Comparison of Hemostatic Activity in Canine Leukoreduced Cryoprecipitate, Cryopoor Plasma, and Fresh Plasma
Roberta Perego, Eva Spada, Luciana Baggiani, Giuliano Ravasio, Enrica Zucca, Graziella Vanosi, Giancarlo Ruffo, Daniela Proverbio

TL;DR
This study compares the clotting abilities of different types of canine blood products and finds that cryoprecipitate has higher Factor VIII, which is important for blood clotting.
Contribution
The study is the first to evaluate hemostatic activity in canine leukoreduced cryoprecipitate and cryopoor plasma, providing new insights into their clinical utility.
Findings
Factor VIII activity is significantly higher in LR-CRYO compared to LR-FP.
Refrozen LR-CRYO shows no significant differences in most hemostatic factors compared to LR-CRYO.
LR-CPP has higher Factor X activity and albumin concentration but lower von Willebrand Factor and fibrinogen.
Abstract
To date, no studies have reported the evaluation of hemostatic activity in canine leukoreduced cryoprecipitate (LR‐CRYO) and leukoreduced cryopoor plasma (LR‐CPP). We aimed to compare the hemostatic activity of LR‐CRYO and LR‐CPP to leukoreduced fresh plasma (LR‐FP) and to evaluate the preservation of LR‐CRYO by refrigeration and refreezing after thawing. Four hundred fifty milliliters of fresh blood was collected from ten donor dogs, leukoreduced, and separated into LR‐FP, then frozen (−20°C) to obtain leukoreduced fresh frozen plasma (LR‐FFP). LR‐FFP was further separated into LR‐CRYO and LR‐CPP. LR‐CRYO was frozen, thawed, and divided into two bags, one refrigerated for 24 h and one refrozen for 7 days. Factor VIII (FVIII) and X (FX) activity, prothrombin time, activated partial thromboplastin time, antithrombin III (ATIII) activity (ATA), total protein, albumin, fibrinogen, and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
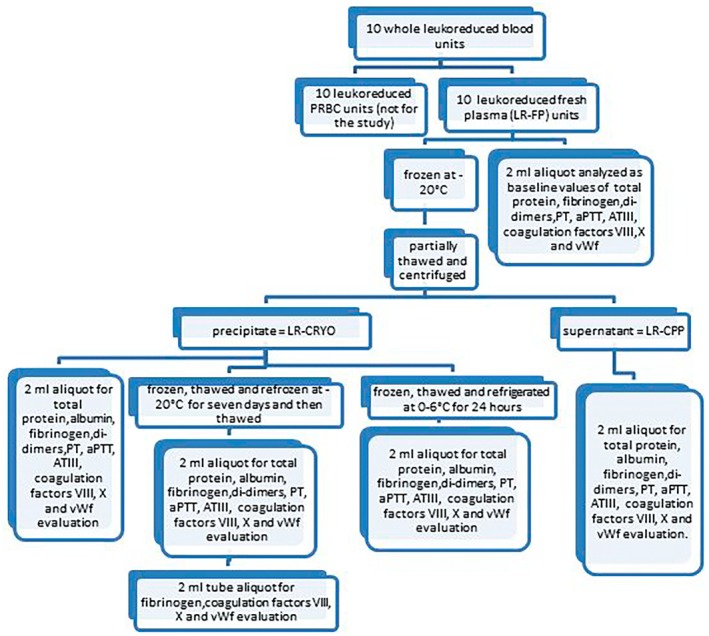 FIGURE 1
FIGURE 1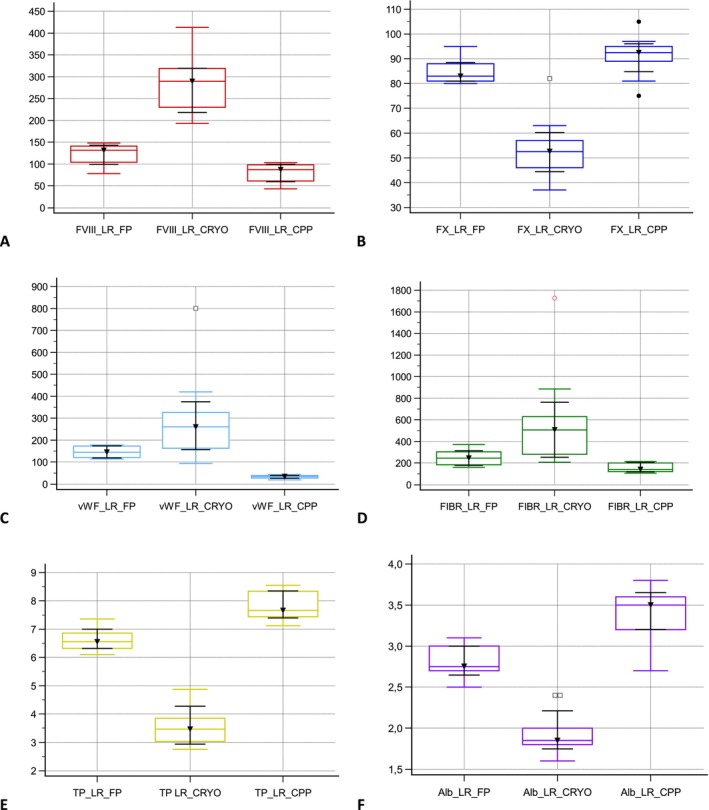 FIGURE 2
FIGURE 2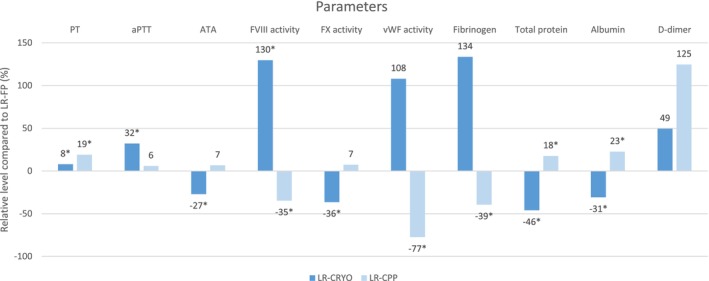 FIGURE 3
FIGURE 3| Analyte (RI) | Component | Min | Max | Median (95% CI) |
|
|
|---|---|---|---|---|---|---|
| PT (7–9.8 s) | LR‐FP | 7.3 | 8.7 | 8.1 (7.6–8.4) | — |
|
| LR‐CRYO | 7.6 | 9.5 | 8.6 (8.3–9.3) |
| — | |
| LR‐CPP | 8.6 | 10.4 | 9.6 (8.9–10.1) |
|
| |
| aPTT (11–16.9 s) | LR‐FP | 13.4 | 15.6 | 14.6 (13.9–15) | — |
|
| LR‐CRYO | 15.4 | 24.6 | 18.5 (17.3–21.2) |
| — | |
| LR‐CPP | 12.7 | 20.1 | 14.6 (14–15.7) | 1.000 |
| |
| ATIII (95%–140%) | LR‐FP | 112 | 132 | 128 (119–132) | — |
|
| LR‐CRYO | 68 | 127 | 88 (76–105) |
| — | |
| LR‐CPP | 121 | 136 |
|
|
| |
| FVIII (50%–150%) | LR‐FP | 78 | 148 | 132 (104–141) | — |
|
| LR‐CRYO | 193 | 413 | 289 (230–319) |
| — | |
| LR‐CPP | 43 | 103 | 87 (61–98) |
|
| |
| FX (80%–175%) | LR‐FP | 80 | 95 | 83 (81–88) | — |
|
| LR‐CRYO | 37 | 82 | 53 (46–57) |
| — | |
| LR‐CPP | 75 | 105 | 93 (89–95) | 0.4055 |
| |
| vWF (70%–180%) | LR‐FP | 114 | 178 | 145 (121–173) | — | 0.3336 |
| LR‐CRYO | 94 | 801 | 261 (163–326) | 0.3336 | — | |
| LR‐CPP | 19 | 43 | 34 (27–39) |
|
| |
| Fibrinogen (100–400 mg/mL) | LR‐FP | 160 | 371 | 245 (184–304) | — | 0.3847 |
| LR‐CRYO | 207 | 1727 |
| 0.3847 | — | |
| LR‐CPP | 106 | 215 | 140.6 (120.7–201) |
| 0.1451 | |
|
Total protein (6–8 g/dL) | LR‐FP | 6.1 | 7.4 | 6.6 (6.3–6.9) | — |
|
| LR‐CRYO | 2.8 | 4.9 | 3.5 (3–3.9) |
| — | |
| LR‐CPP | 7.1 | 8.6 | 7.7 (7.4–8.3) |
|
| |
| Albumin (2.3–3.2 g/dL) | LR‐FP | 2.5 | 3.1 | 2.8 (2.7–3) | — |
|
| LR‐CRYO | 1.6 | 2.4 | 1.9 (1.8–2) |
| — | |
| LR‐CPP | 2.7 | 3.8 | 3.5 (3.2–3.6) |
|
| |
| D‐Dimers (0.01–0.35 μg/mL) | LR‐FP | 0.12 | 0.27 | 0.16 (0.15–0.18) | — | 1.0000 |
| LR‐CRYO | 0.05 | 0.75 |
| 1.0000 | — | |
| LR‐CPP | 0.15 | 1.25 |
| 0.7507 | 0.1926 |
| Analyte (reference range) | Component | Min | Max | Mean (±SD) or median (95% CI) |
|
|---|---|---|---|---|---|
| PT (7–9.8 s) | LR‐CRYO | 7.6 | 9.5 | 8.6 (8.3–9.3) |
|
| Refrigerated‐LR‐CRYO | 7.7 | 9.1 | 8.4 (8.1–8.5) | 0.1133 | |
| Refrozen‐LR‐CRYO | 7.8 | 9.0 | 8.4 (8.1–8.8) | 1.0000 | |
| aPPT (11–16.9 s) | LR‐CRYO | 15.4 | 24.6 | 18.5 (17.3–21.2) |
|
| Refrigerated‐LR‐CRYO | 15.3 | 24.9 | 18.3 (17–22) | 1.0000 | |
| Refrozen‐LR‐CRYO | 15.2 | 24.2 | 19 (18–20.9) | 1.0000 | |
| ATIII (95%–140%) | LR‐CRYO | 68 | 127 | 88 (76–105) |
|
| Refrigerated‐LR‐CRYO | 69 | 123 | 84 (73–100) |
| |
| Refrozen‐LR‐CRYO | 73 | 115 | 89 (76–98) | 1.0000 | |
| FVIII (50%–150%) | LR‐CRYO | 193 | 413 | 289 (230–319) |
|
| Refrigerated‐LR‐CRYO | 114 | 504 | 232 (217–290) | 1.0000 | |
| Refrozen‐LR‐CRYO | 171 | 407 |
| 0.9009 | |
| FX (80%–175%) | LR‐CRYO | 37 | 82 | 53 (46–57) |
|
| Refrigerated‐LR‐CRYO | 41 | 77 | 53 (52–54) | 1.0000 | |
| Refrozen‐LR‐CRYO | 41 | 79 | 55 (51–57) | 1.0000 | |
| vWF (70%–180%) | LR‐CRYO | 94 | 801 | 261 (163–326) |
|
| Refrigerated‐LR‐CRYO | 100 | 810 | 238 (138–340) | 0.9634 | |
| Refrozen‐LR‐CRYO | 51 | 794 |
| 0.1185 | |
| Fibrinogen (100–400 mg/mL) | LR‐CRYO | 207.2 | 1727.4 |
|
|
| Refrigerated‐LR‐CRYO | 197.1 | 1984.2 |
| 1.0000 | |
| Refrozen‐LR‐CRYO | 161.8 | 1998.0 |
| 1.0000 | |
| Total protein (6–8 g/dL) | LR‐CRYO | 2.8 | 4.9 | 3.5 (3–3.9) |
|
| Refrigerated‐LR‐CRYO | 2.9 | 4.7 | 3.5 (3.2–3.8) | 1.0000 | |
| Refrozen‐LR‐CRYO | 2.9 | 4.7 | 3.6 (3.1–3.8) | 1.0000 | |
| Albumin (2.3–3.2 g/dL) | LR‐CRYO | 1.6 | 2.4 | 1.9 (1.8–2) |
|
| Refrigerated‐LR‐CRYO | 1.6 | 2.4 | 1.9 (1.7–2) | 1.0000 | |
| Refrozen‐LR‐CRYO | 1.6 | 2.4 | 1.9 (1.7–2.1) | 1.0000 | |
| D‐Dimers (0.01–0.35 μg/mL) | LR‐CRYO | 0.05 | 0.75 |
|
|
| Refrigerated‐LR‐CRYO | 0.07 | 0.77 |
| 0.7469 | |
| Refrozen‐LR‐CRYO | 0.04 | 0.85 |
| 1.0000 |
- —Piano di Sostegno alla Ricerca 2021, Linea 2—Azione A, University of Milan, Italy
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTrauma, Hemostasis, Coagulopathy, Resuscitation · Hemostasis and retained surgical items · Hemophilia Treatment and Research
Introduction
1
Current human and veterinary transfusion medicine favors goal‐oriented blood component selection based on individual patient requirements [1]. Cryoprecipitate (CRYO), a blood component that precipitates when fresh frozen plasma (FFP) is slowly, partially thawed and centrifuged [2], contains cold‐insoluble plasma proteins (i.e., von Willebrand factor [vWF], factor VIII [FVIII], factor XIII, fibrinogen, and fibronectin) [3]. Its key therapeutic advantage compared with FFP is higher hemostatic plasma protein concentration while in a much smaller plasma volume, thereby avoiding volume overload in recipients that are normovolemic or sustain congestive heart failure or renal failure [4]. CRYO might be used to treat coagulopathies in critically ill patients, but with the advent of recombinant human vWF and FVIII proteins, CRYO is now mainly used in humans in bleeding trauma patients requiring massive transfusion [1] and those with dysfibrinogenemia and acquired hypofibrinogenemia [5, 6, 7]. In dogs, CRYO is mainly used for bleeding management or prevention in cases of hemophilia A and von Willebrand disease (vWD) [4, 8]. In human medicine, CRYO preparations have been evaluated regarding their indications, dosing, and potential adverse effects [9, 10, 11, 12, 13]. Likely, canine CRYO has similar qualities to those in humans, although these have yet to be confirmed. The potential uses of CRYO in dogs were recently reviewed [1]. In vitro studies of canine CRYO are limited [2, 14, 15]. In one study, FVIII and vWF stabilities in canine CRYO were determined. Another, more recent study has examined the ability of cryopoor plasma (CPP) to correct vitamin K‐dependent coagulopathy in dogs.
The supernatant fraction, removed when producing CRYO, is termed cryopoor plasma (CPP), cryosupernatant, or cryodepleted plasma. It is considered a less useful by‐product component of CRYO production for treating hemostatic disorders. Nevertheless, recent studies in dogs suggest that CPP contains similar concentrations of vitamin K‐dependent factors II, VII, and X (FX) and higher albumin concentration and colloid osmotic pressure (COP) [14] than FFP. CPP improves the clotting times and vitamin K‐dependent coagulation factors concentrations similarly to FFP [16].
Whole blood or blood component transfusions might cause serious, potentially fatal adverse recipient reactions, some of which are caused by the presence and activity of leukocytes [17, 18]. Therefore, human blood components are subjected to leukoreduction [19]. In human blood components, leukoreduction might lead to decreased coagulation factors VII, VIII, and XI, and longer activated plasma thromboplastin time (aPTT) in leukoreduced FFP [20, 21, 22], although reported results vary [23, 24, 25], and differences between studies are possibly attributed to differences in filter type [21]. Nevertheless, none of the differences observed in leukoreduced components was clinically significant [22]. Recently, several in vitro veterinary studies have reported production with leukoreduction of canine blood components [17, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38] and their use [39, 40, 41, 42, 43, 44]. Only two studies [30, 38] have evaluated coagulation factor levels in canine leukoreduced FP, finding no or few significant ones (i.e., factor XI and aPTT) [30], which do not affect the component's therapeutic efficacy.
To the authors' knowledge, the hemostatic activity of canine leukoreduced CRYO and CPP has not been reported. The main aim of this study was therefore to determine the hemostatic activity of leukoreduced CRYO (LR‐CRYO) and leukoreduced CPP (LR‐CPP) compared to that of leukoreduced fresh plasma (LR‐FP). Unlike human blood components, there are no relevant differences in most hemostatic factors between leukoreduced and non‐leukoreduced canine plasma. We hypothesized that the hemostatic characteristics of canine LR‐CRYO and canine non‐leukoreduced CRYO are similar and that LR‐CRYO would show higher concentrations of fibrinogen, FVIII, and vWF levels than its source, LR‐FP, and LR‐CPP would show lower levels of these factors. We also hypothesized that LR‐CPP albumin concentration and FX activity would be similar to or higher than their levels in LR‐FP. A secondary aim of this study was to determine the hemostatic activity of LR‐CRYO stability when refrigerated and when refrozen after thawing.
Materials and Methods
2
Blood Donors
2.1
The study was approved by the Animal Welfare Bio Ethical Committee of the University of Milan (OPBA_26_2018). Blood units were collected with the dog owners informed consent from 10 blood donor dogs (intact females, 6; intact males, 4), with a mean age of 3.2 years (±1.03 years, range 2–5 years), of different breeds (Segugio Italiano, 4; Dogo Argentino, 4; Bernese mountain dogs, 2) belonging to the Volunteer Blood Donors Program of the Veterinary Transfusion Research Laboratory (REVLab) of the Department of Veterinary Medicine and Animal Science, University of Milan. The donors were DEA‐1 (Lab Test DEA 1, Alvedia, Limonest, France), DEA‐4 and Dal‐positive, and DEA‐7 negative (ID‐CARD NaCl enzyme test and cold agglutinins, DiaMed GmbH, Cressier FR, Switzerland). The donor dogs fulfilled the criteria for selection issued by the Italian Ministry of Health guidelines for veterinary transfusion medicine [45] (i.e., body weight > 25 kg, age 2–8 years, current vaccination, and ecto‐ and endo‐parasites prophylaxis). Dogs were deemed healthy based on their unremarkable clinical history, physical examination, complete blood count, routine serum biochemistry, and hemostatic tests (prothrombin time, activated partial thromboplastin time and fibrinogen concentration) and negative serology for Dirofilaria immitis (Snap Canine Heartworm antigen test kit, IDEXX), Anaplasma phagocytophilum (Fluo Anaplasma Biopronix kit, Agrolabo Spa, Scarmagno, Turin, Italy), Ehrlichia canis (Fluo Ehrlichia Biopronix kit Agrolabo Spa, Scarmagno, Turin, Italy), Babesia canis (Fluo Babesia Biopronix kit, Agrolabo Spa, Scarmagno, Turin, Italy), Leishmania infantum (Fluo Leishmania Biopronix kit, Agrolabo Spa, Scarmagno, Turin, Italy), Rickettsia conorii (Fluo Rickettia Biopronix kit, Agrolabo Spa, Scarmagno, Turin, Italy). In addition, for Babesia spp., microscopic observation of a fresh blood smear was performed, while for Dirofilaria spp. the microhematocrit method was done. Donors were not administered medications known to interfere with hemostasis for 6 months prior to the study.
Blood Collection and Processing
2.2
Whole blood (450 ± 50 mL) was collected into a commercial closed collection system for human use (CompoSelect Premium T&T CPD/SAG‐M, Fresenius Kabi Italia S.r.l., Isola della Scala (VR) Italy) by jugular or cephalic venipuncture by gravity with the help of a blood collection scale/mixer with high/low blood flow alarm (Hemotek‐2, Delcon, Italy) with no sedation, following standard operating procedures of the Veterinary Transfusion Research Laboratory (REVLab) of the Department of Veterinary Medicine and Animal Science, University of Milan. No adverse reactions were noted in dogs during or after blood donation. The blood collection quadruple bag system, previously shown to be applicable for use in dogs [27], consisted of a primary bag, containing 63 mL of citrate, phosphate, dextrose (CPD) anticoagulant‐preservative solution in the and 100 mL of sodium chloride‐adenine‐glucose‐mannitol (SAG‐M) solution in one of the two satellite storage bags. The primary bag was connected to a secondary empty bag with an in‐line leukocyte soft filter for pre‐storage leukoreduction. This filter is a neutral‐charged, third‐generation polyester filter, fabricated to remove both leukocytes (WBCs) and platelets (PLTs). After collection, the primary bag containing the collected blood was macroscopically inspected for clots, delicately mixed, weighed, and a 2 mL aliquot was taken for further analysis. The integral canal above the filter was then broken, and the contents of the primary bag were drained through the filter and collected by gravity into the secondary bag at room temperature (20°C). Filtration time varied between 15 and 30 min. All 10 leukoreduced whole blood (LR‐WB) units were collected on the same day and stored at 2°C–6°C pending completion of collections.
After leukoreduction, a 2 mL aliquot of LR‐WB was taken from each unit for subsequent analysis. The secondary bags, containing LR‐WB, were then centrifuged (4657 g for 15 min, 4°C; Rotixa 50RS centrifuge, Hettich Lab Technology, Milan, Italy) within 6 h from blood collection. The supernatant leukoreduced fresh plasma (LR‐FP) was expressed into an attached empty satellite bag using a manual plasma extractor, leaving approximately 2 mL of LR‐FP in the transfer tubing of the satellite bag, which was transferred into a polypropylene test tube for further analysis. The LR‐FP bag (containing 200 mL) was separated from the collection system and from the transfer tubing using an electric tube sealer (HemoWeld, Delcon, Monza Brianza, Italy) and frozen at −20°C in a dedicated plasma unit freezer (Fiocchetti snc, Luzzara, Italy) to prepare LR‐FFP, used in this study. The remaining leukoreduced packed RBCs were transferred into the SAG‐M satellite bag and stored at 2°C–6°C in a dedicated blood unit refrigerator (Fiocchetti snc, Luzzara, Italy) and were used for transfusion purposes unrelated to this study. Within 2 days of freezing at −20°C, the LR‐FFP was thawed in a refrigerator at 2°C–6°C for 15–18 h, until reaching a slushy consistency, and then centrifuged (at 1°C–6°C, at 4657 g for 5 min), as previously described [14]. The precipitate product obtained was the leukoreduced cryoprecipitate (LR‐CRYO) while the supernatant fraction was the leukoreduced cryopoor plasma (LR‐CPP), which was then transferred into a satellite bag (Compoflex Transfer Bag, 150 mL) with a sterile spike (Fresenius Kabi Italia S.r.l., Isola della Scala, VR, Italy), while the LR‐CRYO ( 60–90 mL) remained in the principal bag. LR‐CCP and LR‐CRYO 2 mL aliquots were collected for further analysis.
For the second purpose of the study, before freezing, LR‐CRYO was divided into two satellite plasma bags containing 30–40 mL volumes using a sterile spike (Fresenius Kabi Italia S.r.l., Isola della Scala, VR, Italy). After 24 h, the two frozen LR‐CRYO satellite bags were thawed in a water bath at 37°C, and one bag was refrigerated at 2°C–6°C (refrigerated‐LR‐CRYO) while the other bag was refrozen at −20°C (refrozen‐LR‐CRYO). After 24 h, a 2 mL refrigerated‐LR‐CRYO aliquot was obtained for further analysis. After 7 days, the refrozen‐LR‐CRYO bag was rethawed in a water bath at 37°C, and then, similarly, a 2 mL aliquot was obtained for further analysis. Finally, a 2 mL aliquot was obtained from the transfer tubing of the refrozen‐LR‐CRYO bag (tube‐refrozen‐LR‐CRYO) to compare with the results of the analysis done in the refrozen‐LR‐CRYO bag sample (refrozen‐LR‐CRYO) to determine, for future studies, if the transfer tubing content adequately represents the bag content.
Laboratory Analysis
2.3
The sample aliquots of WB, LR‐WB, LR‐FP, LR‐CRYO, LR‐CPP, refrigerated‐LR‐CRYO, refrozen‐LR‐CRYO, and tube‐refrozen‐LR‐CRYO were all placed into polypropylene test tubes containing no anticoagulant and analyzed immediately after sampling. For technical reasons, WB and LR‐WB CBC (Cell‐Dyn 3500—Abbott S.r.l., Italy) were performed in only 6/10 samples. With the exception of tube‐refrozen‐LR‐CRYO, the parameters assessed from each sample included factor VIII (FVIII), factor X (FX), antithrombin III (ATIII), and von Willebrand factor (vWF) activities, prothrombin time (PT), activated partial thromboplastin time (aPTT), and fibrinogen, D‐Dimers (DD), total protein, and albumin concentrations. In the tube‐refrozen‐LR‐CRYO samples, only FVIII, FX, and vWF activities and fibrinogen concentration were measured (Figure 1).
Schematic flowchart of study design.
Hemostatic tests, except fibrinogen evaluation, were measured using a coagulometric analyzer (STA Compact Max, Stago Italia SRL, Milan, Italy) with commercial reagents obtained from the analyzer manufacturer. Fibrinogen concentration was measured using the Clauss method (Hagen Diagnostica S.r.l., San Giovanni Valdarno, Italy), total protein (TP, Biuret method, Hagen Diagnostica S.r.l., Firenze, Italy), and albumin (bromocresol green method, Hagen Diagnostica S.r.l., Firenze, Italy) concentrations were measured using spectrochemistry (Cobas Mira Classics, Roche Diagnostics, Basilea, Switzerland). FVIII and FX activities were measured with pooled canine citrate plasma obtained from 10 healthy dogs as a control. For DD, PT, and aPTT, the calibration curve was imported by bar code at each new batch. For ATIII and vWF activities, commercial human plasma controls were used (STA‐Unicalibrator e STA‐vWF: Ag calibrator, Diagnostica Stago, Asnières‐sur‐Seine, France).
Statistical Analysis
2.4
The distribution pattern of results was determined using the Kolmogorov–Smirnov test. Analyte in different sample types (i.e., LR‐FP, LR‐CRYO, LR‐CPP, and refrigerated‐LR‐CRYO and refrozen‐LR‐CRYO) was compared using ANOVA, with Bonferroni's correction for multiple comparisons, followed by post hoc paired Student's t‐test or Wilcoxon Rank‐Signed test, depending on the data distribution pattern. All the tests were two‐tailed, and in all, p < 0.05 was considered significant. T‐test or Wilcoxon test, depending on the data distribution, was used to compare WB and LR‐WB groups and refrozen‐LR‐CRYO and tube‐refrozen‐LR‐CRYO groups. Statistical analyses were conducted, and graphs were created using a commercial software package (MedCalc Statistical Software version 20.027, MedCalc Software Ltd., Ostend, Belgium).
Results
3
The only significant differences in CBC analytes between WB and LR‐WB were in the leukocyte count (10.6 ± 3.6 × 103/μL vs. 0.2 ± 0.1 × 103/μL, respectively; p = 0.0009) and platelet count (22 ± 54 × 103/μL vs. 44 ± 22 × 103/μL, respectively; p = 0.0002). The PT, aPTT, FVIII, FX, AT, and vWF activities, and fibrinogen, DD, albumin, and TP in LR‐FP, LR‐CRYO, and LR‐CPP are reported in Table 2. FVIII activity was higher (p = 0.0001) in LR‐CRYO and lower (p = 0.0003) in LR‐CPP compared with LR‐FP. FX activity was lower in LR‐CRYO compared with LR‐FP (p = 0.0002) and LR‐CPP (p < 0.0001). vWF activity was lower in LR‐CPP compared with LR‐CRYO (p = 0.0217) and LR‐FP (p < 0.0001) and was insignificantly different between LR‐CRYO and LR‐FP (p = 0.3336).
Median fibrinogen concentrations for LR‐FP, LR‐CPP, and LR‐CRYO were 251.6 mg/mL (min–max, 160.3–370.6), 152.4 mg/mL (min–max, 106–214.7), and 506 mg/mL (min–max, 207.2–1727), respectively (Table 1, Figure 2). Fibrinogen concentrations were higher in LR‐FP compared with LR‐CPP (p = 0.0012) but were not different between LR‐CRYO and LR‐CPP (p = 0.3847) or LR‐FP (p = 0.1451) (Figure 2).
Box and whisker plots of some activity levels and concentrations measured for each unit of LR‐fresh plasma (LR‐FP), LR‐cryoprecipitate (LR‐CRYO) and LR‐cryopoor plasma (LR‐CPP). (A) Factor VIII activity levels, Y‐axis represent %, (B) factor X activity levels, Y‐axis represent %, (C) Von Willbrand VIII activity levels, Y‐axis represent %, (D) fibrinogen concentrations, Y‐axis represent mg/dL, (E) total protein concentrations, Y‐axis represent g/L, and (F) albumin concentrations, Y‐axis represent g/L.
TP concentration was higher in LR‐CPP (median, 7.7 g/dL; min–max, 7.4–8.3) than in LR‐FP (median, 6.6 g/dL; min–max, 6.3–6.9) (p < 0.0001) and then in LR‐CRYO (median, 3.6 g/dL; min–max, 3–3.9) (p < 0.0001) (Table 1, Figure 2). LR‐FP TP was higher (p < 0.0001) compared with LR‐CRYO. Albumin concentration was higher in LR‐CPP (median, 3.5 g/dL; min–max, 3.2–3.6) than in LR‐FP (median, 2.8 g/dL; min–max, 2.7–3) (p < 0.0001) and then in LR‐CRYO (median, 1.9 g/dL; min–max, 1.8–2) (p < 0.0001). LR‐FP albumin was higher (p = 0.0001) compared with LR‐CRYO (Table 1, Figure 2).
The relative analyte level differences in LR‐CRYO and LR‐CPP from the LR‐FP baseline are illustrated graphically in Figure 3.
Mean relative difference in analyte levels in leukoreduced cryoprecipitate (LR‐CRYO) and leukoreduced cryopoor plasma (LR‐CPP) from leukoreduced fresh plasma (LR‐FP) depicted as baseline values. PT: prothrombin time; aPTT: activated partial thromboplastin time; FVIII: factor VIII; FX: factor X; ATA: antithrombin III activity; vWF: factor von Willebrand. Asterisks denote significant difference (p < 0.05) compared with LR‐FP level.*
The only significant analyte difference between refrigerated‐LR‐CRYO and refrozen‐LR‐CRYO was in the ATA, which was lower (p = 0.0062) in refrigerated‐LR‐CRYO (median, 84%; min–max, 73–100) than in LR‐CRYO (median, 88%; min–max, 76–105) (Table 2).
The only significant analyte difference between refrozen LR‐CRYO and tube‐refrozen LR‐CRYO was in FX activity, which was higher (p = 0.0018) in tube‐refrozen LR‐CRYO (median, 59%; min–max, 57–63) than in refrozen LR‐CRYO (median, 55%; min–max, 51–57).
Discussion
4
To the author's knowledge, this study is the first reporting the PT, aPTT, ATA, FVIII, and FX activities, and DD, TP, and albumin concentrations in canine LR‐CRYO and LR‐CPP, comparing them to those of the source LR‐FP, and obtaining that FVIII activity was higher in LR‐CRYO vs. LR‐FP, FX activity was higher in LR‐CPP and LR‐FP vs. LR‐CRYO, and albumin concentration was higher in LR‐CPP vs. LR‐FP and LR‐CRYO.
Processing WB to obtain LR‐CRYO for transfusion requires a series of steps that might influence the stability of clotting factors. First, the filters used for leukoreduction might impact WB‐derived plasma quality. Studies in human medicine examined the effects of WB or plasma leukofiltration on residual coagulation factor activity, with conflicting results. Several studies that evaluated several leukoreduction filters in human fresh plasma units indicated that leukofiltration did not activate coagulation and affected coagulation factors activities [23, 24, 46, 47, 48, 49, 50]. Nevertheless, in other studies, during filtration, contact between artificial surfaces and plasma coagulation proteins might induce changes in clotting times and coagulation factor concentration and activity (significant losses of factors V, VII, VIII, IX, XI, and XII, decrease of fibrinogen levels, and increases in coagulation activation markers) [20, 21, 51].
In recent years, leukoreduction has become increasingly routine in veterinary transfusion medicine, with several studies of the use of various human [17, 26, 31, 32, 33, 34, 35, 36, 37, 38, 52] or veterinary [28, 29, 30] blood collection systems and leukoreduction filters. Nonetheless, few studies focused on leukoreduced plasma and coagulation factor activity [30, 38]. One study examined the PT, aPTT, fibrinogen, and DD concentrations, activity of coagulation factors V, VIII, X, XI, as well as ATA and vWF activity in canine leukoreduced FFP, produced using a veterinary collection and filtration system. The only statistically significant difference between LR‐FPP and non‐leukoreduced FFP included a longer aPTT and lower factor XI activity in the former [30]. Another recent study of canine LR‐FP and non‐LR‐FP produced from non‐precooled WB, employing a human blood collection device and a polyurethane leukocyte filter, similar to the one used in this study showed no significant differences between components in PT, aPTT, activity of coagulation factors V, VII, VIII, X, and XI, fibrinogen concentration and activity of AT and protein C [38]. Differences between results of previous studies possibly occurred due to differences in filter type [20, 24, 53] and WB storage temperature [26, 49, 53] or time‐period [21] prior to leukoreduction. In our study, we used a human leukoreduction system previously used in dogs [27, 34] which proved highly efficient, evident by markedly decreased leukocytes and platelets counts in LR‐WB compared with WB.
In the LR‐FP freezing and partial thawing production process, separation of plasma protein based on their freezing temperature, in theory, separates fibrinogen, FVIII, and vWF into the LR‐CRYO fraction, while other coagulation factors remain, at higher concentrations, in the LR‐CPP component [54]. Our results indicate that the method and the materials used in this study produced the predicted product with partial success, higher FVIII activity in a smaller plasma volume in LR‐CRYO compared with LR‐FP (approximately 60–90 mL compared with 200 mL, respectively) and higher (nearly double), albeit insignificantly, vWF activity and fibrinogen concentration compared with LR‐FP. The level of all these factors was higher in LR‐CRYO and LR‐FP as compared with LR‐CPP. The present results are somewhat similar to previous ones [14], with the advantage of the leukoreduction, although in the previous study vWF activity and fibrinogen concentration were, in fact, significantly higher in CRYO than in FFP and CCP. The absence of a statistically significant increase in LR‐CRYO vWF activity and fibrinogen concentration vs. LR‐FP in our study is possibly due to the small cohort with low statistical power and high individual variability of these factors LR‐CRYO levels, regardless of similar LR‐FP levels. Such high individual variability of fibrinogen concentration and FVIII and vWF activities in canine FPP and in its CRYO product is known in human donors, even between same‐donor samples obtained at different times [55, 56]. Furthermore, a recent study of the impact of hemostatic protein levels on CRYO quality has suggested the latter depends both on specific donor factors and the blood component production techniques used [2].
The use of CPP, though non‐leukoreduced, in dogs was reported in a single previous study focused on its impact on albumin concentration and colloid osmotic pressure in critically ill dogs with hypoalbuminemia [40]. Human CPP has lower levels of vWF, fibrinogen, FVIII, factor XIII, and fibronectin, but similar concentrations of other plasma proteins and clotting factors as the original FPP [3, 57]. CPP is used in place of FFP in human medicine primarily for the treatment of thrombotic thrombocytopenic purpura [58, 59], a condition not reported in dogs. CPP has also been used in human patients instead of FFP for the treatment of generalized peritonitis and disseminated intravascular coagulation associated with pancreonecrosis [60, 61]. In dogs, CPP was used for treating vitamin K antagonist rodenticide toxicity [40], and its effectiveness in that study is supported by our findings that LR‐CPP FX activity is to that of LR‐FP and higher than in LR‐CRYO, warranting further studies.
Hypoalbuminemia is common in various conditions in dogs (e.g., hemorrhage, septic peritonitis, protein‐losing nephropathy, and enteropathy) and is associated with death and poor healing [62, 63, 64]. Species‐specific albumin is the ideal replacement product for treating hypoalbuminemia, but canine‐specific albumin concentrate is unavailable, and therefore, in severe hypoalbuminemia, human serum albumin or synthetic colloids are administered, with their associated risks [65]. An alternative could be FFP, but the large volume of FFP needed to treat hypoalbuminemia can result in volume overload [66]. A recent publication [40] suggests the use of CPP for albumin replacement: our study demonstrated that total protein and albumin concentrations, as measured, were significantly higher in LR‐CPP compared with LR‐FP and LR‐CRYO, and confirms the results obtained on non‐leukoreduced CPP [40]. Therefore, CPP is an effective source of albumin, and thus, although hypoalbuminemia might be treated with canine plasma (fresh or not), CPP should be considered in such cases, in clinical settings where CRYO is routinely produced from FFP.
In this study, ATIII was found in lower concentrations in LR‐CRYO compared with LR‐FP, and this data is in line with what has been reported in some human studies on CRYO [67, 68] but contrasts with an older human study that reported no difference in ATIII content between FFP, CRYO, and CPP [69]. Conversely, it seems that CPP is an adequate ATIII source to be considered in cases of AT consumption and loss (e.g., acute pancreatitis, PLE and PLN).
In regard to clotting times, PT and aPTT values were increased in LR‐CRYO compared with LR‐FP, and these results might be related to the different concentrations of factor X in these products. In fact, factor X deficiency in humans is usually suspected when both plasma PT and aPTT are abnormal [70], and in LR‐CRYO the factor X concentration was significantly lower than in LR‐FP. Nonetheless, in our study, PT is more prolonged in CPP than in FP and CRYO, although FX activity is actually higher in CPP vs. the other components; therefore, the real reasons for this difference in clotting times remain unclear.
In human CRYO, fibrinogen and vWF are stable when refrigerated for 24 h after thawing [71]. A recent study demonstrated that thawed CRYO storage time extension up to 120 h, at either 2°C–6°C or at room temperature, is feasible and maintains FVIII, fibrinogen, and vWF international standard levels, at no risk of potential bacterial contamination [72]. Fibrinogen has been proven stable in CRYO, refrigerated, or stored at room temperature for 35 days after thawing, which nevertheless showed that FVIII and VWF levels decline significantly under both these conditions [73]. Canine and feline coagulation factors, fibrinogen, and vWF were shown to remain stable in FFP subjected to freezing and thawing cycles [74], while an old study in greyhound dogs indicates that CRYO, subjected to freezing and thawing cycles, maintains FVII activities and vWF concentrations similar to those in the original thawed precipitate [15]. The present study similarly confirms that in LR‐CRYO, refrigerated for 24 h or when refrozen for 7 days, all hemostatic analytes measured remained unchanged, excluding ATA, which was significantly lower in refrigerated LR‐CRYO as compared with LR‐CRYO. This decrease in ATA was an unexpected result that cannot be explained in the authors' opinion. Our results regarding the stability of LR‐CRYO suggest that thawed LR‐CRYO, when refrigerated for 24 h or refrozen for up to 7 days, can be efficacious if used for its intended indications, increasing the efficiency of blood component banking.
Finally, in this study, there was no significant difference in hemostatic analytes between refrozen LR‐CRYO bag and refrozen LR‐CRYO transfer tubing, excluding FX activity that was significantly higher, but not clinically significant, in the tubing compared with the bag. This was perhaps due to a more rapid freezing and thawing process in the transfer tubing, warranting further studies to prove this hypothesis. These data are important for future studies regarding refrozen LR‐CRYO long‐term storage, where in such studies a segment of the transfer tubing can be used to measure hemostatic analytes that adequately reflect their levels in the bag (excluding FX activity), avoiding the need to thaw the bag contents.
Despite the attentiveness to the study protocol, this study has some limitations. The major limitation is the limited sample size, which increases the type‐II error probability. The possibility that certain undetected filtration and processing effects did impact the hemostatic analyte results precludes the identification of minor group differences due to the limited sample size. Nonetheless, the present sample size is similar to those in previous veterinary studies of plasma, ranging between 8 and 15 [14, 15, 16].
Another limitation of this study is the failure to determine the hemostatic analytes in LR‐FFP, in addition to LR‐FP. This shortcoming is because no transfer tubing segment was available to measure LR‐FFP analytes prior to its LR‐CRYO production processing. Canine LR‐FPP hemostatic characteristics were reported [30, 38]; however, in the present study, a different filtration was used, and different leukoreduction filter types have different effects on hemostatic analytes [20]. Use of the same filtration system would have allowed a more complete comparison of the current findings of LR‐FFP hemostatic analytes with previous results. Therefore, the present results should be best applied to the specific filter used in this study and should be applied cautiously to other filtering systems. In addition, although some standard veterinary plasma processing protocols for processing exist [75, 76], differences in such protocols might preclude extrapolation of the results of this study to blood products produced following different protocols.
Lastly, this study did not examine the effect of long‐term LR‐CPP storage, warranting future studies. Nevertheless, under standard storage conditions, a LR‐CPP shelf‐life of up to 6 years is recommended by certain blood banks [14].
Conclusions
5
The results of this study support the use of canine LR‐CRYO for FVIII, fibrinogen, and vWF deficiencies, as previously suggested for canine non‐leukoreduced CRYO. The results also suggest that unused LR‐CRYO can be refrozen, stored, and re‐thawed for efficient use. LR‐CPP has high albumin concentration and FX activity, making it suitable for hypoalbuminemic dogs and those in need of FX.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1J. Prittie , “The Role of Cryoprecipitate in Human and Canine Transfusion Medicine,” Journal of Veterinary Emergency and Critical Care 31, no. 2 (2021): 1–11, 10.1111/vec.13034.33751762 · doi ↗ · pubmed ↗
- 2M. Drinkhouse , M. B. Brooks , D. Stefanovski , K. Marryott , and M. B. Callan , “Influence of Canine Donor Plasma Hemostatic Protein Concentration on Quality of Cryoprecipitate,” Journal of Veterinary Internal Medicine 33, no. 1 (2019): 124–131, 10.1111/jvim.15376.30548342 PMC 6335516 · doi ↗ · pubmed ↗
- 3R. L. Sparrow , D. W. Greening , and R. J. Simpson , “A Protocol for the Preparation of Cryoprecipitate and Cryodepleted Plasma,” Methods in Molecular Biology 728 (2011): 259–265, 10.1007/978-1-61779-068-3_17.21468954 · doi ↗ · pubmed ↗
- 4Y. N. L. H. Ching , K. M. Meyers , J. A. Brassard , and K. J. Wardrop , “Effect of Cryoprecipitate and Plasma on Plasma von Willebrand Factor Multimeters and Bleeding Time in Doberman Pinschers With Type‐I von Willebrand's Disease,” American Journal of Veterinary Research 55, no. 1 (1994): 102–110.8141483 · pubmed ↗
- 5R. L. Sparrow , R. J. Simpson , and D. W. Greening , “Preparation of Cryoprecipitate and Cryo‐Depleted Plasma for Proteomic Research Analysis,” Methods in Molecular Biology 2628 (2023): 41–49, 10.1007/978-1-0716-2978-9_4.36781778 · doi ↗ · pubmed ↗
- 6S. F. Idris , A. V. Hadjinicolaou , M. Sweeney , C. Winthrop , G. Balendran , and M. Besser , “The Efficacy and Safety of Cryoprecipitate in the Treatment of Acquired Hypofibrinogenaemia,” British Journal of Haematology 166, no. 3 (2014): 458–461, 10.1111/BJH.12864.24725203 · doi ↗ · pubmed ↗
- 7A. Endo , A. Senda , Y. Otomo , M. Firek , M. Kojima , and R. Coimbra , “Clinical Benefits of Early Concurrent Use of Cryoprecipitate and Plasma Compared With Plasma Only in Bleeding Trauma Patients,” Critical Care Medicine 50, no. 10 (2022): 1477–1485, 10.1097/CCM.0000000000005596.35759689 · doi ↗ · pubmed ↗
- 8T. Stokol and B. W. Parry , “Efficacy of Fresh‐Frozen Plasma and Cryoprecipitate in Dogs With von Willebrand's Disease or Hemophilia A,” Journal of Veterinary Internal Medicine 12, no. 2 (1998): 84–92, 10.1111/j.1939-1676.1998.tb 02100.x.9560764 · doi ↗ · pubmed ↗