Granulomatosis With Polyangiitis (GPA): A Case Report
Rana Hoseen, Sara G Haroutunian, Salvatore Grasso, Donya Farmand, Marinelle Camilon, Sanaz Hashemi

TL;DR
This case report describes a young woman diagnosed with GPA, a rare vasculitis disease, after experiencing persistent symptoms and abnormal imaging findings.
Contribution
The novelty lies in presenting a rare clinical case of GPA in a young female with atypical initial symptoms.
Findings
The patient had persistent dry cough, weight loss, and lung infiltrates that led to GPA diagnosis.
Biopsy confirmed GPA vasculitis associated with ANCA-related inflammation.
The case highlights the importance of considering GPA in patients with unexplained respiratory and systemic symptoms.
Abstract
Granulomatosis with polyangiitis (GPA) is a rare necrotizing vasculitis disease affecting small to medium vessels. The exact cause of GPA is not fully understood, but the inflammation is associated with anti-neutrophil-cytoplasmic-antibody (ANCA). GPA involves the upper and lower respiratory tract, systemic vasculitis, and glomerulonephritis. This case report describes a young female patient presenting with a dry cough for a month that did not improve with Bactrim, weight loss, sinusitis, mastoid effusion, and multiple mass-like infiltrates in the lungs on imaging, who was found to have GPA vasculitis after being confirmed with a biopsy.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
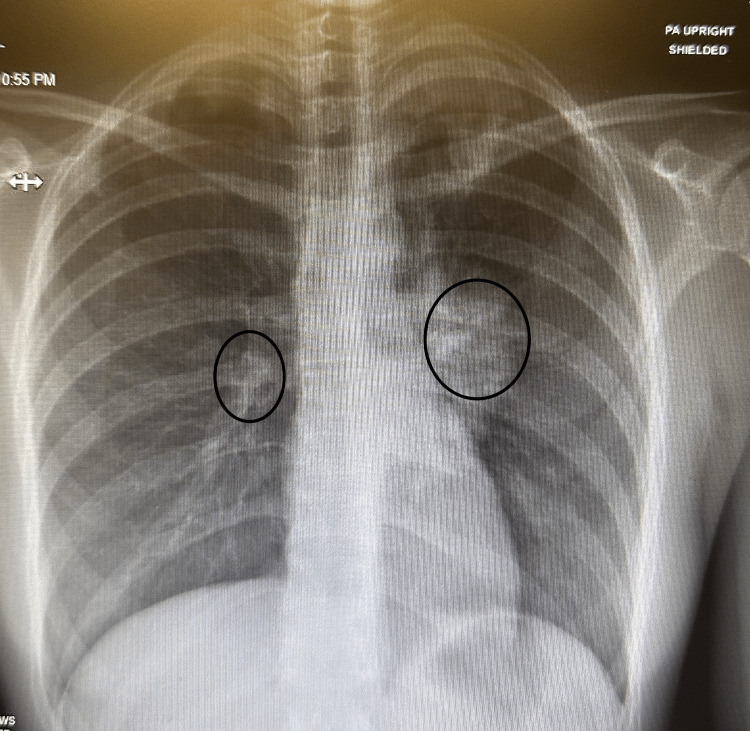 Figure 1
Figure 1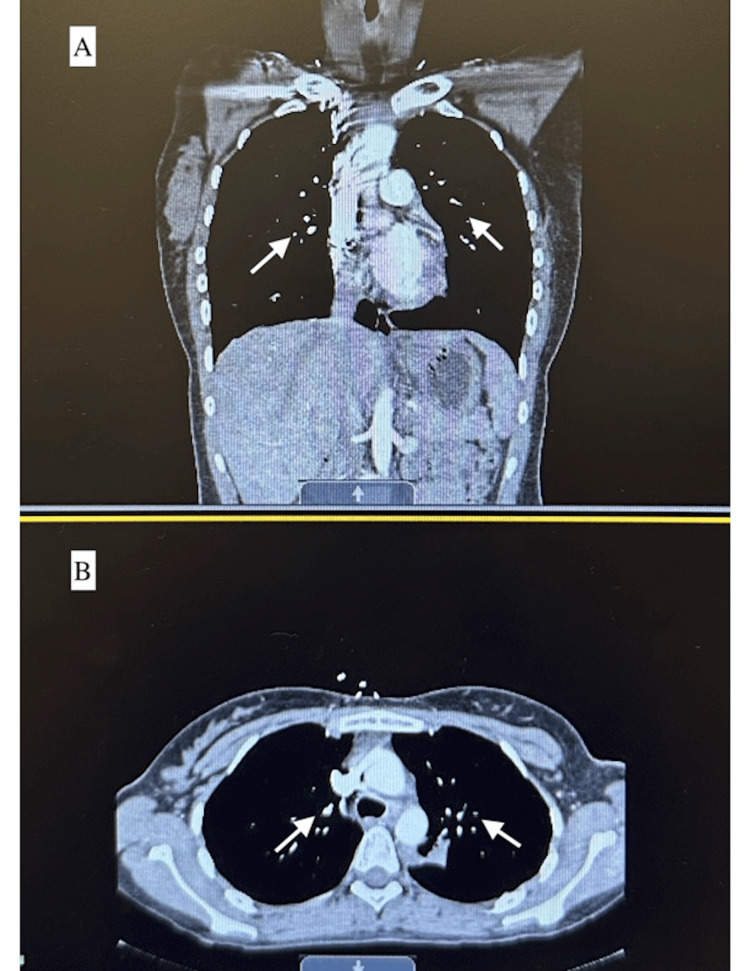 Figure 2
Figure 2 Figure 3
Figure 3| Lab values and vital signs | Patient's values | Normal range |
| Complete blood count (CBC) | Leukocyte of 23.3 thousand/uL | 5.0-11.0 thousand/uL |
| Heart rate (HR) | 130 beats per minute (BPM) | 60-100 BMP |
| Urine red blood cells (RBC) | 51-100 | None |
| Comparison Criteria | 27 y.o. female (our patient) | 62 y.o. female [ | 70 y.o. male [ | 52 y.o. male [ | 66 y.o. male [ |
| Generalized symptoms | Cough, weight loss, shoulder pain | Cough, weight loss | weight loss, fatigue, dry cough | Fever, cough, arthralgia | Fever, cough |
| Upper respiratory symptoms | Mastoiditis, sinusitis | Sinusitis, hearing loss | Otitis media | Runny nose | None |
| Lower respiratory symptoms | Mass-like infiltrates in the lungs | left lower lobe lung mass | Multiple small infiltrates in both lungs | Reticulonodular shadows scattered all over the lung field | bilateral parenchymal and pleural-based nodules |
| Kidney | Mild hematuria was noted on UA but had stable renal function | None | None | Proteinuria, pauci-immune deposition of antibodies, mostly IgG, in a linear pattern with crescent formation | Hematuria and proteinuria, segmental necrotizing, and crescentic glomerulonephritis with granulomatous features |
| Blood vessel | No purpura was seen | None | None | None | None |
| Lab results | Leukocytosis, elevated ESR and CRP, Positive c-ANCA against PR3 | Leukocytosis, elevated ESR, Positive c-ANCA | Leukocytosis, elevated CRP, positive p-ANCA | Elevated ESR, positive p-ANCA | Positive c-ANCA |
| Treatment | Steroids and methotrexate | Steroids and methotrexate | Steroids and cyclophosphamide | Steroids and azathioprine | Steroids and plasmapheresis, then rituximab was added |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVasculitis and related conditions · Sarcoidosis and Beryllium Toxicity Research · Whipple's Disease and Interleukins
Introduction
Vasculitis is an autoimmune disorder in which the body's defense system attacks healthy tissues, such as granulomatosis with polyangiitis (GPA) vasculitis [1]. GPA is a small to medium vessel inflammation associated with anti-neutrophilic-cytoplasmic-antibody (ANCA). ANCA activates neutrophils, which increases their adherence to the endothelium to form neutrophilic microabscesses that lead to the formation of granulomas. These granulomas will cause partial or total occlusion of blood vessels, decreasing the blood flow to distal organs [2]. Researchers believe an infection might contribute to the onset of GPA in addition to environmental and genetic factors [1]. GPA affects the blood vessels of the nose, sinuses, throat, lungs, and kidneys [3]. The first case reported was by a German medical student in 1931.
The severity of the symptoms of GPA varies from one person to another; some patients might have mild symptoms, while others might develop severe or life-threatening symptoms [1]. Patients usually present with nonspecific symptoms such as fever, weight loss, and myalgia. Also, 90% of the patients will have upper respiratory tract problems such as sinusitis, crusting rhinitis, otitis media, mastoiditis, and hearing loss. Nearly 50% of patients present with bilateral or unilateral pulmonary infiltrates. About 50-60% of the patients have dermatological involvement, including purpura of the lower extremities. About 10-20% of patients have rapidly progressive glomerulonephritis leading to chronic kidney disease or end-stage renal disease. Finally, half of the patients have eye involvement, such as developing conjunctivitis or scleritis [2].
Diagnosis requires blood and urine tests, imaging studies, and a biopsy to confirm the diagnosis. Blood tests will show elevated C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), and positive ANCA. Urine tests will show abnormal results, including positive red blood cells (RBC) or elevated protein, to indicate affected kidneys [2]. Computed tomography (CT) and chest X-rays (CXR) will show lesions or hemorrhages in the lungs [2]. Lastly, lung or renal biopsy is the definitive method of confirming GPA.
Case presentation
A 27-year-old female with no significant past medical history presented to the emergency department with a dry cough for a month, along with night sweats and weight loss, and failed an oral trimethoprim-sulfamethoxazole course.
On admission, the patient had leukocytosis (23.3 cells/μL) and tachycardia (130 bpm), as seen in Table 1 below. CXR and CT angiography of the chest showed multiple mass-like lung infiltrates as seen in Figures 1 and 2. The patient was admitted for further evaluation. Infectious disease (ID) was consulted, and the patient was started on empiric intravenous antibiotics (IV Abx) while cultures were pending, with no improvement. IV Abx was discontinued. A pulmonary consult was recommended for empiric steroids and status post bronchoscopy, and a lung biopsy was suggested if there was no improvement. Cultures from bronchoscopy showed no growth.
Chest X-rays The circles show mass-like infiltration in the lung parenchyma
CT of the chest A) Coronal CT scan of the chest that shows mass-like infiltrates within the left and right lung cavities (white arrows); B) Axial CT scan of the chest that shows mass-like infiltrates within the left and right lung cavities (white arrows)
The patient complained of chronic left mastoiditis, which was seen in CT of the temporal bone, and she was started on Loratadine to help with the symptoms per the ear nose throat (ENT) specialist's recommendation. CT of the orbit showed sinusitis and mastoid effusion but no lymphadenopathy to suggest lymphoma or other malignancy, as shown in Figure 3. ENT recommended an outpatient audiometric evaluation and added fluticasone nasal spray and loratadine for nasal congestion. The patient also had left shoulder pain, but the X-ray was normal. The patient developed conjunctivitis on day four of admission and was treated with neomycin + polymyxin B + dexamethasone ophthalmic drops for five days per ID.
CT of the orbit/stella/posterior fossa without contrast
The patient's C-ANCA against PR3 was markedly elevated (492 U/mL), suggesting GPA vasculitis with primary pulmonary and upper airway involvement. On the physical exam, there was no obvious rash on her extremities available for biopsy, and she had no current renal involvement. Therefore, the patient underwent successful video-assisted thoracic surgery (VATS) with wedge resection biopsy on day 12 of admission by cardiothoracic surgery. The pathology of the biopsy confirmed GPA vasculitis, as it showed acute capillaritis and poorly formed epithelioid granulomas. Therefore, the patient began taking steroids and methotrexate. Three days later, a repeat CXR showed a trace left-sided pneumothorax and ill-defined left retrocardiac opacities, suggesting atelectasis.
Nephrology was consulted to evaluate the renal involvement of GPA. The patient had stable renal function throughout admission; however, hematuria was noted on urine analysis, as seen in Table 1 below. The patient was recommended to follow up with outpatient nephrology for further evaluation. The ophthalmology consultant noted that the patient did not have manifestations of vasculitis on the exam, and the redness in the eyes was due to dry eyes. The patient can use eye lubricant to help with symptoms.
On the day of discharge, the patient was hemodynamically stable, tolerating diet, and ambulating. The patient was advised to follow up with her primary care provider within one week to obtain appropriate outpatient follow-ups with specialists. The patient was discharged with a three-week 30 mg steroid dose, then tapered by 10 mg weekly, and trimethoprim-sulfamethoxazole as prophylaxis, and was given methotrexate and steroids.
Discussion
GPA is a rare disease that causes inflammation in the blood vessels (vasculitis) and tissues such as the lungs, sinuses, and kidneys, which can lead to organ system damage. It can affect people of all ages, but the peak age group is the 5th-7th decade of life [4]. As a result, physicians may be less likely to consider GPA in younger adults, potentially leading to delayed or missed diagnosis despite the presence of suggestive symptoms. Our patient came in complaining of a month-long history of cough, weight loss, and night sweats, along with elevated ESR and CRP that are suggestive of lung carcinoma, lymphoma, tuberculosis, or systemic vasculitis. Further investigations showed that the patient has positive c-ANCA against PR3, which is highly supportive of vasculitis. Therefore, a biopsy was done and the diagnosis was confirmed.
This patient exhibited a typical presentation of GPA, including sinusitis, a mass-like infiltrate in the lungs on chest CT, cough, nasal congestion, and conjunctivitis. These features align with the most frequently reported symptoms in GPA, as illustrated in Table 1. Although there was no evidence of renal involvement at the time of evaluation, the patient was referred to outpatient nephrology for ongoing monitoring to help prevent the development of progressive glomerulonephritis.
The patient was started on a 30 mg dose of steroids for three weeks, then tapered down by 10 mg weekly due to the patient's low body weight, as well as Methotrexate. Her symptoms were improving with the treatment, and she was advised to follow up with the specialists to manage her disease and prevent any worsening prognosis.
Conclusions
This case highlights an uncommon presentation of granulomatosis with polyangiitis (GPA) in a young woman, characterized by prominent respiratory involvement without renal dysfunction or vasculitic symptoms. GPA, though more prevalent in older adults, should be considered in patients of all ages who present with unexplained respiratory symptoms, systemic features, and radiologic lung findings. Early diagnosis, ideally confirmed through tissue biopsy, is critical to initiate timely immunosuppressive therapy and prevent disease progression. Treatment typically involves corticosteroids combined with immunosuppressive agents such as methotrexate or cyclophosphamide, followed by maintenance therapy to minimize relapse risk. This case underscores the importance of maintaining a broad differential diagnosis and close monitoring, even in atypical patient populations.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Granulomatosis with polyangiitis 20242025 https://vasculitisfoundation.org/education/vasculitis-types/granulomatosis-with-polyangiitis/
- 2Granulomatosis With Polyangiitis Rout P Garlapati P Qurie A Treasure Island, FL Stat Pearls Publishing 2024 https://www.ncbi.nlm.nih.gov/books/NBK 557827/32491759 · pubmed ↗
- 3Granulomatosis with polyangiitis Mayo Foundation for Medical Education and Research.(2022 November 30 2022 https://www.mayoclinic.org/diseases-conditions/granulomatosis-with-polyangiitis/symptoms-causes/syc-20351088
- 4Granulomatosis with polyangiitis (GPA, formerly called Wegener’s) Professional Professional CC 2025 https://my.clevelandclinic.org/health/diseases/granulomatosis-with-polyangiitis-formerly-wegeners-granulomatosis
- 5From triumph to tribulation: a granulomatous polyangiitis case report Int J Resp Pulmon Med Anthony AIL Ibrahim ZA Loh LC 2019 https://clinmedjournals.org/articles/ijrpm/international-journal-of-respiratory-and-pulmonary-medicine-ijrpm-6-113.php
- 6A case of granulomatosis with polyangiitis (Wegener's granulomatosis) presenting with marked inflamed tracheobronchial mucosa Case Rep Med Nishiuma T Ohnishi H Yoshimura S Kinami S Sakamoto S 20819420132013 https://www.hindawi.com/journals/crim/2013/208194/ 2419883410.1155/2013/208194 PMC 3806251 · doi ↗ · pubmed ↗
- 7A case of granulomatosis with polyangiitis (Wegener's granulomatosis) presenting with rapidly progressive glomerulonephritis Cureus Hasan MR Sakibuzzaman M Tabassum T Moosa SA 011201910.7759/cureus.5896 PMC 683975431772866 · doi ↗ · pubmed ↗
- 8Granulomatosis with Polyangiitis (GPA) Case Report Outlining the Importance of Urinalysis in Patients Presenting with Pulmonary Cavitary Lesions Pulm Crit Care Med Zagelbaum N Shamim Z Gilani A El Zarif S Krishna MG D'Agati VD Obligado S 2016 https://www.oatext.com/Granulomatosis-with-Polyangiitis-GPA-Case-Report-Outlining-the-Importance-of-Urinalysis-in-Patients-Presenting-with-Pulmonary-Cavitary-Lesions.php