Disseminated tuberculosis with rare coccygeal involvement: a case report
Sarra Baziaa, Adil Zegmout, Mohamed Beaouiss, Soufiane El Fathi, Aniss Rafik, Hicham Souhi, Ismail Rhorfi, Hanane El Ouazzani

TL;DR
This case report describes a rare instance of tuberculosis affecting the coccygeal region in a 64-year-old diabetic patient, successfully diagnosed and treated with non-invasive methods.
Contribution
The novelty lies in the rare coccygeal TB localization in an immunocompetent individual, diagnosed non-invasively.
Findings
TB was diagnosed using Xpert MTB/RIF, confirming Mycobacterium tuberculosis infection.
The patient showed complete symptom resolution after starting anti-TB therapy.
The case emphasizes the importance of considering rare TB locations in diagnostic evaluations.
Abstract
Tuberculosis (TB) is a preventable and usually curable disease but remains a major health problem worldwide, particularly in developing countries. TB of the lumbosacral junction is rare and occurs in only 1–2% of all cases of spinal TB. Moreover, isolated sacrococcygeal TB is extremely rare. We present a case of a 64-year-old patient with a history of diabetes who presented with chronic back pain and cough. Physical examinations revealed a perianal fistula and left elbow joint arthritis. The patient is diagnosed with disseminated TB with coccygeal involvement. Diagnosis was achieved non-invasively using Xpert MTB/RIF, confirming Mycobacterium tuberculosis infection. The patient experienced complete resolution of symptoms following the commencement of anti-TB therapy. We highlight the importance of this case due to the rare coccygeal localization of TB in an immunocompetent patient,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
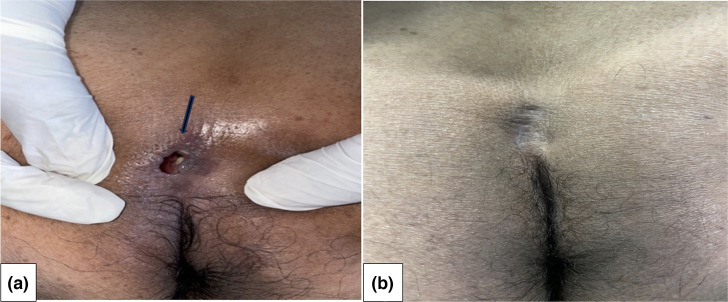 Fig. 1
Fig. 1 Fig. 2
Fig. 2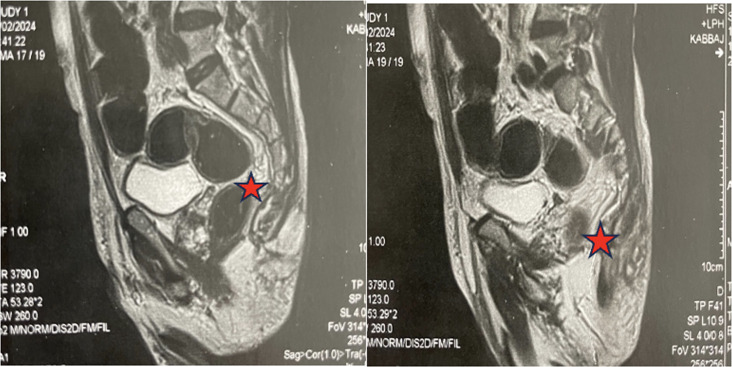 Fig. 3
Fig. 3 Fig. 4
Fig. 4| Author | Country | Age | Gender | Presence of perianal discharge | Pulmonaryinvolvement | Diagnostic method |
|---|---|---|---|---|---|---|
| Thilakaranthe | Sri Lanka | 47 | F | Yes | No | Biopsy under exploration of post-anal space |
| Kim | Korea | 35 | M | No | No | CT guided biopsy |
| Singh | India | 20 | F | No | No | Needle biopsy |
| Osman | Tunisia | 55 | F | No | No | Surgery |
| Takakura | Japan | 93 | M | Yes | No | Bacterial examination of fistula discharge |
| Kumar | India | 42 | F | Yes | No | Biopsy |
| Gadi | India | 23 | F | No | No | CT guided biopsy |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfectious Diseases and Tuberculosis · Diagnosis and treatment of tuberculosis · Tuberculosis Research and Epidemiology
Data Summary
No data were generated during this research or are required for the work to be produced.
Introduction
Each year over 10 million people still fall ill with tuberculosis (TB) [1]. TB is an infectious disease caused by the bacterium Mycobacterium tuberculosis. While it primarily affects the lungs, leading to pulmonary TB, the infection can disseminate beyond the lungs through haematogenous and lymphatic spread, resulting in extrapulmonary tuberculosis (EPTB). EPTB refers to TB that affects organs other than the lungs. Around 15–25% of TB cases affect extrapulmonary sites, leading to EPTB through the haematogenous and lymphatic spread of M. tuberculosis. The most common sites of EPTB include the pleura, lymphatic system and osteoarticular structures [2].
Clinically, EPTB often goes underrecognized, with diagnoses frequently delayed due to its paucibacillary nature and atypical presentations. Factors such as Human Immunodeficiency Virus (HIV) infection and female gender have been identified as significant risk factors for the spread of EPTB. Diabetes is another critical factor, as multiple studies have shown it to be associated with a higher risk of developing active TB. Moreover, patients with diabetes have a greater risk of developing EPTB compared to pulmonary TB [3].
Disseminated TB is defined as a tuberculous infection involving the bloodstream, bone marrow, liver or two or more non-contiguous sites, or miliary TB. The symptoms are non-specific, and the duration of symptoms before diagnosis is variable.
Disseminated TB is a rare condition defined by the involvement of two extrapulmonary sites, with or without associated pulmonary involvement.
Osteoarticular TB represents between 1 and 3% of TB cases, with variable incidence in endemic and non-endemic areas of the world [4]. The lower thoracic and lumbar spine are the most common sites for spinal TB, whether it originates primarily or as a result of pulmonary TB. In contrast, infection of the lumbosacral junction is quite rare, occurring in only 1–2% of all spinal TB cases [5].
Here, we report a unique case of disseminated TB with rare sacrococcygeal involvement.
Case report
A 64-year-old male patient presented with a 3-month history of persistent cough and severe back pain. The clinical history was notable for prolonged fever and significant weight loss. The patient had a history of type 2 diabetes; he did not have any past history of TB or any contact with another patient diagnosed with TB.
The physical examination revealed a perianal fistula with purulent discharge (Fig. 1). The motor and sensory examination of the lower limbs was normal and there was no bowel or bladder incontinence. Osteoarticular examination found left elbow arthritis. The rest of the clinical examination was unremarkable.
(a) Perianal fistula (see arrow) and (b) after 2 months of treatment.
A thoracic, abdominal and pelvic computed tomography (CT) scan revealed a consolidation of the left upper right lobe with a cavity (Fig. 2), lysis of the D3-K3 costo-vertebral joint and the presence of coccygeal arthritis. Magnetic resonance imaging (MRI) of the lumbosacral spine demonstrates a complex lesion centred in the left median and paramedian retro-rectal space, extending into the pericoccygeal region. The lesion is enhanced in its periphery after gadolinium administration, and there is soft tissue involvement as well (Fig. 3). A CT scan of the elbow revealed a joint effusion with severe osteopenia (Fig. 4).
Chest CT scan shows consolidation with excavation (see arrow) in the right upper lobe.
Pelvic MRI shows a pericoccygeal collection with soft tissue involvement and a fistulous tract.
Blood tests showed elevation in C reactive protein level with normal blood cells. HBA1C=7%. He tested negative for HIV. The acid-fast bacilli (AFB) test performed on sputum and fistula discharge was positive. Additionally, the GeneXpert MTB/RIF assay conducted on sputum, fistula discharge and elbow joint fluid showed positive for M. tuberculosis.
We retained the diagnosis of multifocal TB with pulmonary and osteoarticular involvement of the left elbow and sacrococcygeal region, which is rare.
Antibacillary chemotherapy was started for 9 months. He was treated with rifampicin, isoniazid, ethambutol and pyrazinamide for 2 months, followed by rifampicin and isoniazid for 7 months, according to the recommendations of the national TB control programme in Morocco. There was no indication for surgical intervention. The patients' pain resolved and the purulent drainage stopped within the second month of treatment.
Discussion
TB remains a global health concern posing significant challenges to both clinicians and radiologists due to its diverse and often non-specific clinical manifestations. Elbow TB is rare; its incidence varies from 2 to 5% of all skeletal locations [6].
In addition, TB infection of the lumbosacral junction is also quite rare, accounting for only 1–2% of all spinal TB cases [5]. Multifocal TB is defined by the occurrence of TB lesions in multiple locations across different adjacent or distant organs. Multifocal TB commonly occurs in immunocompromised patients, who differ from immunocompetent individuals in terms of clinical presentation, radiological features, laboratory findings and treatment outcomes, often leading to misdiagnosis [7].
We report a case of multifocal TB with atypical and rare localizations including the left elbow and sacrococcygeal joint. We were able to confirm our diagnosis at all sites using the GenXpert MTB/RIF test on the joint fluid, fistula discharge and sputum samples. Our patient is immunocompetent and has a history of well-controlled diabetes.
The diagnosis of EPTB can be challenging because of the diverse clinical presentations that mimic other medical conditions. Our patient reported initially elbow joint pain and back pain. Clinical manifestations of sacral TB depend primarily on patient age. Young individuals tend to present with discharging sinuses and abscesses, whereas backache is a dominant clinical feature in adults. Due to the protection provided by the sacral bone to the nerve roots, neurological symptoms in sacral TB are relatively uncommon [5]. Indeed, our patient does not present with any neurological symptoms, and the clinical examination shows no motor deficits or sensory dysfunction.
Only a few cases of coccygeal TB have been reported in the literature (see Table 1), and only three of them presented with sinus discharges. Concomitant active pulmonary TB is observed in around 50% of spine TB cases [8]. Our patient had active pulmonary TB as well with a positive AFB examination of the sputum.
The usefulness of the GeneXpert MTB/RIF test is worth emphasizing due to its less invasive nature and high specificity for TB. The specificity of Xpert MTB/RIF for detecting TB is 99% [9].
Most cases of coccygeal TB have been diagnosed through invasive procedures such as biopsies or surgery, likely due to clinical presentations that often suggest alternative diagnoses, particularly malignancies. In our case, we confirmed the presence of * M. tuberculosis* using a rapid and non-invasive technique through PCR testing on various samples. The combination of immune, behavioural, anatomical and environmental factors likely contributed to the difference in presentation between our male patient and previously reported female cases. This unique presentation highlights the need for individualized consideration in the diagnosis and management of multifocal TB.
Conclusion
Multifocal TB is an uncommon presentation of a disease that predominantly affects immunocompromised individuals. Our case, involving the rare combination of the elbow joint and sacrococcygeal region, highlights the diverse and atypical manifestations of this condition, emphasizing the importance of maintaining a high index of suspicion in unusual presentations. The use of molecular diagnostic tools such as GeneXpert played a pivotal role in confirming the diagnosis promptly, facilitating targeted treatment and improving the patient’s prognosis.
Left elbow CT scan shows joint effusion and severe osteopenia.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization Global Tuberculosis Report 2024 https://www.who.int/teams/global-tuberculosis-programme/tb-reportsaccessed 7-July-2024
- 2Fang Y Zhou Q Li L Zhou Y Sha W Epidemiological characteristics of extrapulmonary tuberculosis patients with or without pulmonary tuberculosis Epidemiol Infect 2022150 e 15810.1017/S 095026882200123635904011 PMC 9472030 · doi ↗ · pubmed ↗
- 3Qian X Nguyen DT Lyu J Albers AE Bi X et al Risk factors for extrapulmonary dissemination of tuberculosis and associated mortality during treatment for extrapulmonary tuberculosis Emerg Microbes Infect 2018710210.1038/s 41426-018-0106-129872046 PMC 5988830 · doi ↗ · pubmed ↗
- 4Agashe VM Johari AN Shah M Anjum R Romano C et al Diagnosis of Osteoarticular Tuberculosis: Perceptions Protocols, Practices, and Priorities in the Endemic and Non-Endemic Areas of the World—A WAIOT View. Microorganismsvol 8p 131210.3390/microorganisms 8091312 PMC 756338832872175 · doi ↗ · pubmed ↗
- 5Kim DU Kim SW Ju CI Isolated coccygeal tuberculosis J Korean Neurosurg Soc 20125249549710.3340/jkns.2012.52.5.49523323174 PMC 3539088 · doi ↗ · pubmed ↗
- 6Dhillon MS Goel A Prabhakar S Aggarwal S Bachhal V Tuberculosis of the elbow: a clinicoradiological analysis Indian J Orthop 20124620020510.4103/0019-5413.9368422448059 PMC 3308662 · doi ↗ · pubmed ↗
- 7Shao C Qu J He L A comparative study of clinical manifestations caused by tuberculosis in immunocompromised and non-immunocompromised patients Chinede Medical Journal 20031161717172210.3760/cma.j.issn.0366-6999.2003.11.11714642144 · doi ↗ · pubmed ↗
- 8Takakura Y Fujimori M Okugawa K Egi H Ohdan H et al Rare case of sacrococcygeal tuberculosis mimicking as an anal fistula Int J Surg Case Rep 201849747710.1016/j.ijscr.2018.05.03329966953 PMC 6039961 · doi ↗ · pubmed ↗