An Unusual Case of Chronic Delimited Rhinosinusal Mucormycosis With Secondary Cutaneous Involvement in a Patient With Ataxia-Telangiectasia Syndrome
Fadia Y Abdala Mendoza, Diego E Gómez López, Monica Ceballos-Pérez, Circe Ancona Castro, Jorge A García Campos, Rogelio de J. Treviño-Rangel, Hiram Villanueva-Lozano

TL;DR
A 15-year-old with ataxia-telangiectasia syndrome developed a rare chronic fungal infection affecting the sinuses and skin.
Contribution
This case report highlights an unusual presentation of mucormycosis in a patient with ataxia-telangiectasia syndrome.
Findings
The patient had a six-month history of recurrent sinusitis unresponsive to treatment.
Secondary cutaneous involvement was observed with ulcerated nodules and crusted plaques.
The case suggests a shift in the epidemiology of opportunistic infections towards new risk factors.
Abstract
Mucormycosis is an immunosuppression-related fungal infection. This pathogen usually manifests as an acute and rapidly progressive, deforming, and lethal disease, but chronic forms of zygomycosis occur rarely. Here we present a case of a 15-year-old female with ataxia-telangiectasia syndrome, reporting a six-month history of recurrent sinusitis and an atypical secondary skin infection characterized by ulcerated nodules and crusted plaques, unresponsive to multiple treatments. This case highlights the changing epidemiology of opportunistic infections, which were usually confined to specific immunosuppressive diseases but are recently presenting a shift towards their associated risk factors and comorbidities.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1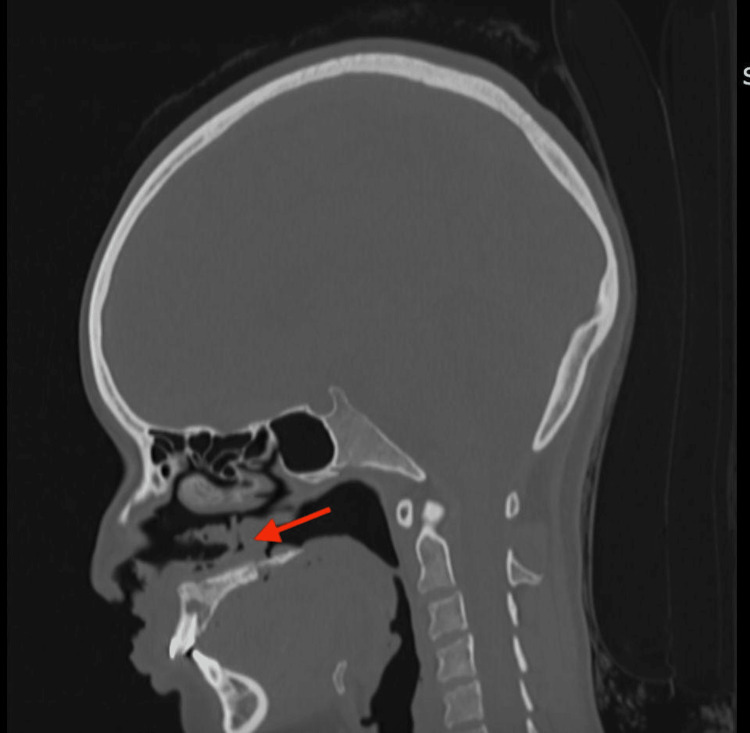 Figure 2
Figure 2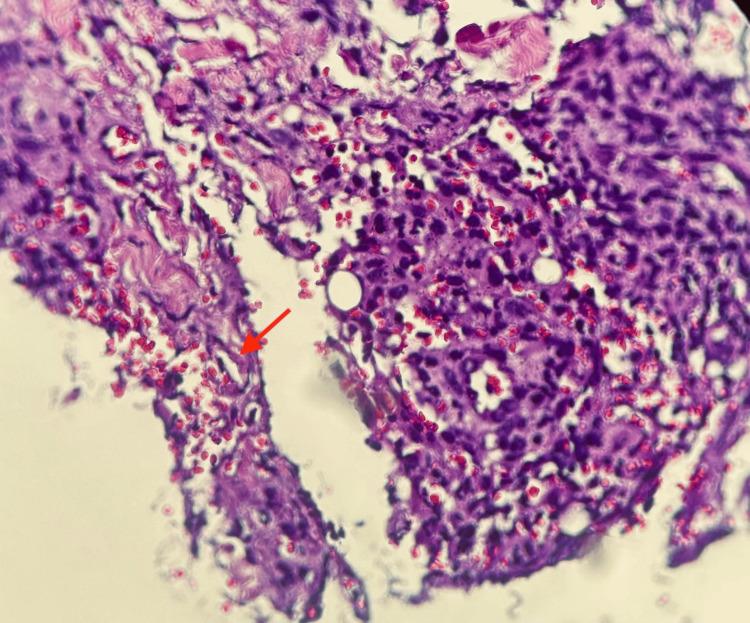 Figure 3
Figure 3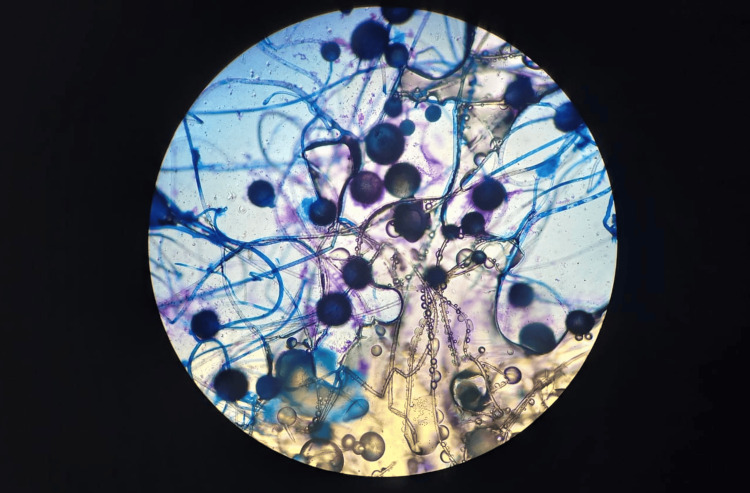 Figure 4
Figure 4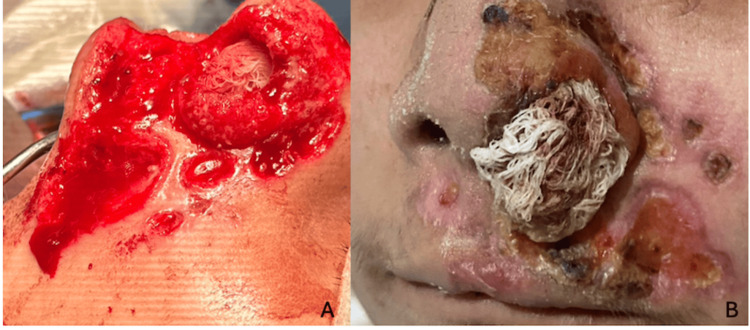 Figure 5
Figure 5| Antimicrobial treatment | Posology dosage | Interval and duration |
| Ceftriaxone | 50 mg/kg/day | IV every 12 hours for 4 days |
| Ceftazidime | 150 mg/kg/day | IV every 8 hours for 6 days |
| Amikacin | 15 mg/kg/day | IV every 12 hours for 7 days |
| Rifampicin | 20 mg/kg/day | IV every 8 hours for 7 days |
| Vancomycin | 43 mg/kg/day | IV every 8 hours for 7 days |
| Cefepime | 160 mg/kg/day | IV every 8 hours for 15 days |
| Meropenem | 75 mg/kg/day | IV every 8 hours for 8 days |
| Amikacin | 15 mg/kg/day | IV every 12 hours for 7 days |
| Antifungal treatment | Posology dosage | Interval and duration |
| Fluconazole | 5.5 mg/kg/day | IV every 24 hours for 7 days |
| Anmphotericin | 1 mg/m2/day | IV every 24 hours for 10 days |
| Fluconazole | 8 mg/kg/day | IV every 24 hours for 5 days |
| Fluconazole | 5 mg/kg/day | PO every 24 hours for 14 days |
| Opportunistic infections encountered with AT | Percentage |
| Otitis media | 46% |
| Sinusitis | 27% |
| Bronchitis | 19% |
| Neumonía | 15% |
| Sepsis | 5% |
| Herpes simple | 8% |
| Molluscum contagiosum | 5% |
| Candidal esophagitis | 3% |
| Herpes zoster | 2% |
| Uncomplicated varicella | 44% |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntifungal resistance and susceptibility · Fungal Infections and Studies · Ocular Infections and Treatments
Introduction
Mucormycosis is an opportunistic fungal infection characterized by a rapid, fulminant progression caused by fungi of the Mucorales group. Most frequently isolated genera are Rhizopus spp., Mucor spp., and Rhizomucor spp. [1]. Mucorales are mainly responsible for rhinocerebral or rhino-orbital infections, which occur after the inhalation of fungal spores, followed by pulmonary, gastrointestinal, cutaneous, and disseminated forms, predominantly in immunosuppressed patients (e.g., diabetes, renal failure, neutropenia, or the use of steroids) [1,2]. The acute form has been described as a clinical progression, and invasive infection typically occurs rapidly over days without appropriate treatment, although more protracted courses over weeks to months have been reported. The chronic presentations of rhinocerebral mucormycosis have been described [3]. In the chronic infection, the disease course is indolent and slowly progressive, often occurring over weeks to months. The infection can be acute or chronic, depending on the time of evolution, with the chronic form being rare (5.6% of rhinocerebral mucormycosis cases) [4].
Ataxia-telangiectasia (Louis-Bar syndrome) is a rare condition that clinically presents with progressive cerebellar ataxia, dystonia, oculocutaneous telangiectasias, growth retardation, premature aging, recurrent sinopulmonary infections, an increased risk of cancer (particularly of the lymphoid lineage), and hypersensitivity to ionizing radiation. Other clinical manifestations may include hypogonadism and delayed puberty, and nonketotic and insulin-resistant diabetes mellitus. Cellular and humoral immunodeficiency is responsible for the recurrence of upper and lower respiratory tract infections, the latter of which leads to chronic lung disease. Infectious pneumonia (viral or bacterial) or aspiration pneumonia is the leading cause of death in these patients. Cellular and humoral immunodeficiency is a hallmark of this disease, leading to a higher incidence of upper and lower respiratory tract infections [5,6]. However, classic opportunistic infections associated with cellular deficiencies, such as Pneumocystis jirovecii pneumonia or Cryptococcus spp. meningitis is rarely reported in these patients [7].
We present an unusual case of a patient with ataxia-telangiectasia who developed a chronic rhinosinusoidal lesion with deep and cutaneous involvement caused by Rhizopus arrhizus.
Case presentation
A 15-year-old female with a history of ataxia-telangiectasia syndrome, diagnosed at four years of age, was found to have a confirmed ATM gene mutation with two pathogenic variants (c.2839-3_2839delinsGATACTA (splice acceptor) and c.8977C>T (p.Arg2993)), both in heterozygosis. She also had severe immunodeficiency with IgA and IgE deficiency and severe grade III malnutrition according to WHO criteria.
Six months prior to her current diagnosis, she experienced multiple recurrent episodes of sinusitis, predominantly affecting the left maxillary sinus as confirmed by computed tomography and direct visualization as evaluated by an otorhinolaryngologist. Rhinoscopy revealed a rapidly evolving septal perforation, accompanied by febrile peaks of up to 38°C. Despite the initiation of antimicrobial agents (Table 1) and antifungal regimens (Table 2), no significant clinical response was observed.
Four months later, she developed localized dermatosis on the face, particularly in the nasal region, characterized by nodules that ulcerated within two weeks (Figure 1).
Skin lesionsDermatosis located on the head, affecting the face in the region of the nose, on the left nasal dorsum, extending to the midline, lateral wall, and left nostril orifice, as well as the bilateral alar rim, nasolabial fold, cheek, and medial upper lip. It consists of five ulcerated, necrotic nodules of variable size, ranging from 0.5 to 5 cm in diameter, with well-defined, irregular borders, all settled on an erythematous background. The increased erythema in the background is possibly due to ataxia-telangiectasia. At the periphery of all ulcers, there is granulation tissue; in the background of some ulcers, the presence of fibrin is especially noteworthy at the alar border and nasolabial fold, with a loss of anatomy of the left nasal ala.
She also exhibited soft palate perforation. Through biopsy with special stains, acid-fast bacilli infections were ruled out. Computed tomography findings included disruption of soft tissues at the left upper labial region, nasolabial fold, and nasal ala, predominantly on the left side, with perforation of the cartilaginous portion of the nasal septum. There was also the presence of material with soft tissue density and a gaseous appearance in the nasal and oral vestibule, secondary to perforation of the soft palate. Bone tissue showed areas of sclerosis and lytic lesions in the alveolar and palatine processes of the maxillary bone, affecting the posterior surface of the upper incisors, the anterior surface of the bilateral maxillary bone, and the horizontal lamina of the palatine bone (Figure 2).
CT scanSagittal computed tomography: Disruption of soft tissues in the left upper labial region, nasolabial fold, and nasal ala, predominantly on the left side, with perforation of the cartilaginous portion of the nasal septum. There was also the presence of material with soft-tissue density and a gaseous appearance in the nasal and oral vestibule, secondary to perforation of the soft palate (red arrow). Bone tissue shows areas of sclerosis and lytic lesions in the alveolar and palatine processes of the maxillary bone, affecting the posterior surface of the upper incisors, the anterior surface of both maxillary bones, and the horizontal plate of the palatine bone.
Serum protein electrophoresis was performed as part of the diagnostic evaluation to rule out acute or chronic inflammatory conditions, hepatic dysfunction, and paraneoplastic syndromes. Serum protein electrophoresis revealed an alpha-2 fraction of 14.4% (reference range: 7.5-12.6%) and a gamma fraction of 29.2% (reference range: 8.0-15.8%), both of which were positive.
Due to its chronic, persistent progression, a new biopsy of the lesion was performed and sent for culture and periodic acid-Schiff (PAS) staining. In culture, a rapidly growing filamentous fungus in Sabouraud-Dextrose and Papa Dextrose agar was visualized, and the presence of broad, irregularly branched, and poorly septate hyphae was reported in histopathology (Figure 3).
Skin biopsyGross description: Spindle-shaped skin biopsy measuring 0.7 × 0.4 cm, processed and stained with hematoxylin and eosin. Microscopic description: At the subcutaneous level, there is a mixed inflammatory infiltrate with areas of necrosis, accompanied by numerous macrophages and extravasated erythrocytes. Broad, non-septate hyphae (red arrow) with right-angled (90º) branching are also observed.
The fungus was morphologically identified as Rhizopus spp. Subsequent sequencing of the internal transcribed spacer (ITS) non-coding region confirmed it as Rhizopus arrhizus (Genbank accession number PV558343) (Figure 4).
Direct examinationDirect examination with lactophenol cotton blue stain revealed numerous fungal structures, with the presence of broad, poorly septate, and branched hyphae, compatible with Rhizopus spp.
Antifungal susceptibility testing using the broth microdilution method (Clinical and Laboratory Standards Institute M38-Ed3) [8] was performed, and the following results were presented: itraconazole 8.0 mcg/mL, posaconazole 0.25 mcg/mL, isavuconazole 2.0 mcg/mL, and amphotericin B 0.25 mcg/mL.
Due to the limitations in Mexican public hospitals, treatment with amphotericin B deoxycholate (1 mg/kg/day) for 14 days was initiated, and 15 days after the initial dose of amphotericin B, itraconazole oral treatment was started and continued, along with broad-spectrum antibiotics to mitigate the risk of bacterial superinfection. Surgical debridement of necrotic tissue was also performed as a partial debridement (Figure 5A). This was delayed because of the difficulty in obtaining a positive culture/biopsy, as well as diagnostic uncertainty associated with the low reported incidence of this type of localized chronic presentation in this group of patients. The treatment was followed by wound healing with Triticum vulgare and pirfenidone (Figure 5B). The infection was contained, with no systemic involvement confirmed by multiple negative control cultures and bronchoalveolar lavage tests.
TreatmentA: debridement after surgery of the necrotic ulcers; B: evolution one month after debridement, topical treatment with Triticum vulgare and pirfenidone, led to an improvement of the dermatosis, with involution and decrease in the diameter of some of the ulcers.
Unfortunately, the patient eventually succumbed to complications of her underlying disease.
Discussion
Acute rhinomucormycosis typically presents as an erythematous and edematous plaque with central ulceration, progressing rapidly to involve subcutaneous tissue, muscle, and bone [1]. However, atypical and chronic forms can also occur, as seen in this patient, who developed rhinosinusal lesions followed by cutaneous nodules that ulcerated [4,6].
In this case, the initial site of infection was the nasal septum, leading to perforation, cutaneous extension, and eventual perforation of the soft palate, creating a communication between the nasal and oral cavities. No systemic, orbital, cerebellar, or other organ involvement was observed.
Severe IgA deficiency likely contributed to the patient’s slow response to treatment, as IgA plays a crucial role in mucosal immunity, preventing pathogen adherence and penetration [9]. The presence of midfacial nodules initially raised suspicion for natural killer (NK) lymphoma due to the rapid clinical progression, which, alongside acute mucormycosis, was considered in the differential diagnosis. However, the slower evolution and chronic nature of the patient’s condition ruled out these acute pathologies.
Considering the markedly chronic progression of the disease, along with the absence of documented cases of mucormycosis associated with ataxia‑telangiectasia syndrome and the exceptional rarity of chronic mucormycosis in pediatric patients, alternative infectious etiologies were contemplated as contributors to the severity of the clinical presentation (Table 3).
Differential diagnoses included actinomycosis, as well as infections caused by typical and atypical mycobacteria. Despite multiple histopathological and microbiological evaluations, including biopsies obtained from sites such as septal perforations and cutaneous lesions, all specimens were negative for infectious agents at the time of analysis.
Mucormycosis should be included in the differential diagnosis for patients of this profile, particularly underscoring the need for heightened clinical suspicion in cases where the primary disease process has precipitated significant malnutrition and subsequent immunosuppression. This case stands out as a rarely documented chronic mucormycosis in ataxia-telangiectasia syndrome, with unusual skin involvement. Chronic mucormycosis is possible in immunodeficient states. Skin signs can be sentinel clues. High suspicion is crucial despite slow progression.
Infections in immunocompromised patients often present atypically, potentially delaying diagnosis without a high index of suspicion. Early diagnostic methods, such as potassium hydroxide (KOH) or calcofluor staining, are essential for the timely initiation of treatment, which should include surgical debridement and first‑line antifungals like liposomal amphotericin B [1,11,12].
Unfortunately, our patient experienced additional complications, including nosocomial pneumonia and multiorgan failure, leading to hepatic and renal involvement and eventual fatality.
Conclusions
This case highlights the diagnostic and therapeutic challenges posed by chronic rhinomucormycosis in immunocompromised pediatric patients, particularly in the context of an underlying primary immunodeficiency. The unusual chronic evolution, absence of systemic dissemination, and progressive local tissue destruction underscore the importance of maintaining a high index of suspicion for mucormycosis, even in atypical clinical scenarios. Despite extensive microbiological and histopathological investigations, diagnostic confirmation may remain elusive, reinforcing the need for early empirical antifungal therapy in suspected cases. In patients with severe immunodeficiencies such as IgA deficiency and complex syndromic backgrounds like ataxia-telangiectasia, infections may present insidiously and progress despite standard interventions. Prompt initiation of both surgical and medical treatment remains critical; however, this case tragically demonstrates that advanced disease and comorbidities, such as nosocomial infections and multiorgan failure, can significantly compromise prognosis. Ultimately, early recognition and multidisciplinary management by the ENT surgeons, infectious disease specialists, pathologists, and pediatric or immunology teams are key aspects of complex case care. It's essential to improving outcomes in similarly complex clinical presentations.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mucormycosis: current and future management perspective (Article in Spanish)Rev Iberoam Micol Martín Gómez MT Salavert LletíM 911003820213414483510.1016/j.riam.2021.04.003 · doi ↗ · pubmed ↗
- 2Rare presentation of nasal mucormycosis Indian J Otolaryngol Head Neck Surg Wadhera R Vashist A 336733697420223645283310.1007/s 12070-020-02001-w PMC 9701954 · doi ↗ · pubmed ↗
- 3Chronic rhinocerebral mucormycosis Laryngoscope Harrill WC Stewart MG Lee AG Cernoch P 129212971061996884980410.1097/00005537-199610000-00024 · doi ↗ · pubmed ↗
- 4Chronic rhino-orbito-cerebral mucormycosis: a case report and review of the literature Ann Med Surg (Lond) Gutiérrez-Delgado EM Treviño-González JL Montemayor-Alatorre A 8791620162698123710.1016/j.amsu.2016.02.003PMC 4776268 · doi ↗ · pubmed ↗
- 5Ataxia-telangiectasia (Louis-Bar syndrome) (Article in Spanish)Arch Pediatr Urug Delfino M Bruzzone R Rey A Delfino A Pírez MC 154158772006 http://www.scielo.edu.uy/pdf/adp/v 77n 2/v 77n 2a 12.pdf
- 6Chronic rhinocerebral mucormycosis: a rare case report and review of the literature Mycoses Dimaka K Mallis A Naxakis SS Marangos M Papadas TA Stathas T Mastronikolis NS 6997025720142503992510.1111/myc.12219 · doi ↗ · pubmed ↗
- 7Acquired Glanzmann's thrombasthenia as part of multiple-autoantibody syndrome in a pediatric heart transplant patient J Pediatr Rawal A Sarode R Curtis BR Karandikar NJ Friedman K Rogers ZR 6726741442004 https://doi.org/10.1016/j.jpeds.2003.12.0401512701210.1016/j.jpeds.2003.12.040 · doi ↗ · pubmed ↗
- 8M 38 Reference Method for Broth Dilution Antifungal Susceptibility Testing of Filamentous Fungi Clinical and Laboratory Standards Institute Wayne, PACLSI 2017 https://webstore.ansi.org/preview-pages/CLSI/preview_CLSI%2BM 38-Ed 3.pdf