A Rare Synchronous Existence of Warthin's Tumour and Oral Cancer: A systematic review
Gargi Sarode, Swapnagandha Mahindre, Vini Mehta, Rahul Anand, Namrata Sengupta, Shruti Singh, Sachin Sarode

TL;DR
This paper reviews rare cases where Warthin's tumour and oral cancer occur together, highlighting the importance of accurate diagnosis to avoid mismanagement.
Contribution
The study systematically reviews and analyzes the rare synchronous occurrence of Warthin's tumour and oral squamous cell carcinoma.
Findings
13 papers with 17 cases of synchronous Warthin's tumour and oral cancer were identified.
Over 50% of cases had a history of tobacco use, and many involved cervical lymph nodes.
No recurrence was reported in the follow-up of these cases.
Abstract
Oral squamous cell carcinoma (OSCC) is a common malignancy, while Warthin's tumour (WT) is a benign salivary gland neoplasm, typically found in the parotid gland but rarely involving extra-parotid tissues. The synchronous occurrence of OSCC and extra-parotid WT is particularly unusual. Accurate identification of these pathologies is crucial, as their rare presentation can resemble metastasis in lymph nodes. This review systematically searched for case reports and series of synchronous WT and OSCC, including 13 papers having 17 cases. The quality of these cases was assessed using CARE guidelines. The findings described WT's histological features and location in patients with OSCC, with many cases involving cervical lymph nodes. Over 50% of the cases had a history of tobacco use. Follow-up showed no recurrence in the reported cases. Awareness of the synchronous occurrence of WT and OSCC…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
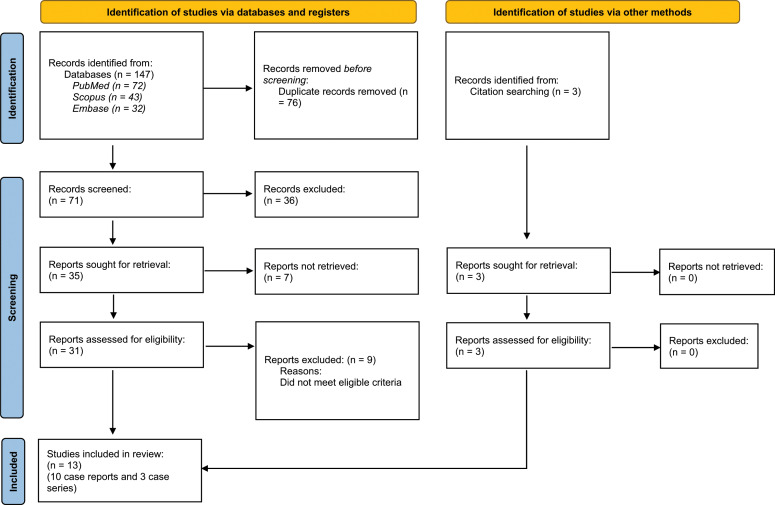 Fig. 1
Fig. 1| Site of OSCC | Site of Warthin’s Tumour | Number of Cases | |
|---|---|---|---|
| Tongue | Parotid gland (4 cases) | Peri-parotid lymph node | 1 |
| Tongue | Tail of parotid gland | 1 | |
| Buccal mucosa | Tail of parotid | 1 | |
| Buccal mucosa | Lower lobe of parotid gland | 1 | |
| Floor of mouth | Submandibular gland (3 cases) | Submandibular gland | 1 |
| Retromolar triangle | Submandibular gland | 1 | |
| Maxillary gingiva | Submandibular gland | 1 | |
| Tongue | Cervical lymph nodes (10 cases) | Cervical lymph node | 1 |
| Lower lip | Cervical lymph node | 1 | |
| Buccal mucosa | Level II lymph node | 1 | |
| Buccal mucosa and gingiva | Cervical lymph node | 1 | |
| Floor of mouth | Level II lymph node | 1 | |
| Tongue | Level II lymph node | 2 | |
| Lower gingiva | Level II lymph node | 1 | |
| Mandible | Level II lymph node | 1 | |
| Gingivobuccal complex | Level II lymph node | 1 | |
|
|
| ||
| Synderman | Sato | Demir | Shehan | Nupehewa | Schwarz | Enomoto | Iwai | Bhatlawande | Sato | Yang | Gontarz | Goh | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Selection | |||||||||||||
| 1. Does the patient(s) represent(s) the whole experience of the investigator (centre), or is the selection method unclear to the extent that other patients with similar presentation may not have been reported? | NO | YES | YES | NO | YES | YES | YES | NO | YES | NO | NO | YES | YES | |
| 2 | Ascertainment | |||||||||||||
| 2. Was the exposure adequately ascertained? | NO | YES | NO | YES | YES | YES | NO | NO | YES | NO | NO | YES | YES | |
| 3. Was the outcome adequately ascertained? | YES | YES | YES | YES | YES | YES | YES | YES | YES | YES | YES | YES | YES | |
| 3 | Causality | |||||||||||||
| 4. Were there other alternative causes that may explain the observation ruled out? | YES | YES | NO | YES | YES | NO | YES | NO | YES | NO | YES | YES | YES | |
| 5. Was there a challenge/rechallenge phenomenon? | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | |
| 6. Was there a dose-response effect? | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | |
| 7. Was follow-up long enough for outcomes to occur? | YES | YES | NO | YES | NO | NO | NO | YES | NO | YES | YES | YES | YES | |
| 4 | Reporting | |||||||||||||
| 8. Is the case(s) described with sufficient details to allow other investigators to replicate the research or to allow practitioners to make inferences related to their own practice? | YES | YES | NO | YES | YES | NO | YES | NO | YES | YES | YES | NO | YES | |
| Item | ||
|---|---|---|
| Number | Section | n (%) |
| 1 | Title | 6 (46.15) |
| 2 | Keywords | 7 (53.84) |
| 3a | Abstract | 11 (84.61) |
| 3b | Case representation | 13 (100) |
| 3c | Conclusion-What were the main ‘takeaways’ from this case? | 12 (92.30) |
| 4 | Introduction | 5 (38.46) |
| 5a | Patient information | 13 (100) |
| 5b | Main symptoms of the patient | 13 (100) |
| 5c | Medical, family and psychosocial history-including diet, lifestyle and genetic information whenever possible and details about relevant comorbidities and past interventions and their outcomes | 13 (100) |
| 6 | Clinical findings | 13 (100) |
| 7 | Timeline | 6 (46.15) |
| 8a | Diagnostic assessment | 13 (100) |
| 8b | Diagnostic challenges | - |
| 8c | Diagnostic reasoning | 11 (84.61) |
| 8d | Prognostic characteristics | 8 (61.53) |
| 9a | Therapeutic intervention | 12 (92.30) |
| 9b | Administration | - |
| 9c | Changes in intervention | - |
| 10a | Follow-up and outcomes | 9 (69.23) |
| 10b | Important follow-up test results | 9 (69.23) |
| 10c | Intervention adherence and tolerability | - |
| 10d | Adverse and unanticipated events | 3 (23.07) |
| 11a | Discussion | |
| 11b | Relevant literature | 12 (92.30) |
| 11c | Rationale for conclusions | 11 (84.61) |
| 11d | Main ‘takeaway’ of this case report | 12 (92.30) |
| 12 | Patient perspective | - |
| 13 | Informed consent | 2 (15.83) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSalivary Gland Tumors Diagnosis and Treatment · Cancer Diagnosis and Treatment · Tumors and Oncological Cases
1. Introduction
Oral cancer is a substantial contributor to global mortality, ranking among the most prevalent malignancies that profoundly affect the population worldwide.^1^ The diagnosis and management of this condition can be complicated by the presence of second primary lesions. Patients with head and neck squamous cell carcinoma (HNSCC) exhibit an increased incidence of second primary lesions, with rates exceeding 2–3% annually. This suggests that these lesions may occur alongside other benign or malignant neoplasms.^2^ Second primary tumours (SPTs) can be classified as either synchronous or metachronous. Synchronous tumours are identified as those detected within 26 weeks of the primary tumour, while metachronous tumours are diagnosed more than 26 weeks after the initial diagnosis of the primary tumour.^3^ Metachronous SPTs (20–30%) are more commonly identified than synchronous ones (1–6%) in HNSCC cases. The most frequently affected sites include the head and neck, pulmonary and oesophageal mucosal regions. These areas are exposed to carcinogens such as tobacco and alcohol, which are suspected to display the phenomenon of field cancerisation.^345678910^
The occurrence of contemporaneous neoplasms in the parotid or any major salivary gland, is an extremely rare event. The risk factors for oral squamous cell carcinoma (OSCC) comprise deleterious habits such as tobacco chewing and smoking, alcohol consumption and the use of betel nuts and betel quid. Additionally, there is a direct or indirect association with various oncoviruses, including human papillomavirus (HPV) and Epstein-Barr virus (EBV). Warthin's tumour (WT), also known as papillary cystadenoma lymphomatosum, is a benign tumour of the salivary glands, primarily affecting the parotid gland. It is one of the most common benign neoplasms of the parotid gland and the most common, bilaterally-occurring neoplasm in this region.^11^ The main predisposing factors for WT include tobacco smoking, exposure to various forms of radiation and viral infections such as those caused by EBV. Cases of synchronous associations between WT and OSCC are rarely seen and documented in the literature.
Thus, there is a rare occurrence of WT at a site different from the primary OSCC, which may mimic a metastatic lesion of the primary OSCC. This necessitates the accurate diagnosis of coexisting neoplasms for effective patient management. Therefore, the current paper presents a systematic analysis of all documented cases of synchronous OSCC and WT in the available medical literature, with a focus on their clinical and histopathological features. It also elaborates on the rare possibility of the occurrence of WT in extra-parotid sites, usually in cervical lymph nodes.
2. Methods
2.1. Focused question
Participants, Intervention, Control and Outcomes (PICO) protocol, as advocated in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA),^12^ were utilised to frame a focused research question: What are the complications, recurrence rates and prognosis following intervention in patients with the synchronous occurrence of OSCC and WT? This systematic review was registered with PROSPERO (registration number: 425093).
2.2. Inclusion and exclusion criteria
Clinical trials (both randomised and non-randomised), cross-sectional studies, case reports (CRs), observational studies (retrospective and prospective), case series (CS) and grey literature (including conference proceedings and non-academic websites) were reviewed. Articles in all languages were considered, and Google Translate was used to translate studies as needed. This review included only those patients who have been diagnosed radiologically and histopathologically with both OSCC and WT.
Non-human subjects, reviews, commentaries and letters to the editor were excluded from this review. Cases of OSCC associated with other neoplasms, WT in conjunction with other neoplasms and inapt studies deemed as non-CRs, such as reviews, commentaries or clinical trials, were also excluded from the present review.
2.3. Literature search
Two investigators (SM and GS) independently conducted a comprehensive search of various databases. An electronic search was piloted using the following databases: PubMed, Scopus and Web of Science. Google Scholar was used to explore grey literature, focusing on cases involving coexisting WT and OSCC. The medical subject headings (MeSH) used were as follows: (Warthin's tumour) OR (papillary cystadenoma lymphomatosum) AND (oral cancer) OR (OSCC) AND (diagnosis) OR (prognosis) OR (recurrence). Cross-referencing of the included articles was also executed to find any further studies satisfying the inclusion criteria. Disparities were resolved through discussions between the investigators regarding the inclusion/exclusion of specific papers. The inter-examiner reliability was assessed using a Kappa score to evaluate the agreement between the examiners.
2.4. Data extraction
The data tabulation was conducted by two investigators independently based on the following criteria: the number of participants, the number of cases with WT occurring synchronously with OSCC as described in each study, chronological age (including mean, median or range) and the gender of the patients. Additionally, characteristic features such as histological, radiographic and clinical features were noted, along with any outcomes related to WT synchronous with OSCC and follow-up information. Details regarding treatment, recurrence rates, complications and prognosis were also recorded.
2.5. Quality assessment
Quality assessment for CR and CS was done based on CARE (CAse REport) guidelines.^13^ Various characteristics were evaluated, such as the title, keywords, quality of the abstract, introduction, reported patient information, clinical findings, timeline, diagnostic evaluation, reported interventions, follow-up and outcomes, quality of the discussion section, patient perspectives and the inclusion of informed consent and approval from the scientific and ethics committee.
During the preparation of this work, the authors used ChatGPT to refine the language in a few sections of the paper. After employing this tool/service, the authors thoroughly reviewed and edited the content as needed and took full responsibility for the publication's content.
3. Results
3.1. Literature search
The initial literature search on the topic yielded 3,264 papers. Subsequently, 3,209 irrelevant papers were excluded. The abstracts and titles of 55 papers were studied for possible annexation, resulting in the exclusion of 42 papers. Consequently, 13 articles with full texts were considered for possible inclusion. Ultimately, 13 studies—encompassing 10 CRs^14161718192021222324^ and three CS^152526^—were included in the present review. No further studies were uncovered in the reference lists of the comprised articles. The literature search is illustrated in the PRISMA flowchart, which includes the exclusion criteria for the selected articles [Fig. 1].
PRISMA 2020 flow diagram.
3.2. General characteristics of the included studies
WT synchronous with OSCC was identified in 17 patients across the included studies.^14151617181920212223242526^ In 13 of these studies, a male preponderance was observed, with almost twice as many females (M: 11, F: 6).^14151617181920212223242526^ The age of the patients ranged from 42 to 86 years, with a mean age of 64 years. The majority of cases presented with a history of tobacco chewing,^141622^ smoking^14192122232426^ and alcohol consumption.^1422^ One case reported deranged liver function tests, which can occur in patients with synchronous pathologies who have a history of alcohol consumption.^22^ Additionally, a single case documented a history of hepatitis C lasting 11 years.^16^
Most cases described the primary finding as OSCC with ulcerative lesion^142122232426^ and enlarged lymph nodes.^1415202223^ In one case, sensory disturbance of the left lower lip was reported.^20^ One patient complained of a burning sensation and limited mouth opening.^22^ The sites of OSCC included the tongue,^1519212526^ buccal mucosa,^14162526^ floor of the mouth,^2425^ buccal mucosa and gingiva,^16^ lower lip,^17^ retromolar triangle,^18^ mandible,^20^ mandibular gingivobuccal complex,^22^ maxillary gingiva^23^ and mandibular gingiva^25^ [Table 1 and 2]. The sizes of the lesions mentioned were 10 mm × 5 mm^16^ 5 cm × 4 cm,^14^18 mm × 13 mm,^21^ 30 mm × 15 mm,^24^ 4 cm × 4 cm^26^ and 2 cm × 2 cm.^26^ The TNM staging of OSCC was reported as T2N2M0,^19^ T4N1M0,^20^ T2N0M0,^21^ T4aN2bM0,^23^ two cases of T3N1M0^25^ and two cases of T2N1M0.^25^ In some reports, the grading of OSCC was noted as well-differentiated squamous cell carcinoma,^1722^ moderately differentiated^1626^ and poorly differentiated.^14^
The majority of the cases described histologically involved WT in the lymph nodes.^141619202122232426^ The sites of the WT were identified in the cervical lymph nodes,^16171920212225^ submandibular lymph nodes,^1823^ the peri-parotid region,^15^ the tail of the parotid gland^1426^ and the submandibular gland^24^ [Table 1 and 2]. The histological findings typically included cystic spaces lined by bilayered cuboidal and columnar epithelium, as mentioned in most cases.^141619202122232426^ Additionally, an epithelial arrangement accompanied by lymphoid aggregate was also noted.^14162021222326^ The sizes of the WT varied, with measurements reported as 12 mm × 8 mm × 6 mm,^16^ 1.45 cm,^20^ 5 mm × 3 mm, 4 mm × 3 mm^23^ and 6 mm,^24^ ranging from 3 mm to 1.45 cm, with a mean size of 8.3 mm.
The investigations conducted included incisional biopsy,^14^ excisional biopsy^16212226^ and excisional biopsy in conjunction with computed tomography (CT) scan.^1621^ Contrast-enhanced CT showed an enlargement of the cervical LN (15 mm × 11 mm × 10 mm) at the contralateral level.^21^ Ultrasound demonstrated a 12 mm × 8 mm × 6 mm hypoechoic mass adjacent to the anterior border of the sternocleidomastoid muscle and posteriorly to the external jugular vein.^16^ A positron emission tomography (PET)/CT scan was performed in several cases,^192023^ with intense radiotracer uptake observed at the resection site, yielding a maximum standardised uptake value (SUV max) of 5.2 in one case.^19^ Additionally, a magnetic resonance imaging (MRI) scan was performed in one of the studies. Fine-needle aspiration cytology (FNAC) reported the presence of red blood cells (RBCs) and inflammatory cells in one case.^21^ FDG-PET/CT scans were also conducted in several instances,^192123^ revealing intense FDG uptake (SUV max 9.5 and 5.7) in the enlarged LN at Level II ipsilaterally.^19^ The SUV max of the primary site and the contralateral cervical LN were 2.2 g/mL and 3.7 g/mL, respectively,^21^ with an SUV max of 19.96 noted. Furthermore, SUV max values of 6.8, 8.17 and 5.1 were reported in the right submandibular LN,^23^ along with an SCC antigen value of 3.3 ng/ml.^23^
The details of various features, including clinical, histological and radiographic characteristics of the WT synchronous with OSCC, are comprehensively described in Table 1.
3.3. Management, recurrence rate and postoperative complications
Four cases described the excision of OSCC at the site and supra-omohyoid neck dissection as a treatment option.^17192025^ Seven cases underwent excision of the OSCC site followed by modified radical neck dissection.^14182223242526^ Three cases reported receiving radiotherapy after excision.^162425^ Follow-up was documented in three studies, which included six cases with follow-up durations of 6 months, 18 months, 24 months, 28 months, 35 months and 46 months.^171825^ No recurrence was observed in four patients.^21232426^ Recurrence of OSCC in the buccal mucosa was noted in one case,^16^ which was subsequently treated with radiotherapy. Additionally, one case reported death due to chemotherapy.^26^ One study concluded that OSCC is a key prognostic determinant in such cases and may majorly complicate postoperative management.^18^
3.4. Quality assessment
In six studies (46.15%), the title was specified as the type of study,^141618222526^ while in five studies, keywords were used as CR and CS.^1619232426^ The principal outcomes were adequately reported in the abstracts of seven studies.^14182123242526^ Conclusions were included in the abstracts of around four studies.^18242526^ The main findings were reported moderately in the abstracts of six studies.^141823242526^ A satisfactory introduction was available in five studies.^1423242526^ Patient information without identification was provided in 13 studies.^14151617181920212223242526^ The main symptoms and findings of the patients were described in 10 cases.^14161819202122232426^ Other findings, such as medical and family history, along with psychosocial and genetic aspects, were not mentioned in any of the included studies, except for one that provided partial information.^16^ A past interventional history was provided in two cases.^1920^ In four CRs, adequate details about the physical examination of the patients were provided.^16222526^ The treatment timeline for the included patients was not reported in any of the studies.
Diagnostic testing was carried out sufficiently in seven cases.^16192021222326^ While the specialists did not report any challenges encountered during the diagnostic assessment, all provided a specific diagnosis for the cases. Adequate information regarding prognosis and/or staging was specified in about 10 cases.^141617181920212223242526^ Information on surgical intervention or radiotherapy was sufficiently provided in 12 cases.^141617181920212223242526^ However, in one case, no details or level of surgical intervention were mentioned.^15^ Additionally, none of the CRs or CS indicated any deviations from the original treatment strategy. Patient- or clinician-reported outcomes were noted in seven cases.^14212223242526^ Adequate information about follow-up details was available in seven cases.^1618212223242526^ Adherence to and tolerability of the follow-up were reported in three cases.^141619^ Data regarding postoperative complications were provided in about three cases.^162026^ An assessment discussion section revealed that limitations and weaknesses were described in about 10 studies.^14151620212223242526^ The related literature was discussed adequately in 12 studies.^1415161819202122232425^ In all the CRs, the conclusions were reasonable and adequately justified.^14161820212223242526^ Recommendations or ‘takeaways’ were provided in 12 cases.^1415181920212223242526^ Patient perspectives were not mentioned in any of the studies, and information regarding patient consent and ethics was addressed in only two cases.^2326^ A detailed description is provided in Table 3.
4. Discussion
In this systematic review, a total of 13 papers were included, documenting 17 cases of synchronous existence of WT and OSCC. The clinical manifestations, TNM staging and OSCC grades were reported in these papers. Reports of sensory disturbances, burning sensations and limited mouth opening indicate that OSCC can lead to various symptoms that may adversely affect the patient's quality of life. Additionally, the results suggest that WT can occur concurrently with OSCC. Given that tobacco use is a common aetiological factor for both OSCC and WT, patients with a known history of such habits should be prioritised for regular oral cancer screenings and assessments of lymph node involvement, especially in cases of regional metastasis and its diagnosis.
The results presented describe the histological features and sites of WT in individuals who also had OSCC. Most studies have documented the histological findings of WT, particularly in the affected lymph nodes. Although WT is typically found exclusively in the parotid gland, this review noted its presence in various locations, including cervical lymph nodes, submandibular lymph nodes, the peri-parotid region, the tail of the parotid gland and the submandibular gland.^14151617181920212223242526^ The histological characteristics of WT were defined by a cystic space lined with bilayered cuboidal and columnar epithelium, along with an epithelial arrangement featuring lymphoid aggregates. These findings are consistent with the typical histological appearance of WT observed in the parotid gland.
Warren and Gates have studied multiple primary malignant tumours (MPMTs) and proposed detailed criteria for diagnosing these types of tumours.^27^ According to their criteria: (1) each tumour must be histologically diagnosed as malignant; (2) each tumour must be geographically separate and distinct; and (3) metastasis resulting from prior cancer must be excluded. International guidelines have been established to elaborate on these criteria. Tumours develop in an organ, and a pair of organs or tissue should be considered a single tumour. However, there are two exceptions to this rule: (1) In any individual, systemic cancers involving multiple different organs should be regarded as one Tumour; and (2) Histologically different cancers, even if diagnosed at the same site, should be considered multiple tumours.^27^
The reported incidence of MPMTs ranges from 0.52% to 11.7%. Formerly, the pathogenesis of MPMTs was attributed to the phenomenon of field cancerisation, which posits that the aetiology of multiple oral primary carcinomas developing independently is due to pervasive exposure of epithelial cells to carcinogens. However, recent literature supports an alternative theory, suggesting a common clonal origin.^28^
A similar set of criteria should be proposed and followed to diagnose WT synchronous with OSCC. Both neoplasms show histologically distinct characteristics and should be geographically separate and distinct. Due to the proximal association of such a salivary gland tumour and regional lymph nodes, particularly in the case of WT, these lesions may clinically present with features of lymph node enlargement. This can lead to a misdiagnosis of metastatic lymph nodes in OSCC patients, further complicating their treatment plans. Nearly 90% of all oral cancers are OSCCs, with 40% of these cases revealing nodal metastasis.^29^ Therefore, associated practitioners (such as radiologists, head and neck surgeons and pathologists) should be well-informed about these infrequent findings to prevent overtreatment in such cases. Extra-parotid WTs are usually found accidentally during neck dissections in approximately 1% of oral cancer patients, and they can resemble metastatic lesions, particularly on PET/CT imaging.^25^ This ambiguity can be mitigated by using fine needle aspiration cytology. Misclassifying WT as metastatic lesions can result in overdiagnosis, leading to unnecessarily extensive treatment planning. The involvement of lymph nodes by WT generally has a better prognosis compared to lymph node involvement due to OSCC metastasis.^30^
The synchronous occurrence of WT with other benign neoplasms, such as oncocytoma, pleomorphic adenoma and sebaceous lymphadenoma as well as malignant neoplasms like lymphoma, has been reported in the literature.^22^ The coexistence of WT with neoplasms like oncocytoma may be attributed to shared aetiological, biological and clinical features.^26^ There are two primary theories regarding WT development: The first hypothesis, related to heterotopia, suggests that the tumour arises from proliferating salivary gland ductal cells that become entrapped in the lymph nodes of the parotid gland during embryonic development. This may explain the absence of WT occurrences in the lower neck levels, specifically Levels IV and V. The second theory proposes that WT primarily develops in the lymph nodes of the parotid gland in response to a stimulus like tobacco smoking.^31^ This theory accounts for the eightfold higher incidence of WTs in smokers compared to non-smokers.^32^ Moreover, there is a general observation of a correlation between smoking and tobacco consumption habits within the male population, which may elucidate the gender predilection observed in this systematic review. This review describes the synchronous occurrence of WT and OSCC in a total of 17 cases, with male predilection and a mean age of 64 years. The deleterious habit of tobacco consumption, whether in the form of chewing or smoking, was recorded in the medical history of almost all patients.
Smoking has a proven connotation with WT development, as evidenced by the literature. In a retrospective analysis of 96 patients diagnosed with WT, about 79% reported a history of cigarette smoking.^33^ This habit leads to oxidative destruction in the mitochondrial DNA of cells, especially oncocytic cells, which contributes to the tumorigenesis of WT. It has been reported that smokers are at an eightfold increased risk of developing this neoplasm compared to non-smokers.^34^ The main etiological factor for OSCC is also tobacco use. A significant correlation exists between the occurrence of WT and OSCC, particularly due to the habit of smoking tobacco. The carcinogens present in smoke mix with saliva and retrogradely enter the ducts of the salivary glands, resulting in metaplasia of the salivary ducts.^14^ The finding that 74.8% of WT patients are smokers supports this hypothesis.^35^ Consequently, the carcinogens from tobacco smoke affect both salivary ductal cells and oral mucosal cells simultaneously, which may elucidate the synchronous occurrence of WTs and OSCC.
The genetic analysis of WT is crucial for understanding its etiopathogenesis and its connection to OSCC, as reported in this systematic review.^36^ Recently, the t(11;19) translocation and its CRTC1/MAML2 fusion transcript have been identified in a few cases of WT, which share similarities with mucoepidermoid carcinoma (MEC), a salivary gland malignancy. This suggests a potential common genetic link between a WT and carcinoma.^37^ Conversely, Sharma et al. reported alterations at 17p13.1 (TP53), 9p21.3 (CDKN2A), 9q34.3 (NOTCH1) and 3q26.32 (PIK3CA), along with 24 other genetic loci, in OSCC patients with a history of smoking.^32^ Several genetic aberrations associated with smoking are also commonly observed in both OSCC and WT. Therefore, there is significant potential to further investigate the genetic and epigenetic factors shared by WT and OSCC in their etiopathogenesis.
There is considerable controversy surrounding the role of oncoviruses in the pathogenesis of OSCC and WT. WT is known to be associated with EBV.^38^ Although there is no direct correlation between EBV and OSCC, evidence in the literature suggests an association between the two.^39^ EBV-associated oral cancers are comparatively rare despite the oral cavity being a known site for the presence and transmission of EBV. However, the oral cavity can serve as a primary location for the virus, which may subsequently seed malignancies at other extraoral sites, such as the nasopharynx or gastrointestinal regions. Consequently, the role of EBV in its associated cancers is multifactorial, requiring the presence of other genetic aberrations and coexisting infections, particularly those caused by HPV.
EBV infection is considered a critical factor in tumorigenesis and is directly associated with the rapid progression of the disease and its metastatic tendency. EBV detection in OSCC is very rare and probably challenging because of its well-documented ‘hit-and-run’ phenomenon. Consequently, incomplete viral associations are often reported. There is evidence suggesting that EBV exerts bystander oncogenic effects on the tumour microenvironment. Additionally, the loss of EBV during the evolution of the neoplasm or the progression of the disease has been proposed. EBV-induced epigenetic reprogramming enables the virus to maintain oncogenic phenotypes even in the absence of the virus itself or its gene expression. Thus, future analyses are necessary to elucidate the definitive role of EBV in the pathogenesis of OSCC and to identify virus-associated biomarkers for OSCC management.^39^ Furthermore, HPV has lately been suggested to play an important role in the pathogenesis of WT.^35^ Conversely, the International Agency for Research on Cancer has stated that there is substantial evidence linking HPV type 16 to OSCC.^40^ Notably, over a 20-year period, the percentage of HPV-positive OSCC cases in the USA and European countries increased from <20% to >70%.^41^
The studies included in the systematic review discussed various investigation techniques, including biopsy, CT scans, contrast-enhanced CT, ultrasound, MRI, PET/CT scans and FDG-PET/CT scans. PET/CT is frequently used during the follow-up of cancer patients. WT demonstrates high FDG uptake, which can lead to the misdiagnosis of cervical lymph node metastases. In such cases, FNAC is valuable for evaluating salivary gland tumours. The diagnostic accuracy of FNAC for detecting salivary gland neoplasms, especially WT, is high (74–100%).^42^ WT is a benign, slow-growing tumour.^43^ Therefore, surgeons may opt for a conservative management approach after diagnosis with FNAC.
Detecting the synchronous occurrence of WT and OSCC presents a real diagnostic challenge for both radiologists and surgeons. Cervical lymph nodes and the tail of the parotid gland are among the most conventional sites for metastasis from primary OSCC. Conversely, the incidence rate of 1.3% was found to be with extra-parotid WTs in the neck specimens of OSCC patients. Thus, these tumours can lead to inaccurate staging of OSCC. Moreover, false-positive results from FDG-positive WT contribute to the risk of misdiagnosis. Therefore, CT/ultrasonography-guided FNAC may be beneficial in distinguishing WTs from OSCC metastasis.
The treatment of synchronous WT and OSCC requires careful planning and consideration of various factors, including the location and extent of the lesions, the stage of the cancer and the patient's overall health. The existing literature indicates that the most common treatment modality for synchronous WT and OSCC is the surgical removal of the primary tumour along with the involved lymph nodes. The extent of neck dissection varies based on the location and size of the tumour, with supraomohyoid neck dissection and modified radical neck dissection being the most frequently performed procedures. In some cases, adjuvant radiotherapy may be required to reduce the risk of recurrence.^141617181920212223242526^ The follow-up period for patients with synchronous WT and OSCC is critical, and close monitoring is necessary to detect any signs of recurrence. The prognosis for patients with synchronous WT and OSCC is generally favourable if the lesions are detected and treated early. However, the prognosis may be poor in the advanced stages of the disease or in the presence of underlying comorbidities. The available literature on synchronous WT and OSCC is notably limited, highlighting the need for further studies to determine the most effective treatment strategies and long-term outcomes for patients with this rare combination.
4.1. Limitations and future scope
The rarity of the synchronous occurrence of WT with OSCC presents a significant limitation that hinders the ability to perform a meta-analysis on this topic. Moreover, the results cannot be generalised due to the limited number of cases included in this study. This review acknowledges the possibility of selection bias, as only CRs and CS were considered. CR and CS presentations often show heterogeneity in terms of clinico-pathological, radiological, management and prognostic data, which limits the findings’ comparability. There is a pressing need for original research involving larger sample sizes to yield meaningful results regarding this rare pathology. Such research should also encompass the genetic and molecular characterisation of WT in conjunction with OSCC as well as the development of targeted therapies. Given the diagnostic challenges, future studies should prioritise the identification of accurate imaging techniques.
Conclusions
The rare occurrence of synchronous WT at a site different from the primary tumour can mimic a metastatic lesion originating from the primary OSCC. This presents a serious diagnostic challenge and may result in mismanagement of the case, leading to potential complications. Accurate diagnosis in such instances is essential for proper management; otherwise, it can alter the entire treatment strategy and adversely affect the individual's quality of life. The team of specialists (such as radiologists, surgeons and pathologists) responsible for managing these cases should be well-informed about the existence of synchronous neoplasms. Awareness of this coexistence can help prevent the overtreatment of such conditions. If diagnosed correctly using techniques like FNAC, the condition can be managed conservatively with non-surgical approaches, especially in elderly individuals.
Data Availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Authors' Contributions
Study conception and design were done by GS and SaS. SM, ShS and NS contributed to the data collection. Data analysis was performed by VM and RA. The results were interpreted by GS, SaS and VM. All authors were involved in manuscript preparation and editing. All authors approved the final version of the manuscript.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Warnakulasuriya S. Causes of oral cancer–an appraisal of controversies. Br Dent J 2009; 207:471–5. https://doi.org/10.1038/sj.bdj.2009.1009.10.1038/sj.bdj.2009.100919946320 · doi ↗ · pubmed ↗
- 2Slaughter DP Southwick HW Smejkal W. Field cancerization in oral stratified squamous epithelium; clinical implications of multicentric origin. Cancer 1953; 6:963–8. https://doi.org/10.1002/1097-0142(195309)6:53.0.co;2-q.10.1002/1097-0142(195309)6:53.0.co;2-q 13094644 · doi ↗ · pubmed ↗
- 3Panosetti E Luboinski B Mamelle G Richard JM. Multiple synchronous and metachronous cancers of the upper aerodigestive tract: A nine-year study. Laryngoscope 1989; 99: 1267–73. https://doi.org/10.1288/00005537-198912000-00011.10.1288/00005537-198912000-000112601541 · doi ↗ · pubmed ↗
- 4Morris LG Sikora AG Hayes RB Patel SG Ganly I. Anatomic sites at elevated risk of second primary cancer after an index head and neck cancer. Cancer Causes & Control: CCC 2011; 22:671–9. https://doi.org/10.1007/s 10552-011-9739-25.10.1007/s 10552-011-9739-2521327458 PMC 3085084 · doi ↗ · pubmed ↗
- 5León X Quer M Diez S Orús CLópez-Pousa A Burgués J. Second neoplasm in patients with head and neck cancer. Head Neck 1999; 21:204–10. https://doi.org/10.1002/(sici)1097–0347(199905)21:33.0.co;2-7.10.1002/(sici)1097-0347(199905)21:33.0.co;2-710208662 · doi ↗ · pubmed ↗
- 6Sturgis EM Miller RH. Second primary malignancies in the head and neck cancer patient. Ann Otol Rhinol Laryngol 1995; 104:946–54. https://doi.org/10.1177/000348949510401206.10.1177/0003489495104012067492066 · doi ↗ · pubmed ↗
- 7Jones AS Morar P Phillips DE Field JK Husband D Helliwell TR. Second primary tumors in patients with head and neck squamous cell carcinoma. Cancer 1995; 75:1343–53. https://doi.org/10.1002/1097-0142(19950315)75:63.0.co;2-t.10.1002/1097-0142(19950315)75:63.0.co;2-t 7882285 · doi ↗ · pubmed ↗
- 8Gluckman JL Crissman JD. Survival rates in 548 patients with multiple neoplasms of the upper aerodigestive tract. Laryngoscope 1983; 93:71–4. https://doi.org/10.1288/00005537-198301000-00014.10.1288/00005537-198301000-000146823179 · doi ↗ · pubmed ↗