Severe Pyothorax Caused by Streptococcus pseudoporcinus and Prevotella buccae: A Case Report
Yuki Chiko

TL;DR
A rare case of severe pyothorax caused by two bacteria, Streptococcus pseudoporcinus and Prevotella buccae, is reported, highlighting their potential to cause serious infections.
Contribution
Reports a rare clinical case where two uncommon bacteria caused severe pyothorax, emphasizing their potential as serious pathogens.
Findings
Streptococcus pseudoporcinus and Prevotella buccae were isolated from pleural fluid in a case of severe pyothorax.
The case required mechanical ventilation due to the rapid progression of the infection.
The findings suggest β-hemolytic streptococci can cause severe infections even when rarely reported in such contexts.
Abstract
Pyothorax is a condition characterized by the accumulation of purulent pleural effusion and is often secondary to pneumonia or lung abscess. The identification of causative pathogens is essential for treatment; however, the sensitivity of pleural fluid culture remains low. We report a rare case of severe pyothorax requiring mechanical ventilation in which Streptococcus pseudoporcinus and Prevotella buccae were isolated from pleural fluid. This case highlights the potential for β-hemolytic streptococci to cause rapidly progressive and severe infections, even when rarely reported as causative organisms of pyothorax.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
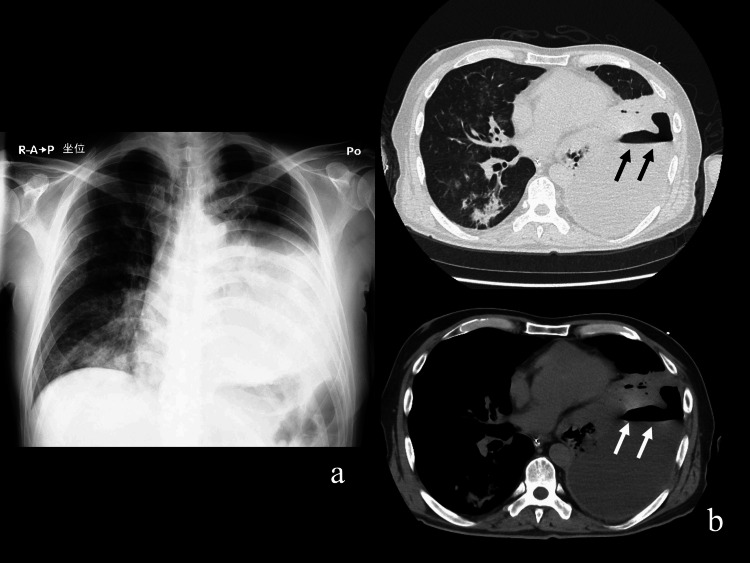 Figure 1
Figure 1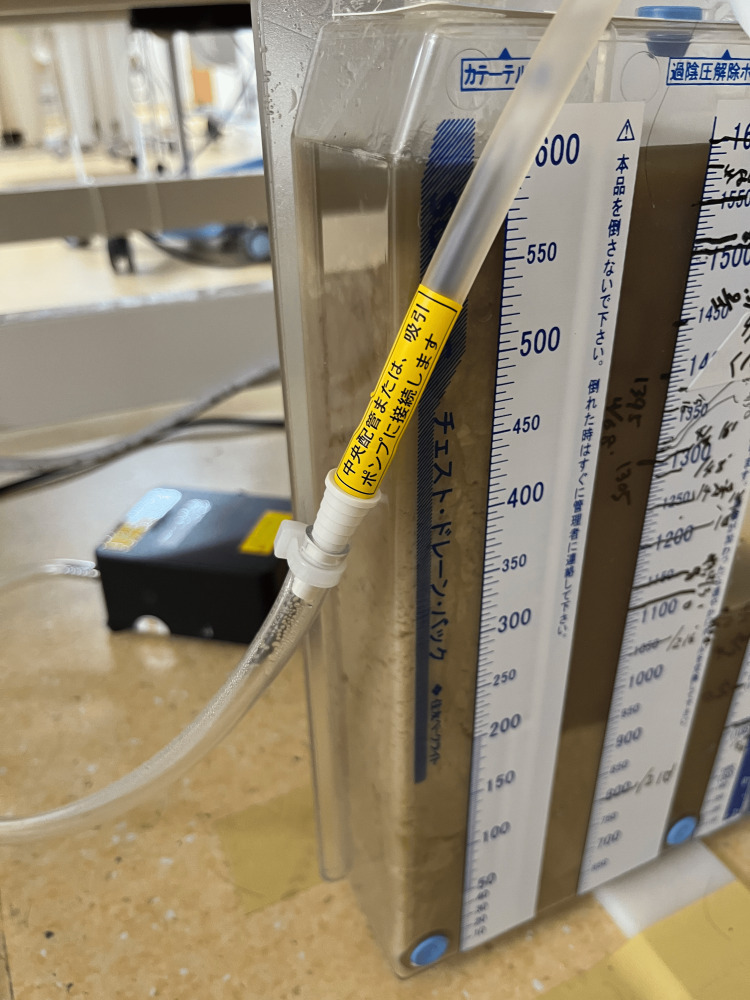 Figure 2
Figure 2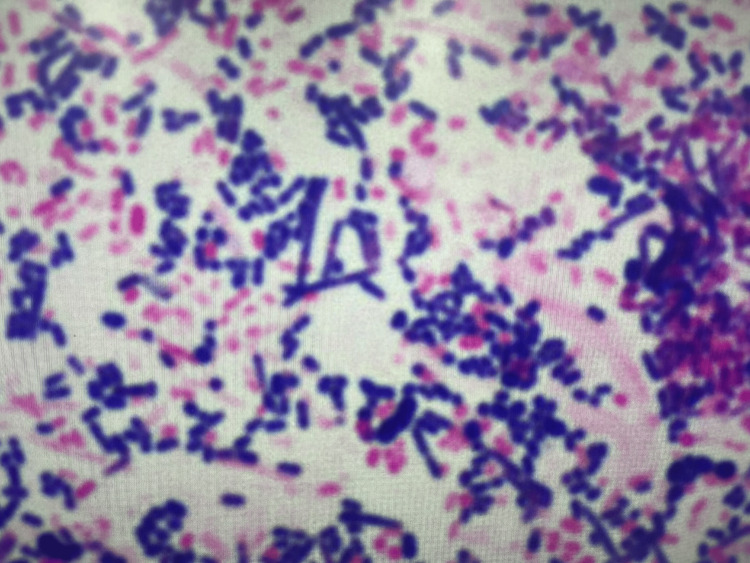 Figure 3
Figure 3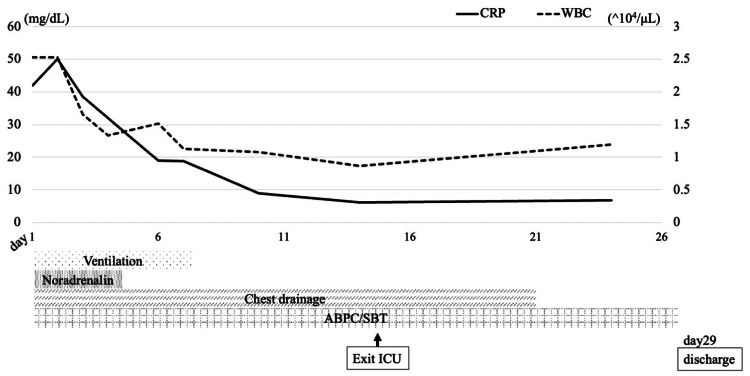 Figure 4
Figure 4| Values | Unit | Reference range | |
| Hematology | |||
| WBC | 25410 | /μL | 3300-8600 |
| Hb | 13.4 | g/dL | 13.7-16.8 |
| Hct | 30.6 | % | 40.7-50.1 |
| PLT | 56.0 | ×104/μL | 15.8-34.8 |
| Biochemistry | |||
| Glu | 214 | mg/dL | 73-109 |
| T-Bil | 0.4 | mg/dL | 0.4-1.5 |
| AST | 23 | IU/L | 13-30 |
| ALT | 21 | IU/L | 10-42 |
| LDH | 336 | IU/L | 124-222 |
| γ-GTP | 138 | IU/L | 13-64 |
| BUN | 26.5 | mg/dL | 8-20 |
| Cr | 1.65 | mg/dL | 0.65-1.07 |
| Na | 137 | mEq/L | 138-145 |
| K | 4.5 | mEq/L | 3.6-4.8 |
| Cl | 95 | mEq/L | 101-108 |
| Ca | 9.5 | mEq/L | 8.8-10.1 |
| Serology | |||
| CRP | 41.94 | mg/dL | 0.00-0.14 |
| BNP | 94.4 | pg/mL | 0.00-18.4 |
| Blood coagulation test | |||
| APTT | 47.3 | Seconds | 24.0-36.0 |
| PT | 15.8 | Seconds | 10.0-12.0 |
| PT-INR | 1.25 | 0.90-1.10 | |
| D-dimer | 2.8 | μg/dL | 0.0-1.0 |
| Appearance | Purulent | |
| pH | 6.86 | |
| LDH | 554 | IU/L |
| Glu | 1 | mg/dL |
| %Neu | 100 | % |
|
|
| ||||
| MIC | MIC | ||||
| PCG | ≤0.03 | S | PCG | ≤0.06 | S |
| ABPC | ≤0.12 | S | ABPC | ≤0.25 | S |
| AMPC/CVA | ≤1 | PIPC | ≤4 | S | |
| ABPC/SBT | ≤0.12 | ABPC/SBT | ≤1 | S | |
| CTX | 0.25 | S | PIPC/TAZ | ≤4 | S |
| CFPM | 0.5 | S | CMZ | 1 | |
| AZM | ≤0.12 | S | CTX | ≤2 | S |
| LVFX | 0.5 | S | VCM | >16 | |
| CTRX | ≤0.25 | S | IPM/CS | ≤0.5 | S |
| MINO | ≤0.12 | MEPM | ≤0.5 | S | |
| IPM/CS | ≤0.12 | CLDM | >8 | R | |
| MEPM | ≤0.25 | S | MFLX | 1 | S |
| VCM | 0.5 | S | |||
| EM | ≤0.12 | S | |||
| CLDM | ≤0.25 | S | |||
| ST | ≤10 | ||||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPleural and Pulmonary Diseases · Ultrasound in Clinical Applications · Amoebic Infections and Treatments
Introduction
Pyothorax is defined as the presence of visible pus in the pleural cavity and is typically a complication of pneumonia or lung abscess, accounting for approximately 80% of cases [1]. The identification of the causative microorganism is crucial for treatment planning. However, the sensitivity of standard pleural fluid culture is reported to be only 14%-21%, and many cases are treated empirically without definitive pathogen identification [2,3]. We report a rare case of pyothorax with severe respiratory failure, in which Streptococcus pseudoporcinus and Prevotella buccae were isolated from pleural fluid culture.
Case presentation
A man in his 60s presented with a one-month history of persistent cough and left-sided chest pain. Despite outpatient treatment at a local clinic, his symptoms progressively worsened, prompting referral to our hospital. The patient's medical history included chronic pancreatitis and diabetes mellitus; however, he had not been receiving regular treatment, as he had voluntarily discontinued hospital visits. Consequently, the timing of the onset of these conditions remained unclear.
On presentation, the patient's vital signs were as follows: body temperature, 35.5°C; heart rate, 134 beats per minute; blood pressure, 93/67 mmHg; respiratory rate, 58 breaths per minute; and oxygen saturation, 81% on room air. He was alert. Physical examination revealed decreased breath sounds in the left lung field, with no jugular venous distension or peripheral edema. Laboratory findings are summarized in Table 1.
Chest X-ray and computed tomography (CT) revealed a massive left-sided pleural effusion with pleural thickening and suspected gas formation (Figure 1). Due to severe respiratory failure, mechanical ventilation was initiated. Upon admission to the intensive care unit (ICU), chest tube drainage was performed, yielding a large amount of malodorous, turbid, purulent fluid (Figure 2). The pleural fluid analysis is summarized in Table 2. Gram staining demonstrated polymicrobial organisms (Figure 3). As the identification of the causative organism was considered important, the pleural fluid sample was inoculated into a blood culture bottle in addition to being submitted for a pleural fluid culture test. A routine blood culture and sputum culture were also obtained.
Imaging studies on admission.(a) Chest X-ray showing decreased radiolucency in the left thoracic cavity, suggestive of pleural effusion. (b) Chest computed tomography (CT) revealing a large left-sided pleural effusion with gas formation (arrow), consistent with empyema.
Pleural drainage bag.A large amount of purulent drainage with a foul odor has accumulated.
Gram staining of pleural effusion.Multiple bacterial species are observed.
Empiric antibiotic therapy with ampicillin/sulbactam (3 g every six hours) was initiated for the treatment of pyothorax. A few days after admission, S. pseudoporcinus and P. buccae were identified as the causative pathogens from two sets of blood culture bottles with pleural fluid cultures. The standard blood cultures remained negative. Sputum culture revealed multiple bacterial species suggestive of aspiration; however, no single predominant organism was identified. The susceptibility results for each of the bacteria are shown in Table 3. Gram staining revealed a large number of bacteria, and ampicillin/sulbactam was continued without de-escalation, considering the possibility of a mixed bacterial infection involving organisms other than these two species. The patient's condition gradually improved with continued antibiotic therapy. Circulatory support with noradrenaline was discontinued on hospital day 4. The patient was successfully extubated on day 8, the chest drain was removed on day 21, and he was discharged on day 29 after transitioning to oral antibiotic therapy using amoxicillin/clavulanic acid (Figure 4).
Clinical course.ABPC/SBT, ampicillin/sulbactam; ICU, intensive care unit; CRP, C-reactive protein; WBC, white blood cell
Discussion
Standard pleural fluid cultures have low sensitivity, often resulting in empirical treatment without identifying the pathogen [2,3]. The use of blood culture bottles for pleural fluid has been reported to increase the diagnostic yield up to 24%-58.5%, raising positive rates by approximately 15% [4]. In this case, the causative organism was identified through conventional culture; however, efforts to identify the pathogen should not be neglected, especially in severe cases. Pleural fluid culture using a blood culture bottle may be a useful option in such situations. In this case, two microorganisms were identified as the causative agents of the pyothorax. In cases of community-acquired empyema where the causative organisms are identified, the *Streptococcus milleri *group species account for approximately one-third of the cases, followed by anaerobic bacteria and Streptococcus pneumoniae [5]. The two bacterial species identified in this case are rare causes of empyema, and in particular, there are very few reports of S. pseudoporcinus as a causative pathogen.
The genus Prevotella comprises obligate anaerobic, Gram-negative, short rod-shaped bacteria that are part of the endogenous flora of the oral cavity and urogenital tract [6]. On the other hand, *S. pseudoporcinus *is a relatively recently identified β-hemolytic streptococcus, known to colonize the female genital tract [7]. The infection route in our case remained unclear due to the absence of sexual exposure, but pleural fluid culture confirmed its role as the pathogen. Reports of S. pseudoporcinus remain extremely limited to date, with documented human infections including skin and soft tissue infections [8], pregnancy-related bacteremia [9], infective endocarditis [10,11], and spontaneous bacterial peritonitis [12]. Only one previous case of empyema was reported, and that case also presented with severe disease [13]. Group A β-hemolytic streptococci are known to cause a rapidly progressive form of pleuritis/empyema termed "explosive pleuritis" [14]. Given that S. pseudoporcinus is also a β-hemolytic streptococcus, it may explain the severe disease course in this patient.
Conclusions
Streptococcus pseudoporcinus is an uncommon pathogen, and its role in pyothorax remains poorly understood due to the scarcity of reported cases. This case illustrates that S. pseudoporcinus, in conjunction with anaerobic organisms such as P. buccae, can lead to fulminant pyothorax and septic shock. Clinicians should be aware of this potential pathogen, especially in polymicrobial infections with a severe clinical course. Accurate microbial identification and the prompt initiation of appropriate antibiotic therapy are essential for patient recovery. Further accumulation of such cases is needed to better elucidate the pathogenicity and clinical characteristics of S. pseudoporcinus.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Predicting factors for outcome of tube thoracostomy in complicated parapneumonic effusion for empyema Chest Huang HC Chang HY Chen CW Lee CH Hsiue TR 75175611519991008448810.1378/chest.115.3.751 · doi ↗ · pubmed ↗
- 2Blood culture bottle culture of pleural fluid in pleural infection Thorax Menzies SM Rahman NM Wrightson JM 6586626620112145985510.1136/thx.2010.157842 · doi ↗ · pubmed ↗
- 3Blood culture bottle and standard culture bottle methods for detection of bacterial pathogens in parapneumonic pleural effusion Jundishapur J Microbiol Charoentunyarak S Kananuraks S Chindaprasirt J Limpawattana P Sawanyawisuth K 08201510.5812/jjm.24893 PMC 464431726587217 · doi ↗ · pubmed ↗
- 4Performance of the Bac T/Alert Virtuo Microbial Detection System for the culture of sterile body fluids: prospective multicentre study Clin Microbiol Infect She RC Romney MG Jang W Walker T Karichu JK Richter SS 9929962420182927446210.1016/j.cmi.2017.12.011 · doi ↗ · pubmed ↗
- 5The approach to the patient with a parapneumonic effusion Clin Chest Med Rahman NM Chapman SJ Davies RJ 2532662720061671681710.1016/j.ccm.2005.12.005 · doi ↗ · pubmed ↗
- 6Antimicrobial susceptibility profile of clinically relevant Bacteroides, Phocaeicola, Parabacteroides and Prevotella species, isolated by eight laboratories in the Netherlands J Antimicrob Chemother Boiten KE Notermans DW Rentenaar RJ 8688747920243839446010.1093/jac/dkae 043PMC 10984934 · doi ↗ · pubmed ↗
- 7Differentiating Streptococcus pseudoporcinus from GBS: could this have implications in pregnancy?Am J Obstet Gynecol Grundy M Suwantarat N Rubin M 490497220201910.1016/j.ajog.2019.01.21930690012 · doi ↗ · pubmed ↗
- 8Streptococcus pseudoporcinus bacteremia in a patient with skin and soft tissue infection. A case report and literature review Infez Med Papapanagiotou M Ioannou P Alexakis K Maraki S Papadokostaki E Kofteridis DP 3994033120233770138910.53854/liim-3103-14PMC 10495064 · doi ↗ · pubmed ↗