Uterine Spindle Cell Sarcoma Presenting With Lower Gastrointestinal Bleeding: A Case Report
Ahmad Habbas, Ismail Althunibat, Shatha Elemian, Byron Okwesili, Abdul Aishat Abiola, Laith Sorour, Amro Al Radaideh, Andre Fedida

TL;DR
A rare case of uterine spindle cell sarcoma presented as lower gastrointestinal bleeding in an elderly woman, highlighting unusual symptoms of this aggressive cancer.
Contribution
This case report adds to the limited literature on uterine spindle cell sarcoma presenting with atypical gastrointestinal symptoms.
Findings
A 79-year-old woman presented with lower GI bleeding, constipation, and weight loss due to uterine spindle cell sarcoma.
Colonoscopy revealed an ulcerated mass in the sigmoid colon, confirmed as high-grade spindle cell sarcoma via biopsy.
The mass was unresectable, leading to chemotherapy as the primary treatment.
Abstract
This case report presents a rare clinical manifestation of uterine spindle cell sarcoma, an aggressive and uncommon malignancy, in a 79-year-old female patient. The patient presented with lower gastrointestinal (GI) bleeding, constipation, and significant weight loss. Colonoscopy identified an infiltrative, ulcerated mass within the sigmoid colon, later confirmed by biopsy as a high-grade spindle cell sarcoma of uterine origin. Given the unresectable status of the mass, chemotherapy was initiated as the primary treatment. This report discusses the diagnostic challenges and highlights the importance of considering atypical presentations in patients with lower GI bleeding and weight loss.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
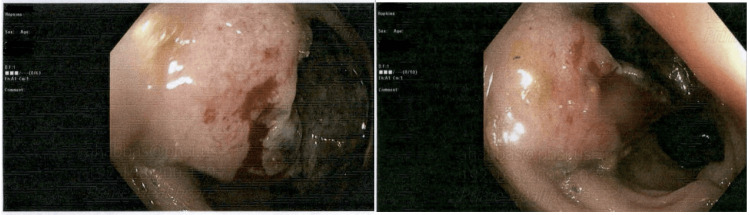 Figure 1
Figure 1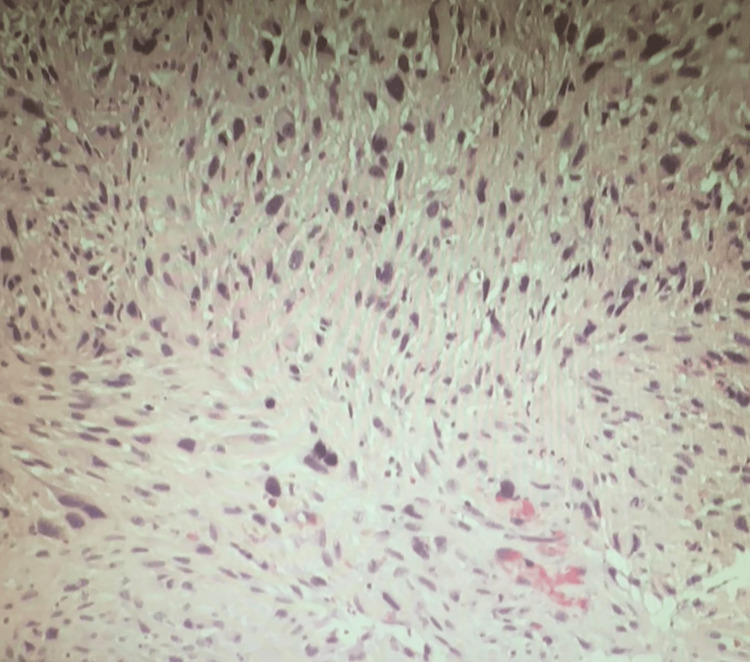 Figure 2
Figure 2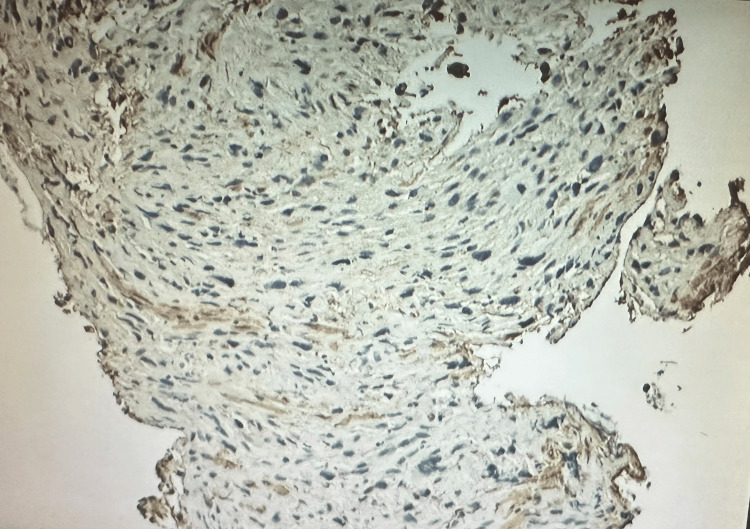 Figure 3
Figure 3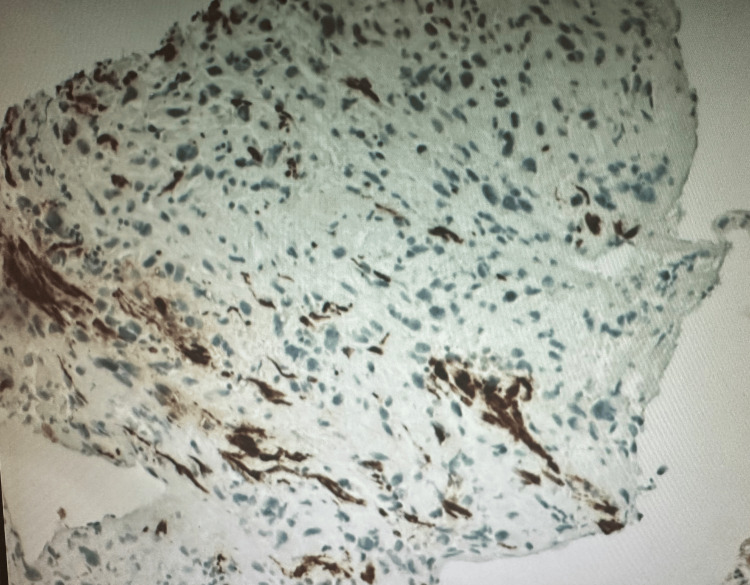 Figure 4
Figure 4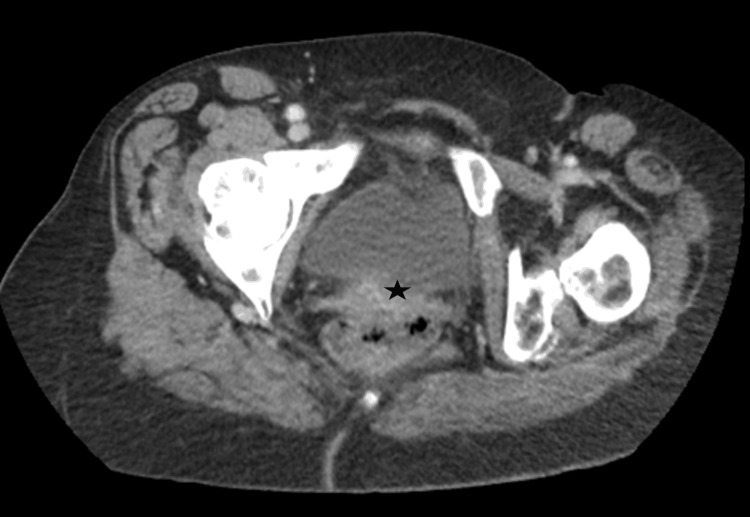 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsUterine Myomas and Treatments · Endometrial and Cervical Cancer Treatments · Sarcoma Diagnosis and Treatment
Introduction
Uterine sarcomas are uncommon malignancies, comprising less than 1% of all uterine cancers, with an estimated annual incidence of 0.36 to 0.64 cases per 100,000 women [1]. They are categorized into several histological subtypes, including leiomyosarcoma, endometrial stromal sarcoma (ESS), and undifferentiated uterine sarcoma (UUS) [2]. Spindle cell variants are particularly aggressive, with a tendency for early local invasion and metastasis.
The current World Health Organization classification recognizes four categories of endometrial stromal tumor: endometrial stromal nodule (ESN), low-grade endometrial stromal sarcoma (LG-ESS), high-grade endometrial stromal sarcoma (HG-ESS), and UUS [3]. Clinical manifestations often overlap with benign gynecological conditions, including abnormal uterine bleeding, pelvic pain, or rapidly enlarging uterine masses [4].
This case report documents an unusual presentation of uterine spindle cell sarcoma with lower gastrointestinal (GI) bleeding and discusses the challenges of diagnosis and management.
Case presentation
A 79-year-old woman with a past medical history of hypertension and paroxysmal atrial fibrillation presented to the gastroenterology clinic with a six-month history of intermittent lower GI bleeding, constipation, weight loss, and generalized fatigue. Her symptoms had worsened recently, prompting a referral for further evaluation.
Colonoscopy showed a fungating, infiltrative, and ulcerated mass in the sigmoid colon (Figure 1), approximately 26 cm from the anal verge. The lesion was partially circumferential, involving one-third of the luminal circumference without causing obstruction. Biopsies were obtained.
Colonoscopy images showing a fungating, infiltrative, and ulcerated mass in the sigmoid colon
Histopathology and immunohistochemistry
Biopsy analysis showed a high-grade, poorly differentiated spindle cell malignant neoplasm with features suggestive of sarcoma. Tumor cells infiltrated benign colonic mucosa (Figure 2). Immunohistochemical staining showed positivity for GATA3, PAX8 (weak to moderate), beta-catenin (nuclear expression), MDM2 (some positive cells), and calretinin. The tumor displayed limited expression of smooth muscle actin (SMA) (Figure 3), desmin (Figure 4), WT1, synaptophysin, p40, and p16, with negativity for CK20, CDX2, and BAP1. This immunohistochemical profile supported the diagnosis of uterine sarcoma with spindle cell morphology.
H&E-stained tissue section showing high-grade malignant tumor spindle cells infiltrating benign colonic mucosaH&E: Hematoxylin and eosin
Positive focal SMA stain from the obtained tissue SMA: Smooth muscle actin
Positive focal desmin stain from the obtained tissue
Imaging
A contrast-enhanced CT scan of the abdomen and pelvis revealed a large pelvic mass, likely a conglomeration of the abnormal sigmoid colon and uterus, with possible fistulous communication (Figure 5). The mass compressed the left ureter, resulting in moderate hydronephrosis, and a 2.3 cm indeterminate nodule was noted on the right adrenal gland. No regional lymphadenopathy or definitive signs of distant metastasis were observed.
Enlarged pelvic mass invading the sigmoid colon with possible fistulous communicationThe star represents the uterine mass invading the rectum with possible fistula formation.
Diagnosis
The diagnosis made was high-grade uterine spindle cell sarcoma with local invasion into the sigmoid colon.
Therapeutic intervention
After multidisciplinary consultation, including gynecology and oncology, the tumor was deemed unresectable due to its local invasion and complex anatomy. Chemotherapy was initiated as the primary mode of management, aiming to control tumor progression, alleviate symptoms, and improve the patient’s quality of life.
Discussion
Uterine sarcomas are relatively rare, accounting for fewer than 5% of all uterine malignancies, yet they remain among the most aggressive gynecologic tumors due to their high risk of recurrence and poor overall survival rates [5]. Among these, spindle cell sarcomas represent a particularly uncommon subtype marked by rapid growth, early metastasis, and significant diagnostic challenges [6]. While patients classically present with gynecologic symptoms such as abnormal uterine bleeding or pelvic pain, atypical manifestations - including lower GI bleeding - can occur if the tumor invades or extends into surrounding structures, such as the sigmoid colon in this case.
Histopathological and immunohistochemical evaluations are crucial for distinguishing uterine spindle cell sarcomas from other spindle cell neoplasms in the GI tract, as the morphological overlap can be substantial [5,7]. Markers indicative of Müllerian origin - such as PAX8 and GATA3 - are key to confirming a uterine primary, particularly when the lesion appears in an unusual location. In this patient, the tumor’s extension into the sigmoid colon and the presenting symptom of lower GI bleeding highlight the potential for uterine sarcomas to manifest similarly to primary colorectal tumors, complicating and potentially delaying the diagnostic process.
Imaging modalities, including CT and MRI, play a vital role in defining the anatomic extent of the disease and evaluating resectability [7]. In advanced cases with significant local invasion, such as the one described, primary surgical management may not be feasible. Instead, chemotherapy becomes the mainstay of treatment, aiming to control tumor progression and provide palliation [8]. However, the prognosis for high-grade uterine sarcomas remains guarded, and the response to conventional chemotherapy is variable.
As this case demonstrates, an older patient presenting with GI symptoms, especially unexplained bleeding and weight loss, warrants a broad differential diagnosis that includes gynecological malignancies, even when the initial findings point to a GI source. Prompt recognition, multidisciplinary evaluation, and the integration of pathology, imaging, and immunohistochemistry are essential to ensuring accurate diagnosis and effective management. Future investigations into novel therapeutic targets and personalized treatment regimens are critical, given the limited efficacy of standard therapies in advanced uterine sarcomas [6,8].
Conclusions
This case emphasizes the diagnostic challenges associated with high-grade uterine spindle cell sarcomas presenting with non-gynecologic symptoms such as lower GI bleeding. The patient’s course highlights the need for a high index of suspicion and comprehensive workup in older patients with atypical GI presentations. Continued research is essential to improve therapeutic outcomes in this aggressive malignancy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Uterine sarcomas: a review Gynecol Oncol D'Angelo E Prat J 13113911620101985389810.1016/j.ygyno.2009.09.023 · doi ↗ · pubmed ↗
- 2Sarcoma of the uterus. Guideline of the DGGG (S 2k-level, AWMF registry no. 015/074, August 2015)Geburtshilfe Frauenheilkd Denschlag D Thiel FC Ackermann S 102810427520152664029310.1055/s-0035-1558120 PMC 4651298 · doi ↗ · pubmed ↗
- 3Endometrial stromal tumors: the new WHO classification Adv Anat Pathol Conklin CM Longacre TA 3833932120142529930810.1097/PAP.0000000000000046 · doi ↗ · pubmed ↗
- 4Uterine endometrial stromal tumors with pure low-grade morphology harboring YWHAE::NUTM 2 fusions: report of a case series emphasizing potential for high-grade transformation and aggressive behavior Am J Surg Pathol Devins KM Attygalle AD Croce S Vroobel K Oliva E Mc Cluggage WG 7177244720233703255510.1097/PAS.0000000000002041 · doi ↗ · pubmed ↗
- 5Endometrial stromal tumors: a clinico-histomorphological spectrum of endometrial stromal tumors with review of literature J Cancer Res Ther Verma A Tomar R Chaturvedi A Dhankar N Mallya V Khurana N 1501552020243855431310.4103/jcrt.jcrt_741_22 · doi ↗ · pubmed ↗
- 6Uterine sarcomas: clinical practice guidelines for diagnosis, treatment, and follow-up, by Spanish group for research on sarcomas (GEIS)Ther Adv Med Oncol Pérez-Fidalgo JA Ortega E Ponce J 15202310.1177/17588359231157645 PMC 1005260737007636 · doi ↗ · pubmed ↗
- 7Uterine sarcomas Int J Gynaecol Obstet Mbatani N Olawaiye AB Prat J 515814320183030657710.1002/ijgo.12613 · doi ↗ · pubmed ↗
- 8Current status of the adjuvant therapy in uterine sarcoma: a literature review World J Clin Cases Rizzo A Pantaleo MA Saponara M Nannini M 17531763720193141792110.12998/wjcc.v 7.i 14.1753 PMC 6692269 · doi ↗ · pubmed ↗