Successful Vaginal Delivery Enabled by Continuous Epidural Analgesia for Cancer-Related Pain in Pregnancy: A Case Report
Risa Miyazaki, Megumi Kanao-Kanda, Toshiyuki Kuriyama, Sarah K Luthe, Tomoyuki Kawamata

TL;DR
A pregnant woman with cancer-related pain successfully delivered vaginally using continuous epidural analgesia, avoiding risky systemic pain medications.
Contribution
This case report demonstrates the safe use of continuous epidural analgesia for managing cancer-related pain during pregnancy.
Findings
Continuous epidural analgesia allowed the patient to maintain optimal labor positioning and achieve vaginal delivery.
Postpartum pain was effectively managed with oral opioids without fetal risks.
The approach enabled timely initiation of oncologic treatment after delivery.
Abstract
Managing cancer-related pain during pregnancy presents a significant clinical challenge due to the limited use of systemic analgesics, such as opioids and nonsteroidal anti-inflammatory drugs (NSAIDs), owing to the potential risks to the fetus. Severe cancer-related pain may impair a parturient’s ability to assume or maintain an optimal labor positioning during labor and delivery, potentially precluding vaginal delivery. In June 2019, a 32-year-old pregnant woman with synovial sarcoma developed intractable gluteal pain that impaired her ability to assume an appropriate delivery position. Given the concerns regarding the use of systemic opioids and NSAIDs, continuous lumbar epidural analgesia was initiated at 34 weeks' gestation to manage cancer-related pain. This approach enabled the patient to tolerate labor positioning, leading to successful vaginal delivery with minimal discomfort.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
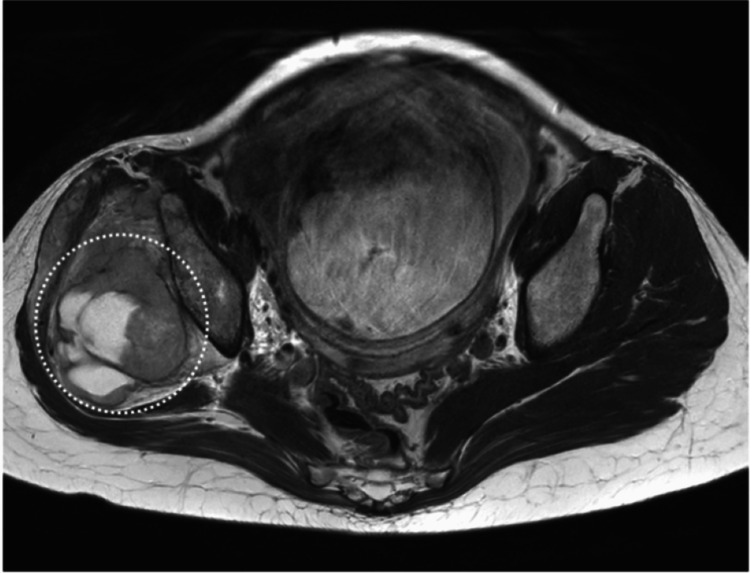 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAnesthesia and Pain Management · Pregnancy-related medical research · Pain Management and Opioid Use
Introduction
Severe cancer-related pain during pregnancy can interfere with labor positioning, posing a challenge to achieving vaginal delivery. Systemic analgesics such as opioids and nonsteroidal anti-inflammatory drugs (NSAIDs) are often avoided due to potential adverse fetal effects [1]. Opioids have been associated with neonatal oversedation, respiratory depression, and withdrawal syndrome [2,3], while NSAIDs may cause premature closure of the ductus arteriosus, fetal renal impairment, and delayed labor [4]. Consequently, alternative strategies for pain management are warranted. Here, we present a case in which epidural analgesia provided effective pain relief in a patient with synovial sarcoma during pregnancy, allowing for vaginal delivery while avoiding systemic analgesics.
Case presentation
A 32-year-old pregnant woman with a history of Kawasaki disease presented with right gluteal pain radiating to the lateral thigh, which had been present for two years. The patient had experienced two pregnancies, including one prior successful vaginal delivery, classifying her as a multipara. As the pain was mild and did not interfere with daily activities, the cause of the pain was not investigated until 31 weeks' gestation, when the pain significantly worsened. The pain was initially managed with acetaminophen 2400 mg/day. MRI revealed a tumor involving her right femoral head, and biopsy confirmed the diagnosis of synovial sarcoma (Figure 1).
T2-weighted MRI obtained at admissionMRI scan showing a large synovial sarcoma (white dotted circle) in the right gluteal region with involvement of adjacent soft tissues.
Due to the urgency of initiating oncologic treatment, labor induction was scheduled at 35 weeks’ gestation.
On June 17, 2019 (at 34 weeks and six days’ gestation), the patient presented with severe, electric shock-like pain in the right L1-4 region, rated 8/10 on the Numerical Rating Scale (NRS), which interfered with sleep, ambulation, and the ability to assume the lithotomy position, the optimal delivery position in her case. An epidural catheter was placed for pain management at the L3/4 interspace. A test dose of 3 mL of 2% lidocaine with epinephrine was administered to confirm catheter placement, resulting in sensory blockade of the L2-4 dermatomes and reducing pain to an NRS of 4/10. Continuous epidural analgesia was initiated using a mixture of 0.8 mg fentanyl, 142 mL of 0.25% levobupivacaine, and 142 mL of normal saline, infused at 5 mL/h.
On June 18, 2019, the patient developed numbness in the left lower extremity, prompting a reduction of the infusion rate to 3 mL/h. Spontaneous labor commenced and was augmented with oxytocin. The patient subsequently delivered vaginally with minimal pain (NRS 1-2/10). The neonate weighed 2072 g with an Apgar score of 10 at 1 and 5 minutes. Postpartum pain was managed with acetaminophen (2000 mg/day) and etodolac (40 mg/day).
On June 19, 2019, the patient reported recurrent pain in the right gluteal region (NRS 6-7/10). Following colostrum expression, the epidural catheter was removed, and oral oxycodone (20 mg/day) was initiated. Continuous epidural analgesia was administered for three consecutive days. During this period, no signs of infection, catheter displacement, or dysfunction were observed, and catheter replacement was not deemed necessary. By June 22, 2019, with the addition of 5 mg rescue doses of oxycodone (2-3 times daily), resting pain decreased to NRS 4-5/10, and the patient was discharged.
Subsequently, neoadjuvant chemotherapy was initiated in July, followed by surgical tumor resection in September, and postoperative chemotherapy in October, which remains ongoing. Written informed consent was obtained from the patient for the publication of this case.
Discussion
Managing cancer-related pain during pregnancy is particularly challenging, due to fetal safety concerns with systemic analgesics such as opioids and NSAIDs [1-4]. In this case, continuous lumbar epidural analgesia effectively controlled severe synovial sarcoma-associated pain, enabling the patient to assume an appropriate labor position and facilitate vaginal delivery without the use of systemic analgesics.
Synovial sarcoma is a rare soft tissue malignancy that accounts for 5-10% of all soft tissue sarcomas [5,6], with a peak incidence in individuals in their 20s and 30s [7]. Synovial sarcoma frequently arises in the lower extremities and is often associated with significant pain [7]. In our patient, worsening cancer-related pain during late pregnancy led to impaired ambulation and difficulty assuming a delivery position, potentially necessitating cesarean section.
Epidural analgesia provided targeted pain relief while minimizing fetal exposure to systemic drugs, avoiding potential cesarean delivery and possible need for general anesthesia. These interventions are associated with increased maternal morbidity and mortality, with cesarean section carrying a tenfold increase in maternal mortality compared to vaginal delivery [8], and general anesthesia carrying a 16.7-fold higher risk compared to regional anesthesia [9]. Although lidocaine with epinephrine is commonly used as a test dose, clinicians should be aware of the concerns regarding its reliability and safety in obstetric patients, as physiological changes during pregnancy may blunt the expected cardiovascular response, potentially masking intravascular injection [10-12]. Fentanyl-based test dosing has been proposed as a safer alternative in this population [13].
Previous reports have also demonstrated the utility of regional analgesia in similar clinical contexts. For instance, thoracic epidural analgesia has been used to manage thoracoabdominal sarcoma pain in pregnancy while avoiding systemic opioids and achieving favorable maternal and fetal outcomes [14]. Similarly, prolonged epidural catheterization provided effective pain control in a pregnant patient with cervical cancer [15].
Conclusions
This case demonstrates that epidural analgesia is a safe and effective strategy in selected patients for managing cancer-related pain in pregnancy when systemic analgesic use is limited. By providing adequate pain relief and facilitating appropriate labor positioning, epidural analgesia may help preserve the option of vaginal delivery in this patient population.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Management of nonobstetric pain during pregnancy and lactation Anesth Analg Rathmell JP Viscomi CM Ashburn MA 10741087851997935610310.1097/00000539-199711000-00021 · doi ↗ · pubmed ↗
- 2Opioid abuse and dependence during pregnancy: Temporal trends and obstetrical outcomes Anesthesiology Maeda A Bateman BT Clancy CR Creanga AA Leffert LR 1158116512120142540529310.1097/ALN.0000000000000472 · doi ↗ · pubmed ↗
- 3Opioid use in pregnancy Curr Psychiatry Rep Tobon AL Habecker E Forray A 1182120193173480810.1007/s 11920-019-1110-4PMC 10296780 · doi ↗ · pubmed ↗
- 4Nonsteroidal anti-inflammatory drugs during pregnancy and the initiation of lactation Anesth Analg Bloor M Paech M 1063107511620132355884510.1213/ANE.0b 013e 31828 a 4b 54 · doi ↗ · pubmed ↗
- 5A review of soft-tissue sarcomas: Translation of biological advances into treatment measures Cancer Manag Res Hoang NT Acevedo LA Mann MJ Tolani B 108911141020182978513810.2147/CMAR.S 159641 PMC 5955018 · doi ↗ · pubmed ↗
- 6Qualitative study to characterize patient experience and relevance of patient-reported outcome measures for patients with metastatic synovial sarcoma J Patient Rep Outcomes Eliason L Grant L Francis A 43620223550723110.1186/s 41687-022-00450-1PMC 9068846 · doi ↗ · pubmed ↗
- 7Biphasic synovial sarcoma in a 19-year-old pregnant woman: A case report Rom J Morphol Embryol Adameşteanu MO Scurtu R Lascăr I Vâlcu M PopescuŞA Sebe IT 289294562015 https://pubmed.ncbi.nlm.nih.gov/25826519/25826519 · pubmed ↗
- 8Maternal death in the 21st century: causes, prevention, and relationship to cesarean delivery Am J Obstet Gynecol Clark SL Belfort MA Dildy GA Herbst MA Meyers JA Hankins GD 3635199200810.1016/j.ajog.2008.03.00718455140 · doi ↗ · pubmed ↗