of evidence from randomised trials of intervention for hand OA.
Conclusion
This review summarizes and critically appraises evidence regarding the course and prognosis of symptomatic hand OA and thumb base OA. Evidence from this review suggests that, on average, there is little change in the hand pain experienced with hand OA over both short and long periods, whereas hand function and grip strength do deteriorate but, on average, by small amounts. There is evidence to suggest that there are differing symptom courses in hand OA, but there is limited or contradictory evidence of prognostic factors that might indicate a worsening trajectory. Prognostic factors that may indicate a higher likelihood of increasing hand pain and worsening hand function are related to general health, psychological factors, and perceived severity of symptoms. Further research is needed to confirm the predictive performance of these factors and broaden our understanding of the prognostic factors for worsening pain in hand and thumb base OA.
Supplementary Material
Supplemental Material
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Pereira D, Peleteiro B, Araújo J, et al. The effect of osteoarthritis definition on prevalence and incidence estimates: a systematic review. Osteoarthritis Cartilage. 2011;19(11):1270–1285. doi: 10.1016/j.joca.2011.08.009.21907813 · doi ↗ · pubmed ↗
- 2Hill S, Dziedzic KS, Ong BN. The functional and psychological impact of hand osteoarthritis. Chronic Illn. 2010;6(2):101–110. doi: 10.1177/1742395309345614.20444766 · doi ↗ · pubmed ↗
- 3Zhang W, Doherty M, Leeb BF, et al. EULAR evidence-based recommendations for the diagnosis of hand osteoarthritis: report of a task force of ESCISIT. Ann Rheum Dis. 2009;68(1):8–17. doi: 10.1136/ard.2007.084772.18250111 · doi ↗ · pubmed ↗
- 4Kloppenburg M, Kwok W-Y. Hand osteoarthritis – a heterogeneous disorder. Nat Rev Rheumatol. 2011;8(1):22–31. doi: 10.1038/nrrheum.2011.170.22105244 · doi ↗ · pubmed ↗
- 5Marshall M, Watt FE, Vincent TL, et al. Hand osteoarthritis: clinical phenotypes, molecular mechanisms and disease management. Nat Rev Rheumatol. 2018;14(11):641–656. doi: 10.1038/s 41584-018-0095-4.30305701 · doi ↗ · pubmed ↗
- 6Kwok WY, Plevier JWM, Rosendaal FR, et al. Risk factors for progression in hand osteoarthritis: a systematic review. Arthritis Care Res (Hoboken). 2013;65(4):552–562. doi: 10.1002/acr.21851.22972764 · doi ↗ · pubmed ↗
- 7Marshall M, Peat G, Nicholls E, et al. Subsets of symptomatic hand osteoarthritis in community-dwelling older adults in the United Kingdom: prevalence, inter-relationships, risk factor profiles and clinical characteristics at baseline and 3-years. Osteoarthritis Cartilage. 2013;21(11):1674–1684. doi: 10.1016/j.joca.2013.08.004.23954700 PMC 3819994 · doi ↗ · pubmed ↗
- 8Kloppenburg M, Kroon FP, Blanco FJ, et al. 2018 update of the EULAR recommendations for the management of hand osteoarthritis. Ann Rheum Dis. 2019;78(1):16–24. doi: 10.1136/annrheumdis-2018-213826.30154087 · doi ↗ · pubmed ↗