Integrated diagnosis and treatment: Endoscopic retrograde direct cholangioscopy addressed the challenges of type III perforations
Shan-Shan Hu, Xiao-Gang Liu, Yun-Chao Yang, Jie Hou, Wei-Hui Liu

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
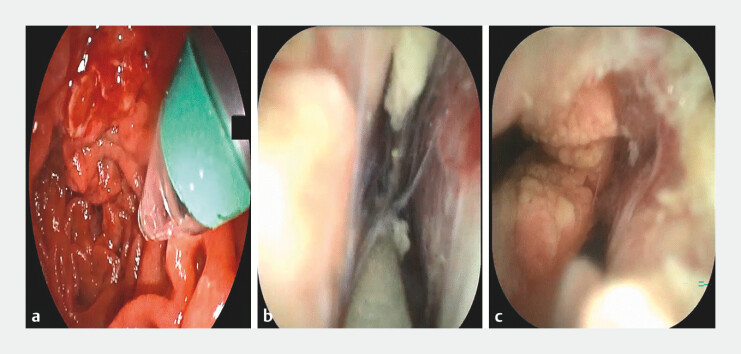 Fig. 1
Fig. 1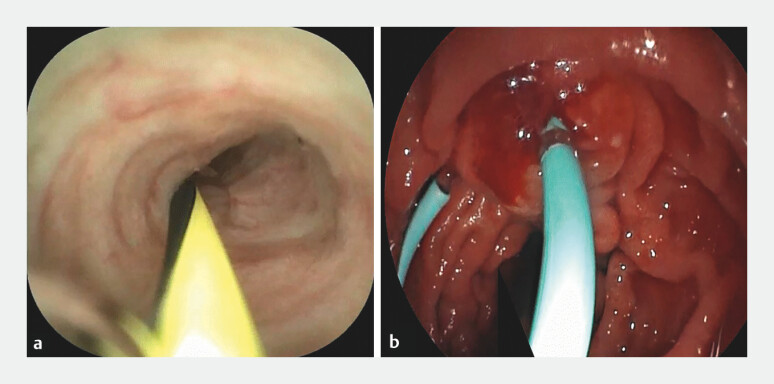 Fig. 2
Fig. 2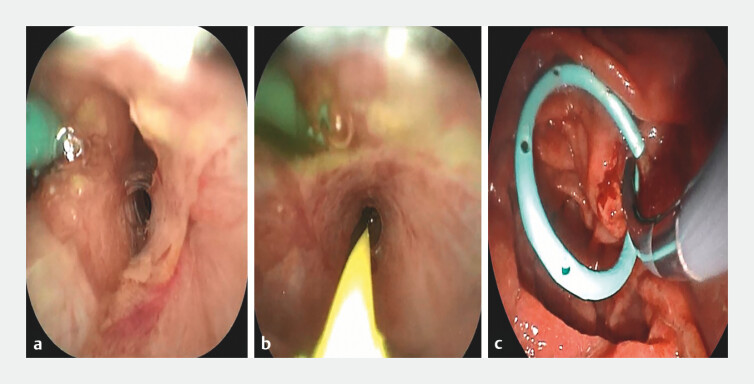 Fig. 3
Fig. 3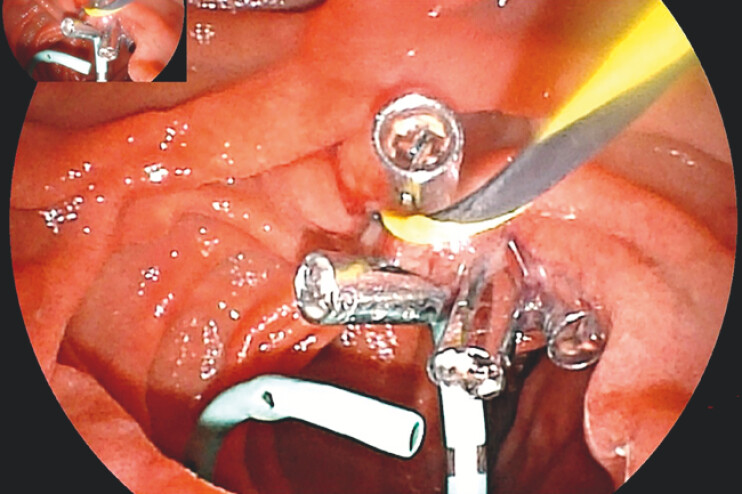 Fig. 4
Fig. 4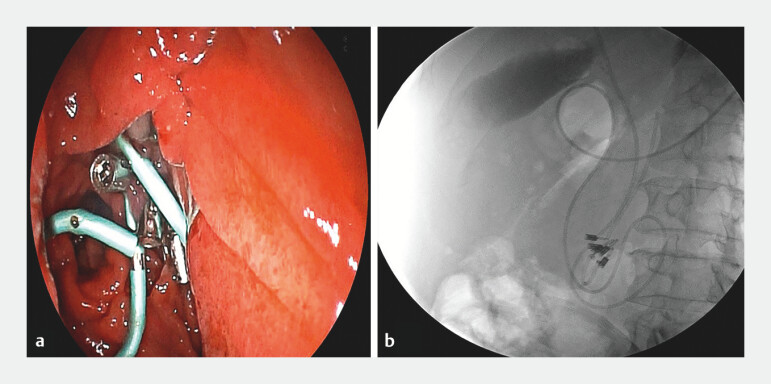 Fig. 5
Fig. 5- —The Science & Technology Department of Sichuan Province
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGallbladder and Bile Duct Disorders · Esophageal and GI Pathology · Biliary and Gastrointestinal Fistulas
The complication of endoscopic retrograde cholangiopancreatography (ERCP)-related perforation (EP) has increasingly drawn clinical concern 1 . According to the Stapfer classification criteria, there exists a diagnostic and therapeutic dilemma for Type III perforations 2 3 . This report introduces a novel endoscopic retrograde direct cholangioscopy (ERDC) technique developed by our team 4 5 and demonstrates its technology as an effective method for the early diagnosis and treatment of Type III ERCP-related perforations.
A patient was scheduled to undergo ERCP. During intubation, the guidewire exhibited abnormal morphology. To facilitate early detection of EP, direct intubation was performed using ERDC-assisted ductal cannulation. This approach allowed for direct visualization, revealing that the guidewire had entered the peritoneal cavity and identifying ruptures in both the bile duct and pancreatic duct caused by the instrumentation ( Fig. 1 ). Using ERDC, we successfully guided the guidewire through the pancreatic duct rupture and placed a pancreatic duct stent ( Fig. 2 ). Similarly, ERDC facilitated identification of the compressed and obstructed bile duct orifice, allowing for smooth guidewire insertion. Upon further manipulation of the choledochoscope, the common bile duct was found to be narrow and slender, necessitating bougie dilation ( Fig. 3 ). Subsequently, endoscopic suturing technology was employed to close a suspected perforation near the duodenal papilla ( Fig. 4 ). Finally, a drainage tube was inserted along the guidewire into the common bile duct for effective drainage ( Fig. 5 ). Postoperatively, the patient experienced no discomfort, and abdominal computed tomography revealed no evidence of pneumoperitoneum or fluid accumulation ( Video 1 ).
ERDC visualization of Type III EP: a Conical transparent cap mounted on the choledochoscope tip; b Guidewire visibly entering the abdominal cavity; c Identification of ruptures in the bile and pancreatic ducts. Abbreviation: EP, ERCP-related perforation.
Super-selective pancreatic duct cannulation and stent placement: a Guidewire placement in the pancreatic duct under ERDC guidance; b Stent placement along the guidewire. Abbreviation: ERDC, endoscopic retrograde direct cholangioscopy.
Super-selective bile duct cannulation and guidewire placement: a Guidewire placement in the bile duct under ERDC guidance; b Successful guidewire insertion; c Bougie dilation of the common bile duct. Abbreviation: ERDC, endoscopic retrograde direct cholangioscopy.
Endoscopic suturing technique.
Placement of the biliary drainage tube: a Insertion of the drainage tube along the guidewire; b Fluoroscopic confirmation of correct placement of the drainage tube, stent, and metal clip, with no contrast agent leakage observed.
The visual capabilities of ERDC enabled the early identification of Type III EP. ERDC offers a direct and intuitive method for observing ruptures in the bile or pancreatic ducts.Video 1
In this case, the visual capabilities of ERDC enabled the early identification of Type III EP. In contrast to conventional ERCP, which depends on contrast agent diffusion for EP diagnosis and carries a risk of inducing peritoneal infection, ERDC offers a direct and intuitive method for observing ruptures in the bile or pancreatic ducts. This facilitates precise and selective intubation.
Endoscopy_UCTN_Code_TTT_1AR_2AK
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bishay K Meng ZW Khan R Adverse events associated with endoscopic retrograde cholangiopancreatography: systematic review and meta-analysis Gastroenterology 202516856858610.1053/j.gastro.2024.10.03339515394 · doi ↗ · pubmed ↗
- 2Plecic N Malenkovic A Begovic A Management of ERCP-related perforations: A Single-Center Experience J Clin Med 202414110.3390/jcm 1401000139797084 PMC 11720675 · doi ↗ · pubmed ↗
- 3Emori T Yamasaki T Itonaga M Management of ERCP-related perforation: a large multicenter study Gastrointest Endosc 20251029710500010.1016/j.gie.2024.12.01839689733 · doi ↗ · pubmed ↗
- 4Liu WH Huang XY Hu X Initial experience of visualized biliary cannulation during ERCP Endoscopy 2023551037104210.1055/a-2113-895237339664 · doi ↗ · pubmed ↗
- 5Liu WH Huang XY Zhang RY From darkness to brightness: the cholangioscopy-guided selective biliary cannulation with the help of transparent cap during ERCP Endoscopy 20235501 E 320E 32110.1055/a-1981-250336513111 PMC 9833945 · doi ↗ · pubmed ↗