In Vivo Assessment of Ankle Stability During Dynamic Exercises: Scoping Review
Sandra Sanchez-Morilla, Pablo Cervera-Garvi, Laura Ramirez-Perez, Irene Garcia-Paya, Salvador Diaz-Miguel, Ana Belen Ortega-Avila

TL;DR
This scoping review explores in vivo methods for assessing ankle stability during dynamic exercises, identifying commonly used tools and techniques.
Contribution
The study systematically categorizes in vivo methodologies for dynamic ankle stability assessment, highlighting optimal tool combinations.
Findings
3D motion capture and force platforms were most frequently used for functional tasks and walking.
Multisegmented foot models combined with these tools appear optimal for assessing ankle stability.
Six categories of dynamic exercises were identified, including balance, stair climbing, and running.
Abstract
Background: The ankle joint plays a key role in stabilizing the lower limb during interaction with ground reaction forces. Instability can result in pain, weakness, and impaired movement. Although assessing ankle stability is important, few studies examine existing in vivo methodologies for dynamic load assessment, limiting effective injury management. Objective: To identify in vivo techniques using objective measurement tools for assessing ankle stability during dynamic exercise. Methods: A scoping review was performed based on PRISMA-ScR criteria. Five databases—PubMed, PEDro, Embase, SPORTDiscus, and CDSR—were searched from inception to September 2024. Results: Out of 1678 records, 32 studies met the inclusion criteria. A total of 1142 subjects were included: 293 females (25.6%), 819 males (71.7%), and 30 unspecified (2.62%). Six categories of dynamic exercise were identified:…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
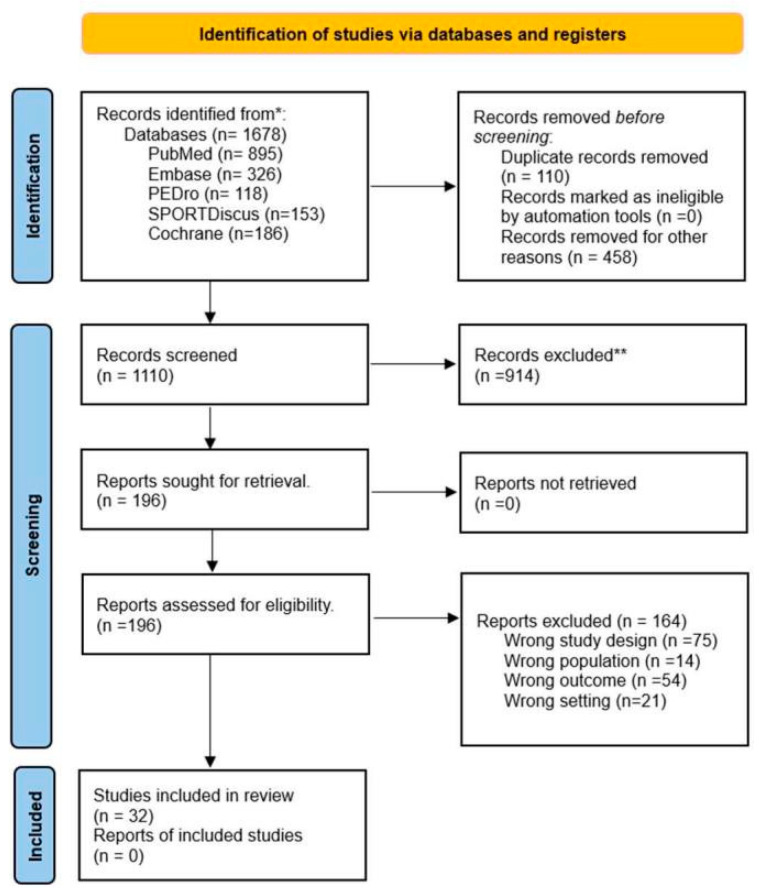 Figure 1
Figure 1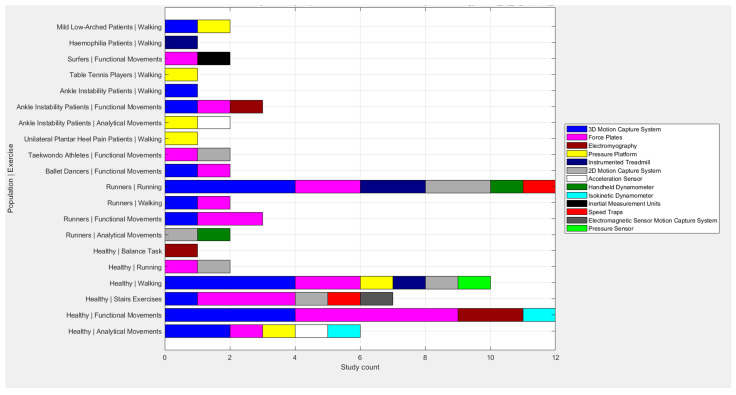 Figure 2
Figure 2- —University Teacher Training Programme (FPU) of the Ministry of Science, Innovation, and Universities of Spain
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFoot and Ankle Surgery · Lower Extremity Biomechanics and Pathologies · Sports injuries and prevention
1. Introduction
The ankle joint, due to its anatomical configuration, acts as a complex element of congruence within the lower limb [1]. From a functional perspective, it plays a crucial role as a stabilizer, regulating the interactions of the lower limb with ground reaction forces [2]. Since stability is the main characteristic of the ankle, any deficit in this regard may manifest through symptoms such as pain, weakness, and swelling, compromising its ability to maintain the control and balance required for movement [3]. Acute lateral ankle sprain (LAS) is a relatively common condition of the lower limb, primarily affecting the lateral ligaments of this anatomical complex [4]. Its most frequent mechanism of occurrence happens during dynamic activity, where the loads and stresses that this joint must bear increase, compromising its biomechanics [5].
A failure in the rehabilitation of the acute phase of the sprain often leads, in most cases, to the recurrence of the injury and, subsequently, to its chronicity in the patient [6]. Chronic ankle instability (CAI) is characterized by a dysfunction in both mechanical and functional stability, linked to residual symptoms from the acute lateral sprain [7]. Functional instability is associated with deficits in postural control, proprioception, and joint weakness [8]. On the other hand, mechanical instability is mainly characterized by the presence of ligamentous laxity [9]. Many patients describe it as a sensation of “giving way”, where the ankle suddenly weakens, causing a loss of control or balance [10]. The problems associated with this pathology are numerous and affect various aspects of the individual’s mobility and well-being [11]. The impairment in ankle functionality can compromise the ability to perform essential movements, leading to difficulties in carrying out everyday activities, such as walking, jumping, working, or practicing sports [12]. These impediments not only generate physical limitations but can also negatively influence the subject’s quality of life, both in their work performance and their emotional well-being, as reduced mobility impacts their autonomy and participation in recreational or social activities [13]. Furthermore, patients with chronic ankle instability present greater impairments in terms of kinesthesia and joint position sense in the affected limb compared with their healthy limb [14]; this pathology could affect not only the injured side but also the healthy limb due to the alteration of the sensorimotor system, leading to postural control issues during single-stance tasks [15], thus confirming again the influence on a patient’s daily life activities.
Considering the prevalence and impact of this pathological mechanism, its diagnosis and assessment become fundamental for appropriate therapeutic management [16]. Identifying tools for assessing ankle stability can provide categorical information to interpret the presence or absence of injury or symptoms [17]. The information in this regard is scattered in clinical practice. Typically, the primary diagnostic focus is on the patient’s medical history, physical examination, symptom identification, and the exclusion of potential fractures. In this sense, diagnostic imaging, clinical tests, and self-administered patient questionnaires have played a fundamental role [18]. However, since the ankle is characterized by complex biomechanics [19], analyzing how variables such as force or deformation influence the structures, particularly ligamentous ones, of this joint is necessary for an adequate evaluation. Although there are in vitro studies [20,21] that assess the anatomical complex of the ankle considering these aspects, there is no clear research supporting the in vivo evaluation, particularly during dynamic exercise, of ankle stability.
The objective of this study, formulated according to the PICO structure, was to identify which in vivo techniques using objective measurement instruments have been applied to evaluate ankle stability during dynamic exercise in individuals assessed for ankle instability.
2. Materials and Methods
2.1. Protocol and Registration
A scoping review was conducted following the criteria of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA), specifically the extension for scoping reviews (PRISMA-ScR guidelines) [22]. The protocol was not registered as PROSPERO does not allow the registration of scoping reviews.
2.2. Eligibility Criteria
2.2.1. Inclusion Criteria
In vivo observational studies were selected according to the following criteria: studies including men or women over 18 years of age, who were defined as physically active according to the WHO [23], to whom a measurement with in vivo objective techniques was applied to determine ankle instability during dynamic exercises involving ankle movement under functional conditions.
2.2.2. Exclusion Criteria
Among the studies that met the inclusion criteria, the following studies were excluded: studies that assessed surgical techniques, studies that only applied an external element (plantar orthoses, footwear) in the assessment of dynamic exercise, and studies that exclusively included clinical tests, questionnaires, or imaging tests for the assessment of ankle instability.
2.3. Information Sources and Search
Five databases were searched from inception to September 2024: PubMed, PEDro, Embase, SPORTDiscus, and the Cochrane Database of Systematic Reviews. The keywords “load”, “ankle”, “ankle instability”, “foot”, “biomechanics”, “kinetic”, “kinematics”, “motor control”, “force”, and “stability” were searched for using the Boolean operators AND and OR. The search strategy followed in the five databases is described in Appendix A.
2.4. Selection of Sources of Evidence
The articles retrieved from the databases were imported into Mendeley. These were then included in Rayyan, Rayyan Systems Inc., Cambridge, MA, USA (https://www.rayyan.ai/ [accessed on 5 September 2024]). Duplicates were identified and removed. The remaining references were screened by title and abstract by two reviewers. Full-text articles were retrieved when the initial review of the title or abstract suggested that the study was eligible or when there was insufficient information in the title or abstract to assess study eligibility. Full-text articles were independently assessed for eligibility by two review authors (SSM, LRP). Disagreements about study eligibility were resolved by discussion or adjudication by two other review authors (ABOA, PCG).
2.5. Data Items
The following data were extracted from all the full-text articles and entered into a standardized Microsoft Word document: the authors and the year of publication, the study population, the sample size, the type of dynamic exercise evaluated, and the evaluation methodology.
2.6. Critical Appraisal of Individual Sources of Evidence
Following current guidelines for conducting scoping reviews [24,25], it was not necessary to include an analysis of the methodological quality. Furthermore, the lack of a standardized tool for the methodological assessment of the studies included in this review makes such an analysis difficult. In this context, this review focuses on identifying ankle stability assessment methodologies, rather than on the results obtained.
3. Results
3.1. Selection of Sources of Evidence
A total of 1678 records were identified in PubMed, PEDro, Embase, SPORTDiscus, and the Cochrane Database of Systematic Reviews. After screening and removing duplicates, 1110 references remained. Of these, 196 were considered potentially eligible after reviewing the titles and abstracts, and the full texts of all were retrieved. After assessing the eligibility criteria, 32 studies were finally included. Figure 1 shows the PRISMA flow diagram.
3.2. Characteristics of Sources of Evidence
In total, 1142 subjects were included in the studies analyzed. Of these, 293 were female (25.6%) and 819 male (71.7%). One article [27] included 30 participants without specifying their gender (2.62%).
Regarding dynamic exercises, six categories were highlighted: analytical movements [28,29,30], functional movements [31,32,33,34,35,36,37,38,39,40], balance exercises [41], stair exercises [27,42,43], running [28,44,45,46,47,48,49], and walking [50,51,52,53,54,55,56,57,58]. The assessment methodologies included two- and three- dimensional motion capture systems, pressure platforms, force platforms, hand-held dynamometers, electromyography, acceleration sensors, instrumented treadmills, speed sensors, electromagnetic sensor motion capture systems, isokinetic dynamometers, inertial measurement units, and pressure sensors.
3.3. Synthesis of Results
Table 1 shows the assessment methodology in relation to the dynamic exercise carried out. Furthermore, Figure 2 graphically represents the distribution of the tools and exercises used for each pathology.
4. Discussion
The aim of this study was to determine the techniques with objective measurement instruments applied in vivo to assess ankle stability during dynamic exercise. The main results identified thirteen assessment methodologies, distributed into six exercise categories. The combination of 3D motion capture systems with multisegmental foot and ankle models, along with force and pressure platforms, appears to be the most suitable for assessing ankle stability during dynamic exercise.
4.1. Three-Dimensional Motion Capture Systems and Force-Pressure Platforms
Three-dimensional motion capture systems with markers are considered the standard for kinematic measurements [59]. Kishor Das et al. [60] highlighted their accuracy in detecting small differences in lower limb movements under various conditions. Gao Piming et al. [61] emphasized their superiority in analyzing dynamic ankle stability and understanding the mechanisms of the sprain and chronic instability. On the other hand, force-pressure platforms are widely used to assess ankle stability and functionality in kinetic terms [62]. Delahunt E et al. [63] applied force platforms to study load distribution and possible joint compensations in the lower limb. In contrast, authors such as Mckeon Po et al. [64] have pointed out that, although useful for identifying acute sprain risks, these tools are not able to adequately detect deficits related to chronic instability. However, the studies by Kyung et al. [55], Aali et al. [50], Farinelli et al. [53], Tajima et al. [56], Hashish et al. [47], and Moudy et al. [43] based this combination of assessment methodologies on their analysis of the lower limb in dynamic exercise, differing in their approaches and objectives, highlighting the complexity of capturing dynamic foot and ankle movements.
Kyung et al. used a 120 Hz 3D system together with a 50 Hz pressure platform to assess gait with the DuPont foot model [65,66] and studied intersegmental motion across different planes of movement [67,68]. Although the authors indicated that this model was detailed and had demonstrated good reliability, it was insufficient to detect small kinematic changes, showing a lack of sensitivity. They suggested the inclusion of refinements in marker-based systems combined with imaging techniques for more precise measurements. In contrast, Aali et al. used a marker placement system determined by Vicon Clinical Manager [69,70] with a 120 Hz 3D system and a 1200 Hz force platform, focusing on ground reaction forces and joint moments during walking. These authors did not report any lack of sensitivity in their results when applying this model.
In this regard, Farinelli et al. [53], using a similar configuration but with a 960 Hz platform, compared several multisegment foot models, such as the Heidelberg [71] and Oxford models [72], highlighting their ability to capture intrinsic foot and ankle movements that are often clinically significant. They critiqued the complexity of the marker placement required by these models, which can limit their practical use in gait analysis. Farinelli introduced the Distal Shank method [73] as a simplified alternative that can capture comprehensive foot power and work production more effectively, indicating that it is more accessible for clinical settings, especially in pathological cases or with children, where precise marker placement is difficult.
Tajima et al. employed the Vicon Plug-in-Gait model with a 200 Hz 3D system combined with a 1000 Hz force platform for running, without reporting any limitations in the model. However, these authors recognized the limitations of their trial sample size, noting that although three trials were analyzed, the literature suggests at least eight trials are necessary for stable values [74]. They justify their choice by referencing the reliability of kinematic and kinetic data, even with a reduced number of trials [75], though they acknowledge the potential influence of fatigue on the results. Moudy et al. also used the Plug-In-Gait body marker set, without reporting any limitations in this marker colocation system. They employed landmark registration for a waveform analysis, which increased the predictive power for performance indicators, though variability in the between-limb influence presented some challenges. Hashish used a dorsal tracking plate with skin-mounted markers affixed to the pelvic, thigh, shank, and foot segments bilaterally. The limitations noted were due to the short running path, but they did not report any inconvenience with the marker’s placement.
Edo et al. [30] and Tavakoli et al. [57] used 3D motion capture systems to assess foot and ankle kinematics. Edo et al. positioned markers on the lower limb using the Vicon Motion System. The validity and reproducibility of the method used to quantify kinematic coupling behavior were confirmed by previous studies [76]. On the other hand, Tavakoli et al. used a 3D motion capture system with reflective markers according to a single-segment model. As a limitation, they indicated that the use of a single-segment model did not specifically isolate ankle or rearfoot kinematics. However, they noted that making ground contact is a functional task for the whole foot and, initially, this model was considered appropriate. Finally, they specified that using a multisegment foot model would certainly further illuminate the kinematic events of the foot pre- and post-ground contact. Similar limitations were found in studies, such as those by Mattiussi et al. [37].
When comparing these approaches, it becomes evident that some models are more detailed in segmental foot analyses, which have been proven to be valid and reproducible by previous studies, but require precise marker placement and sophisticated setups, which may not be feasible in all settings. Farinelli’s method stands out for its clinical applicability, providing a balance between complexity and practical utility. These studies highlight the importance of the experimental setup, including the number of trials or inter-limb variability.
On the other hand, some authors, such as Balaji et al. [51] and Chow et al. [52], used pressure platforms at different frequencies to assess gait. Chow et al. measured the arch index, plantar load distribution, center of gravity, balance, and toe angle. Through static and dynamic plantar pressure analyses, they effectively assessed the load distribution in specific regions and the participants’ center of gravity balance, as well as transitions between these states. Finally, to counteract the limitations of their study, they suggested using electromyography to analyze the static and dynamic signals of the dominant leg during habitual movements and to explore the correlation between plantar load distribution, the center of gravity, and lower limb strength. Other authors, such as Malisoux et al. [36], who exclusively used force platforms to assess functional movements of the lower limb, similarly pointed out the limitations of the analysis in terms of force measurement and noted motion analysis systems or electromyography could have provided more information about biomechanical adaptations.
4.2. Electromyography
Electromyography allows for the analysis of muscle activation patterns, coordination, and fatigue, which are crucial for ankle stability [77]. Understanding this is essential, as altered or delayed muscle activation can increase the risk of sprains [78]. Authors such as Kessler et al. [34] and Son et al. [40] have used it in combination with other tools in their studies to assess functional exercises. However, although this technique is valuable, Qin P et al. [79] emphasize that studies using this tool exclusively on the lower limb are limited, mainly due to the influence of gravity, and recommend combining it with tools that measure kinetics and kinematics. Despite this, authors like Avila de Oliveira et al. [41] have exclusively used electromyography to evaluate balance exercises in the lower limb.
4.3. Instrumented Treadmills
Instrumented treadmills have recently been used due to their ability to analyze various functional aspects of the lower limb [80,81]. These treadmills allow for speed and incline adjustments, simulating diverse dynamic conditions [82]. Authors such as Coifman et al. [44] combined a 3D system with an instrumented treadmill featuring a 240 Hz sampling rate to assess running. However, other authors, such as Futrell et al. [45] and Hmida et al. [54], noted that despite this instrument’s ability to identify various parameters, such as specific gait phases, stride length and time, cadence, and pressure distribution, the constant speed used to standardize the gait during data collection may have reduced its external validity.
4.4. Handheld Dynamometer
The handheld dynamometer is a portable and accessible device in clinical practice that is used to assess ankle strength in different positions, making it useful for quantifying strength differences between both sides of the body [83]. However, according to Spink MJ et al. [84], its accuracy and reliability may be affected by variations between examiners, and it only measures isometric strength [85]. In contrast, the isokinetic dynamometer offers a more advanced assessment of muscle strength, allowing for the measurement of concentric and eccentric contractions throughout the movement, which improves its accuracy in evaluating fatigue, endurance, and strength imbalances [86]. Komatsu et al. [31] have used this dynamometer alongside 3D systems and force platforms to assess both functional and analytical movements.
4.5. Inertial Sensors
Another way to measure ankle stability is through sensors. Acceleration sensors, which measure forces along the X, Y, and Z axes [87], allow for the evaluation of the response to sudden changes in direction or speed. They have been used at frequencies of 50–1000 Hz alongside other tools by authors such as Baczkowicz et al. [29] to assess analytical movements. Pressure sensors, used by Yamamoto et al. [58] at frequencies of 200 Hz, estimate force and balance, especially when analyzing gait [88]. However, these authors pointed out that plantar pressure measurement systems are limited in that they only measure force perpendicular to the sensor surface. Therefore, other relevant forces, including shear force, cannot be measured. This system is not useful when the influence of other forces might be greater, such as in dynamic exercises, like turning or stop-and-go motions. Lastly, velocity sensors have been used by Petersen et al. [48] and DiLiberto FE et al. [42] to evaluate joint performance during stair exercises, combining them with 3D systems, force platforms, and motion capture using electromagnetic sensors, which allow for the assessment of ankle rotational movements with high sensitivity and angular precision, while being resistant to visual occlusion.
According to Franz Am et al. [89], this latest system offers advantages over 2D and 3D systems, such as position and orientation tracking with minimal processing, the detection of six degrees of freedom without requiring a direct line of sight, and simple digitization, as well as the ability to accurately capture rotational movements [90]. However, Clark R et al. [91] point out that its main limitation is its susceptibility to the distance between the transmitter and receiver and interference from elements that distort the electromagnetic field, such as metals or electrical devices. Although it provides detailed kinematic data, it does not collect kinetic data, which requires its combination with force or pressure platforms [92].
The latest tools identified are inertial measurement units, applied by Lundgren et al. [35] at frequencies of 120 Hz, combined with force platforms to evaluate functional movements. These units measure linear acceleration, angular velocity, and orientation in three dimensions [93], capturing movements with six degrees of freedom and providing real-time data on stability and balance [94]. Their cost-effectiveness makes them very useful; however, they present limitations, such as position drift due to signal noise. To correct this, authors such as Roger N et al. [95] have proposed the fusion of magnetometers and GPS, along with techniques such as extended Kalman filters.
4.6. Strengths and Limitations
The main limitation of this study stems from the variety and heterogeneity of the terms used; although this has been minimized by an extensive search including broad terms, some studies may not have been identified.
However, it has important strengths, most notably the methodology used, being the first study to determine and review techniques with objective measurement instruments applied in vivo to assess ankle stability during dynamic exercise. It provides information on current evaluative trends and the exercises in which these tools are used.
4.7. Clinical Implications
The findings of this review provide valuable guidance for clinicians in selecting the most appropriate tools for the dynamic assessment of chronic ankle instability (CAI). By highlighting the strengths and limitations of current methodologies, the review supports evidence-based decision-making in clinical settings. Integrating these methodologies, particularly when guided by the clinical context, may enhance the accuracy of diagnosis and the effectiveness of rehabilitation strategies. This comprehensive and context-driven approach could contribute to more personalized treatment plans and improved patient outcomes.
5. Conclusions
Thirteen objective measurement tools have been identified and applied in vivo across six categories of dynamic exercises to assess ankle stability, with 240 Hz 3D motion capture systems and 1000 Hz force platforms being the most used for kinematic and kinetic measurements. Functional exercises and walking are the primary activities for evaluation. The preferred method combines 3D motion capture with multisegmental foot models, such as force and pressure platforms, for comprehensive assessment, although the tool of choice varies based on the exercise type, resources, and scope of application.
Three-dimensional systems effectively evaluate multiplanar ankle movement but require a complex setup and model selection, while simpler 2D systems lack full spatial analyses. Force and pressure platforms offer accurate kinetic data, ideally paired with motion capture or electromyography to monitor muscle activation and fatigue. Instrumented treadmills enable controlled simulations but have limited external applicability. Electromagnetic sensors provide precise 3D rotation without visual obstruction, and inertial measurement units afford real-time stability data at a lower cost, though they suffer from signal noise. Isokinetic dynamometers assess muscle strength in both contraction phases, and velocity, acceleration, and pressure sensors contribute crucial data on movement dynamics. The integrated use of these tools supports effective injury prevention and rehabilitation.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Aparisi Gómez M.P. Aparisi F. Guglielmi G. Bazzocchi A. Particularities on Anatomy and Normal Postsurgical Appearances of the Ankle and Foot Radiol. Clin. N. Am.20236128130510.1016/j.rcl.2022.10.01336739146 · doi ↗ · pubmed ↗
- 2Dhillon M.S. Patel S. Baburaj V. Ankle Sprain and Chronic Lateral Ankle Instability: Optimizing Conservative Treatment Foot Ankle Clin.20232829730710.1016/j.fcl.2022.12.00637137624 · doi ↗ · pubmed ↗
- 3AlexandreÉ. Monteiro D. Sotto Mayor R. Jacinto M. Silva F.M. Cid L. Duarte-Mendes P. Assessing Functional Ankle Instability in Sport: A Critical Review and Bibliometric Analysis Healthcare 202412173310.3390/healthcare 1217173339273757 PMC 11395028 · doi ↗ · pubmed ↗
- 4Martin R.L. Davenport T.E. Fraser J.J. Sawdon-Bea J. Carcia C.R. Carroll L.A. Kivlan B.R. Carreira D. Ankle Stability and Movement Coordination Impairments: Lateral Ankle Ligament Sprains Revision 2021 J. Orthop. Sports Phys. Ther.202151 CPG 1CPG 8010.2519/jospt.2021.030233789434 · doi ↗ · pubmed ↗
- 5Medina Mc Keon J.M. Hoch M.C. The Ankle-Joint Complex: A Kinesiologic Approach to Lateral Ankle Sprains J. Athl. Train.20195458960210.4085/1062-6050-472-1731184957 PMC 6602390 · doi ↗ · pubmed ↗
- 6Miklovic T.M. Donovan L. Protzuk O.A. Kang M.S. Feger M.A. Acute lateral ankle sprain to chronic ankle instability: A pathway of dysfunction Physician Sportsmed.20184611612210.1080/00913847.2018.140960429171312 · doi ↗ · pubmed ↗
- 7Chang S.H. Morris B.L. Saengsin J. TournéY. Guillo S. Guss D. Di Giovanni C.W. Diagnosis and Treatment of Chronic Lateral Ankle Instability: Review of Our Biomechanical Evidence J. Am. Acad. Orthop. Surg.20212931610.5435/JAAOS-D-20-0014533347006 · doi ↗ · pubmed ↗
- 8Han J. Anson J. Waddington G. Adams R. Liu Y. The Role of Ankle Proprioception for Balance Control in relation to Sports Performance and Injury Bio Med Res. Int.2015201584280410.1155/2015/84280426583139 PMC 4637080 · doi ↗ · pubmed ↗