Morphological analysis of peritoneal fluid in fumarate hydratase deficiency-associated renal cell carcinoma: a case report
Yingying Du, Yu Shang, Chang Shi

TL;DR
This case report examines peritoneal fluid from a rare kidney cancer patient to improve diagnosis and understanding of FH-RCC.
Contribution
The study presents unique cytological features of peritoneal fluid in FH-RCC, aiding in its differential diagnosis.
Findings
Distinct cellular features were identified in the peritoneal fluid of an FH-RCC patient.
The findings may enhance the recognition and management of FH-RCC through improved differential diagnosis.
Abstract
Fumarate hydratase deficiency-associated renal cell carcinoma (FH-RCC) is a rare, aggressive subtype of renal cell carcinoma (RCC) driven by FH gene mutations. Its non-specific imaging features and heterogeneous pathological morphology complicate early diagnosis. This case report describes the cytological evaluation of peritoneal fluid from a 35-year-old male with FH-RCC, highlighting distinct cellular features within the effusion. These findings provide insights into the clinicopathological differential diagnosis of serous cavity effusions, potentially enhancing the recognition and management of this uncommon malignancy.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
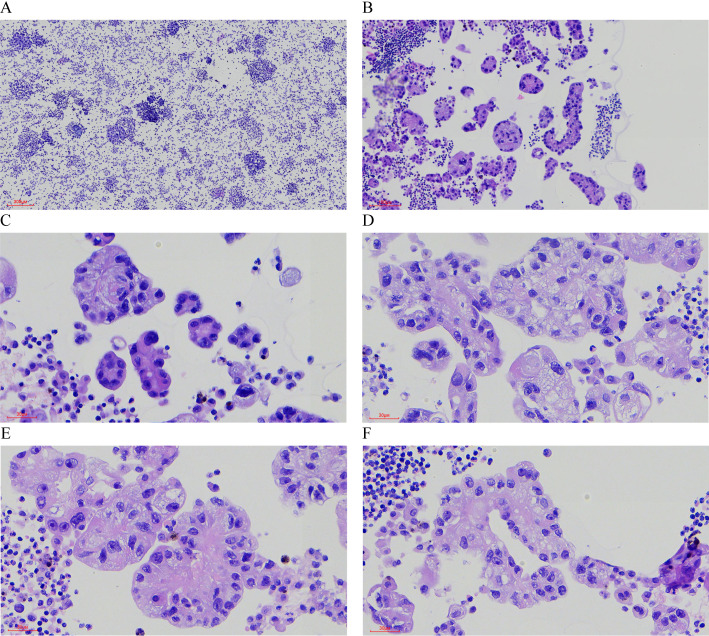 Figure 1
Figure 1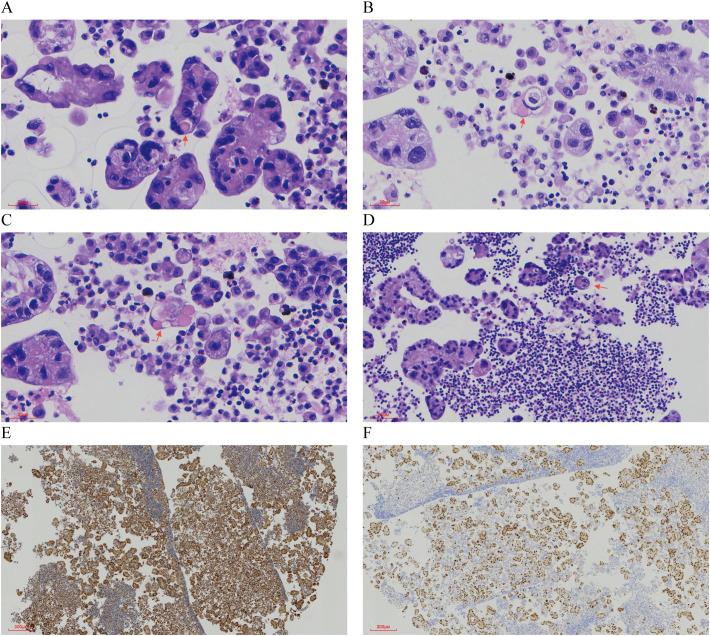 Figure 2
Figure 2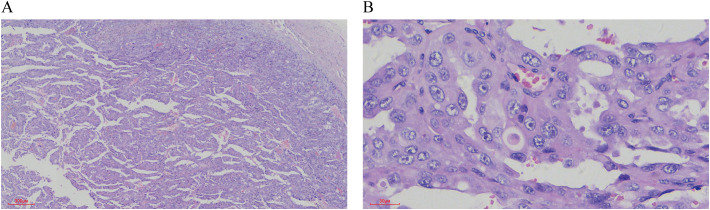 Figure 3
Figure 3| No. | Publication Date/Author | Gender/Age | HLRCC evidence and family history | Surgical approach | Tumor size(cm) | Pathological morphological features | Immunohistochemistry | Other findings | Follow-up | |
|---|---|---|---|---|---|---|---|---|---|---|
| FH | 2SC | |||||||||
| 1 | 2017/Steven C Smith | Male/11 | Germline G354R FH mutation | Radical nephrectomy | 8.5 | Solid, tubular, and cystic; Eosinophilic cytoplasm; Eosinophilic cytoplasmic inclusions | – | + | / | NED, >84 months |
| 2 | Male/40 | Homozygous p.K80 fs FH mutation in separate tumours | Radical nephrectomy | 0.2 and 0.4 | Solid, nodular; Eosinophilic cytoplasm; Eosinophilic cytoplasmic inclusions | – | + | / | Liver metastasis, of high grade, at presentation | |
| 3 | Male/41 | / | Partial nephrectomy | 5 | Solid; Eosinophilic cytoplasm; Eosinophilic cytoplasmic inclusions | – | + | Renal: Multilocular cystic change | NED, 48 months (oncocytic RCC); metastasis at 3 months after high-grade FHRCC nephrectomy | |
| 4 | 2020/Nicolas Wyvekens | Female/50 | Cutaneous leiomyomata; Uterine leiomyoma | Nephrectomy with lymphadenectomy | FHRCC:11 Uterine leiomyoma: none | FHRCC: Tubulocystic and papillary growth pattern, prominent nucleoli, perinucleolar halos; | FHRCC: -; Uterine leiomyoma: - | / | / | Local recurrence and subsequent treatment one year later; NED, 14 months |
| 5 | Female/46 | Cutaneous leiomyomata; Uterine leiomyoma | Partial nephrectomy | First recurrent tumor nodule:1.2 | FHRCC recurrence and metastasis: Papillary growth pattern, large tumor cells, prominent nucleoli with perinuclear halos, abundant cytoplasmic “colloid-like” inclusions; | FHRCC recurrence: -; | / | / | Local recurrence | |
| 6 | 2022/Athanase Billis | Female/45 | Uterine leiomyoma | / | 7.5 | Papillary arrangement, solid arrangement, tubulocystic arrangement, eosinophilic cytoplasm, large nucleoli surrounded by a clear halo, eosinophilic inclusions (round and oval) | – | + | / | NED, 15 months |
| 7 | Female/35 | Uterine leiomyoma | / | 21 | Papillary arrangement, solid arrangement, eosinophilic cytoplasm, large nucleoli surrounded by a clear halo, eosinophilic inclusions (round and oval) | – | + | / | NED, 32 months | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRenal cell carcinoma treatment · Renal and related cancers · Pancreatic and Hepatic Oncology Research
Introduction
1
Fumarate hydratase deficiency-associated renal cell carcinoma (FH-RCC) is an infrequent subtype of renal cell carcinoma (RCC) resulting from germline or somatic mutations in the FH gene (1). Germline mutations are linked to hereditary leiomyomatosis and renal cell carcinoma syndrome (HLRCC), an autosomal dominant condition characterized by renal malignancies, uterine leiomyomas, and cutaneous leiomyomas (2). Compared to common RCC subtypes, such as clear cell RCC (ccRCC), FH-RCC exhibits earlier onset, aggressive behavior, and a propensity for early metastasis (1). However, its rarity limits comprehensive understanding of its multi-omics profile (3), including genomics, epigenomics, and immune microenvironment in metastatic settings. Non-specific imaging and clinical presentations further challenge timely diagnosis. This report presents a cytological analysis of peritoneal fluid in a patient with FH-RCC, aiming to delineate characteristic morphological features that may facilitate early detection and inform clinical management.
Case presentation
2
A 35-year-old male presented with significant peritoneal effusion, thoracolumbar vertebral destruction, and hypodense liver lesions on imaging. Twenty-two months prior, he underwent radical nephrectomy for a renal tumor, with postoperative pathology confirming HLRCC-associated FH-RCC. Post-surgery, he received tiragolumab and cabozantinib combination therapy. Subsequent bone and lung metastases prompted treatment with bevacizumab, lenvatinib, and toripalimab. Six months later, massive peritoneal effusion developed, necessitating aspiration. Liquid-based cytology and cell block sections were analyzed. This study was approved by the Ethics Committee of the First Affiliated Hospital of Dalian Medical University.
Pathological Findings: Liquid-based cytology revealed abundant tumor cells arranged in papillary formations, with areas of solid, nested, or dispersed single cells (Figures 1A, B). Tumor cells were large, with indistinct borders, eosinophilic or clear cytoplasm, and occasional biphasic staining. Cytoplasmic vacuoles were observed in some cells (Figures 1C–F). Nuclei displayed variable size and shape, irregular contours, prominent eosinophilic nucleoli, and occasional perinucleolar halos (Figures 1E, F). Phagocytosis of similar cells and eosinophilic globular material was noted in some tumor cells (Figures 2A–D). Immunophenotype (Peritoneal Fluid): 2SC (+), Ber-EP4 (+), FH (+), CK (+), Ki-67 (30% in hotspots), MOC-31 (+), Pax-8 (+), P53 (wild-type), CAIX (+), CR (-), Desmin (-), WT-1 (-), CK20 (-), CK7 (-), P40 (-) (Figures 2E, F). Post-Nephrectomy Pathology: The primary tumor exhibited papillary, nested, and solid architecture with prominent nucleoli (Figures 3A, B). Tumor emboli were identified in blood vessels and the renal vein. Immunophenotype (Primary Tumor): 2SC (+), CAIX (+), CD10 (-), CK (+), EMA (+), FH (+), Ki-67 (30% in hotspots), TFE3 (-), CK20 (-). Diagnosis: Fumarate hydratase-deficient renal cell carcinoma (FH-RCC).
Hematoxylin-Eosin (HE) Staining of Tumor Cells in Ascitic Fluid. (A) Tumor cells are numerous and densely packed in the ascitic fluid. (×40) (B) The tumor cells exhibit a variety of growth patterns, including papillary, solid, and nested structures. (×100) (C-F) The cytoplasm is abundant, eosinophilic or transparent, with some cells showing amphophilic staining or cytoplasmic vacuoles. (×400) (E, F) Prominent eosinophilic nucleoli are visible, some surrounded by a distinct halo (×400).
Characteristic Morphology and Immunohistochemical Features in Ascitic Fluid. (A-C) Eosinophilic spherules are observed. (×400) (D) Tumor cells exhibit phagocytosis. (×200) (E) Immunohistochemical staining for FH is positive. (×40) (F) Immunohistochemical staining for PAX8 is positive (×40).
HE staining of Postoperative Renal Tumor Features. (A) The tumor tissue displays a mixture of papillary, nested, and solid growth patterns. (×40) (B) The tumor cells are large, with either eosinophilic or vacuolated cytoplasm. The nuclei vary in size, and prominent eosinophilic nucleoli are evident (×400).
Treatment Course: Three months post-nephrectomy, the patient began tiragolumab and cabozantinib. One year later, bone and lung metastases emerged, leading to a regimen of bevacizumab, lenvatinib, and toripalimab. Six months into this treatment, significant peritoneal effusion developed.
Discussion
3
Fumarate hydratase-deficient renal cell carcinoma (FH-RCC), first described by Launonen et al. in 2001, arises from FH gene mutations or inactivation on chromosome 1q42.3-43 (2, 4). This leads to fumarate accumulation, stabilizing hypoxia-inducible factor 1-alpha (HIF1α) and driving metabolic dysregulation and tumorigenesis. Classified under HLRCC in the 2016 WHO renal tumor classification (4th edition), FH-RCC was redefined in the 2022 WHO update to encompass all RCCs with FH alterations (5, 6). According to the 5th edition of the WHO classification, the required diagnostic criteria for fumarate hydratase-deficient renal cell carcinoma (FH-RCC) include immunohistochemical evidence of FH germline or somatic mutation, or FH deficiency, defined by loss of FH protein expression and/or positive 2SC staining. The supportive diagnostic features include the presence of multiple, admixed architectural patterns with at least focal macronucleoli, and a personal or family history of cutaneous and uterine leiomyomas, which may indicate an association with hereditary leiomyomatosis and renal cell carcinoma (HLRCC) syndrome (7).
FH-RCC typically affects younger patients and presents as a solitary renal mass with non-specific symptoms (8). Its aggressive nature predisposes to early metastasis, commonly to lymph nodes, bones, liver, and lungs (9). In this case, a 35-year-old male developed bone and lung metastases 15 months post-nephrectomy, followed by peritoneal effusion and liver metastasis at 22 months.
Cytologically, FH-RCC is characterized by prominent eosinophilic nucleoli with perinucleolar halos (8). In this patient’ s peritoneal effusion, eosinophilic globular material was also observed, potentially reflecting fibrin or peroxisomal complexes linked to autophagic defects, as suggested by prior studies (10). Similar globules have been reported in papillary and clear cell RCC subtypes, distinguishable by their distinct cytoplasmic boundaries (11, 12).
A review of FH-RCC cases with eosinophilic globules (Table 1) revealed: (1) no gender predilection (female: male= 4:3); (2) mean onset age of 38 years (range: 11–50); (3) frequent FH mutations (e.g., G354R, p.K80fs); (4) association with HLRCC features in some cases; (5) variable tumor sizes (0.2–21 cm) and growth patterns (solid, tubular, cystic); (6) consistent FH negativity and 2SC positivity; and (7) variable outcomes, with some patients disease-free post-surgery and others experiencing recurrence or metastasis.
Differential diagnosis of peritoneal effusion includes: (1) Ovarian Cancer: Features irregular clusters or glandular structures, often with calcified psammoma bodies in serous carcinoma, contrasting with FH-RCC’s eosinophilic nucleoli and “owl-eye” appearance (13–15). (2) Gastrointestinal Adenocarcinoma: Exhibits glandular or signet-ring morphology with PAS-positive vacuoles, distinguishable by negative CDX-2 and villin in FH-RCC. (3) Mesothelioma: Shows scattered or clustered cells with basophilic cytoplasm and BAP1 loss in ~60% of cases, unlike FH-RCC’s eosinophilic features (16).
The presence of eosinophilic globules in this case, alongside characteristic nucleoli and immunoprofile (FH loss, 2SC positivity), strongly supports FH-RCC diagnosis. Absent FH IHC staining in tumor cells is highly specific for FH-RCC, but its sensitivity is limited. In contrast, diffuse expression of 2-succinocysteine (2SC), resulting from aberrant cysteine modification due to fumarate accumulation, is highly sensitive but lacks specificity. Additionally, a recently described pattern of heterogeneous FH expression—characterized by patchy positive staining—has been associated with FHRCC. This phenomenon is thought to result from certain missense mutations that impair FH enzymatic activity while allowing for variable protein expression (17–21). In this case, immunohistochemical staining showed diffuse and strong positivity for 2SC, whereas FH demonstrated a patchy immunoreactivity pattern.
Therapeutically, FH-RCC lacks standardized guidelines. Bevacizumab with erlotinib has shown partial efficacy in HLRCC-associated RCC, while immune checkpoint inhibitors (ICIs) with anti-angiogenic agents yield objective response rates (ORR) of 27–44% in retrospective studies (22–24). In this patient, despite sequential therapies (tiragolumab/cabozantinib, then bevacizumab/lenvatinib/toripalimab), disease progression persisted, highlighting therapeutic challenges in advanced FH-RCC.
Conclusion
4
This report presents the first cytological description of FH-RCC in peritoneal effusion, emphasizing distinctive features—eosinophilic nucleoli, perinucleolar halos, and globular material—that aid differential diagnosis. Despite multimodal therapy, disease progression underscores the aggressive nature and poor prognosis of some FH-RCC cases, necessitating further research into effective treatments.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Rare Kidney Cancer Collaborative Group Genitourinary Cancer Committee China Anti-Cancer Association . Consensus on clinical diagnosis and treatment of fumarate hydratase-deficient renal cell carcinoma. Zhonghua Wai Ke Za Zhi. (2022) 60:961–8. doi: 10.3760/cma.j.cn 112139-20220729-00328 36323576 · doi ↗ · pubmed ↗
- 2Patel VM Handler MZ Schwartz RA Lambert WC . Hereditary leiomyomatosis and renal cell cancer syndrome: an update and review. J Am Acad Dermatol. (2017) 77:149–58. doi: 10.1016/j.jaad.2017.01.023 28314682 · doi ↗ · pubmed ↗
- 3Board PDQCGE . Hereditary leiomyomatosis and renal cell cancer (Pdq®): health professional version. In: Pdq Cancer Information Summaries. National Cancer Institute (US, Bethesda (MD (2002).33724749 · pubmed ↗
- 4Launonen V Vierimaa O Kiuru M Isola J Roth S Pukkala E . Inherited susceptibility to uterine leiomyomas and renal cell cancer. Proc Natl Acad Sci U.S.A. (2001) 98:3387–92. doi: 10.1073/pnas.051633798 PMC 3066311248088 · doi ↗ · pubmed ↗
- 5Inamura K . Renal cell tumors: understanding their molecular pathological epidemiology and the 2016 who classification. Int J Mol Sci. (2017) 18(10):2195. doi: 10.3390/ijms 18102195 29053609 PMC 5666876 · doi ↗ · pubmed ↗
- 6Goswami PR Singh G Patel T Dave R . The who 2022 classification of renal neoplasms (5th edition): salient updates. Cureus. (2024) 16:e 58470. doi: 10.7759/cureus.58470 38765391 PMC 11100973 · doi ↗ · pubmed ↗
- 7Hes O Gill AJ Gupta S Jimenez RE Smith SC Trpkov K . Fumarate hydratase-deficient renal cell carcinoma. In: WHO Classification of Tumours: Urinary and Male Genital Tumours. 5th ed. Lyon, France: International Agency for Research on Cancer (IARC) (2022). pp. 78–79.
- 8Kuroda N Tsutsui M Iguchi M Nobuoka E Uehara T Sonobe Y . Fumarate hydratase-deficient renal cell carcinoma: A clinicopathological study of seven cases including hereditary and sporadic forms. Ann Diagn Pathol. (2020) 49:151599. doi: 10.1016/j.anndiagpath.2020.151599 32977234 · doi ↗ · pubmed ↗