Safety of Vancomycin Use Through Midline Catheters for Outpatient Parenteral Antimicrobial Therapy
David Paje, Emily Walzl, Megan Heath, Elizabeth McLaughlin, Jennifer K. Horowitz, Caitlin Tatarcuk, Lakshmi Swaminathan, Scott Kaatz, Anurag N. Malani, Ashwin Gupta, Valerie M. Vaughn, Steven J. Bernstein, Scott A. Flanders, Vineet Chopra

TL;DR
This study investigates whether using vancomycin through midline catheters in outpatient settings causes device-related complications.
Contribution
The study provides new evidence on the safety of administering vancomycin via midline catheters in outpatient care.
Findings
Vancomycin use through midline catheters was not significantly associated with increased device-related complications.
Patients receiving vancomycin via midline catheters had similar complication rates to those on other antimicrobials.
Abstract
This cohort study examines the association between vancomycin use through midline catheters and device-related complications among patients receiving outpatient parenteral antimicrobial therapy.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure
Figure| Outcomes | Total No. (No. per 1000 catheter-days) | Adjusted HR (95% CI) | |||
|---|---|---|---|---|---|
| Total (N = 3317) | Vancomycin (n = 597) | No vancomycin (n = 2720) | |||
| Any major complication | 49 (1.10) | 27 (3.27) | 22 (0.61) | 4.82 (2.64-8.83) | <.001 |
| Catheter-related BSI | 22 (0.49) | 15 (1.82) | 7 (0.19) | 8.00 (2.96-21.63) | <.001 |
| Catheter-related VTE | 27 (0.61) | 12 (1.45) | 15 (0.41) | 3.30 (1.52-7.16) | .003 |
| Upper extremity DVT | 20 (0.45) | 7 (0.85) | 13 (0.36) | 1.51 (0.64-3.58) | .35 |
| Pulmonary embolism | 7 (0.16) | 5 (0.61) | 2 (0.06) | NA | NA |
| Any minor complication | 379 (8.50) | 92 (11.14) | 287 (7.90) | 1.47 (1.14-1.90) | .003 |
| Catheter dislodgement | 123 (2.76) | 26 (3.15) | 97 (2.67) | 1.14 (0.69-1.86) | .61 |
| Catheter occlusion | 89 (2.00) | 22 (2.66) | 67 (1.84) | 1.69 (0.94-3.02) | .08 |
| Catheter tip migration | 40 (0.90) | 11 (1.33) | 29 (0.80) | 1.74 (0.83-3.69) | .15 |
| Infiltration | 23 (0.52) | 10 (1.21) | 13 (0.36) | 3.92 (1.70-9.03) | .001 |
| Superficial thrombosis | 30 (0.67) | 6 (0.73) | 24 (0.66) | 1.48 (0.58-3.77) | .42 |
| Exit site concerns | 146 (3.28) | 40 (4.84) | 106 (2.92) | 1.81 (1.22-2.70) | .003 |
| Any major or minor complication | 410 (9.20) | 110 (13.32) | 300 (8.26) | 1.67 (1.32-2.11) | <.001 |
| Device failure | 362 (8.12) | 101 (12.23) | 261 (7.19) | 1.75 (1.36-2.25) | <.001 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntibiotics Pharmacokinetics and Efficacy · Central Venous Catheters and Hemodialysis · Anesthesia and Sedative Agents
Midline catheters are alternatives to peripherally inserted central catheters for outpatient parenteral antimicrobial therapy (OPAT).^1^ Current guidelines recommend against using midline catheters for extended treatment with vancomycin due to its irritant and vesicant properties.^2,3^ However, evidence supporting this recommendation is limited, and whether such practice is prevalent or harmful remains unknown. We analyzed data from the Michigan Hospital Medicine Safety Consortium (HMS) to assess device-related complications among hospitalized patients receiving OPAT with and without vancomycin therapy.
Methods
We used data from hospitalized patients who received midline catheters between January 2017 and August 2024. We excluded patients who received their device in critical care settings and included patients who received antimicrobials through a midline catheter after hospital discharge.^1^ Patients were followed up until device removal, death, or 30 days from device insertion. This study was classified as not regulated by University of Michigan’s Institutional Review Board; informed consent was waived because all data were deidentified. This study followed the STROBE reporting guideline.
The primary outcome was a major device complication, including catheter-related bloodstream infection (CRBSI) and catheter-related venous thromboembolism (CR-VTE). Secondary outcomes included device failure, defined as premature removal of midline catheter due to any complication as described.^1^ We assessed associations between receipt of vancomycin and outcomes using Fine-Gray hazards models, accounting for dwell time and risk of competing event of device removal from other device complications, adjusting for patient and device characteristics.^4^ Adjusted hazard ratios (aHRs) with 95% CIs were calculated using SAS version 9.4 (SAS Institute). All tests were 2-tailed, and P < .05 was considered statistically significant (eMethods in Supplement 1).
Results
Among 3317 patients prescribed OPAT through midline catheters, the median (IQR) age was 67.5 (56.1-77.6) years; 1678 (51.5) were male and 1639 (49.4%) were female. A total of 597 (18.0%) received vancomycin, whereas 2720 (82.0%) did not. OPAT duration (median [IQR], 11 [7-17] vs 11 [7-16] days; P = .33), catheter dwell time (median [IQR], 12.0 [8.0-19.0] vs 12.0 [8.0-17.0] days; P = .14), and consultation with infectious diseases (ID) specialists (84.9% vs 82.8%; P = .22) were similar between both groups.
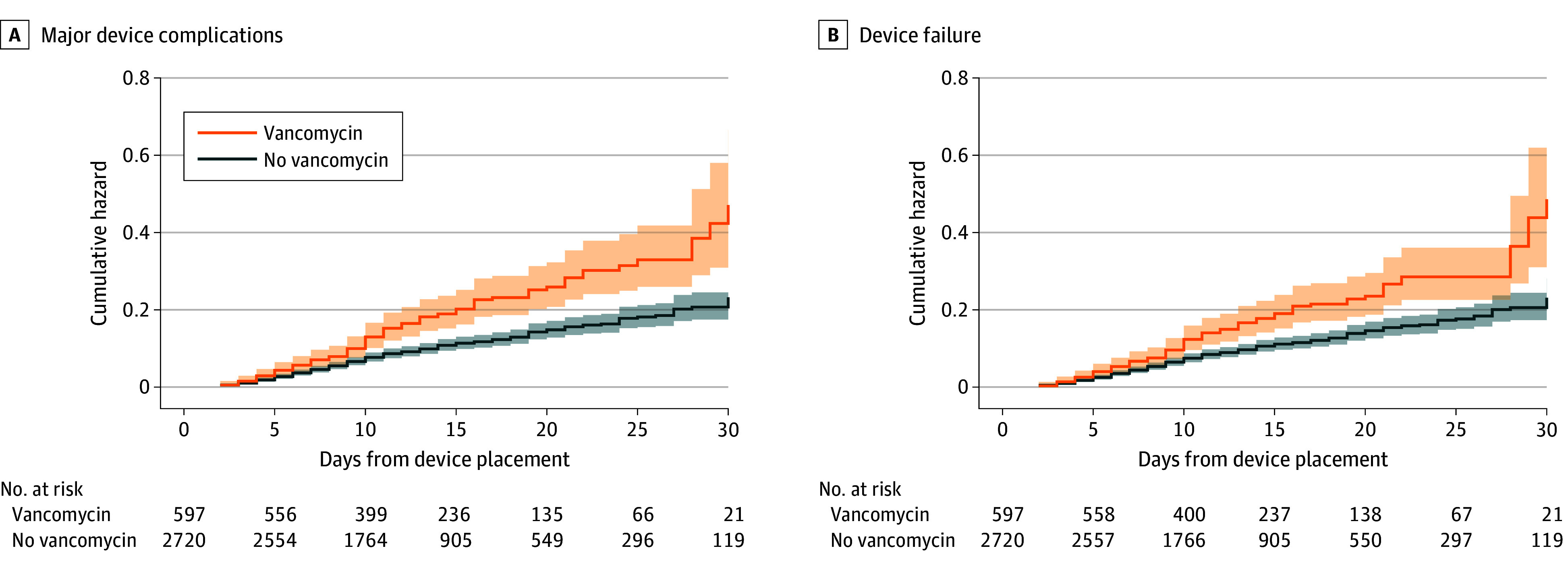
Major device complications occurred in 49 (1.5%) of 3317 patients in the overall cohort, including 27 (4.5%) of 597 vancomycin recipients vs 22 (0.8%) of 2720 nonrecipients (P < .001). Vancomycin recipients had higher rates of CRBSI (2.5% vs 0.3%; P < .001) and CR-VTE (2.0% vs 0.6%; P < .001) than nonrecipients. Device failure was more prevalent among vancomycin recipients than nonrecipients (16.9% vs 9.6%; P < .001). In adjusted analyses, vancomycin administration through a midline catheter was associated with a higher hazard of major device complications (aHR, 4.82; 95% CI, 2.64-8.83) and device failure (aHR, 1.75; 95% CI, 1.36-2.25; Table; Figure). Vancomycin was also associated with higher risks of CRBSI (aHR, 8.00; 95% CI, 2.96-21.63) and CR-VTE (aHR, 3.30; 95% CI, 1.52-7.16). Results were robust to sensitivity analyses, including patients discharged home (vs facility) and patients who received vancomycin monotherapy.
Cumulative Hazard Curves of Patients Receiving Outpatient Parenteral Antimicrobial Therapy (OPAT) Through Midline Catheters, by Receipt of VancomycinShaded areas represent 95% CIs.
Discussion
In this multicenter study of patients discharged with midline catheters for OPAT, vancomycin infusion was associated with higher risk of major device complications and premature catheter removal. Major device complications were 5 times more likely among vancomycin recipients than nonrecipients, arising from an 8-fold greater risk of CRBSI and 3-fold greater risk of CR-VTE. Our findings support current recommendations against using midline catheters for vancomycin infusion.^2^ However, nearly 1 in 5 midline catheters in our cohort were used for vancomycin-based OPAT, and 4 of 5 recipients were seen by an ID specialist before device placement. Study limitations included its observational design, secondary use of medical records, and lack of information regarding events after midline catheter removal.
These findings highlight opportunities for practice improvement, especially given widespread availability of intravenous and oral alternatives to vancomycin.^5,6^ They also underscore the importance of infusate compatibility in ensuring the safety and reliability of midline catheters. Collaboration among vascular access teams, ID specialists, pharmacists, and ambulatory infusion nurses is necessary to optimize practice and prevent harm from using midline catheters for vancomycin-based OPAT.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Paje D, Walzl E, Heath M, . Midline vs peripherally inserted central catheter for outpatient parenteral antimicrobial therapy. JAMA Intern Med. 2025;185(1):83-91. doi:10.1001/jamainternmed.2024.5984 39527077 PMC 11555572 · doi ↗ · pubmed ↗
- 2Nickel B, Gorski L, Kleidon T, . Infusion therapy standards of practice, 9th edition. J Infus Nurs. 2024;47(1S)(suppl 1):S 1-S 285. doi:10.1097/NAN.000000000000053238211609 · doi ↗ · pubmed ↗
- 3Scarano M, D’Arrigo S, De Letteriis S, Grasso S, Pittiruti M, Scoppettuolo G. Risk of thrombophlebitis associated with continuous peripheral infusion of vancomycin: the effect of dilution. J Vasc Access. 2024;25(1):107-112. doi:10.1177/11297298221095778 35608270 · doi ↗ · pubmed ↗
- 4Fine JP, Gray RJ. A proportional hazards model for the subdistribution of a competing risk. J Am Stat Assoc. 1999;94(446):496-509. doi:10.1080/01621459.1999.10474144 · doi ↗
- 5Kawasuji H, Nagaoka K, Tsuji Y, . Effectiveness and safety of linezolid versus vancomycin, teicoplanin, or daptomycin against methicillin-resistant Staphylococcus aureus bacteremia: a systematic review and meta-analysis. Antibiotics (Basel). 2023;12(4):697. doi:10.3390/antibiotics 12040697 37107059 PMC 10135165 · doi ↗ · pubmed ↗
- 6Kato H, Hagihara M, Asai N, . Meta-analysis of vancomycin versus linezolid in pneumonia with proven methicillin-resistant Staphylococcus aureus. J Glob Antimicrob Resist. 2021;24:98-105. doi:10.1016/j.jgar.2020.12.009 33401013 · doi ↗ · pubmed ↗