Home‐based collaborative management of bullous pemphigoid with delayed seropositive conversion of anti‐BP180‐NC16a antibody
Hiromitsu Yamashita, Takayuki Ando, Hirohisa Fujikawa, Masayoshi Shiota

TL;DR
An elderly man with bullous pemphigoid was successfully treated at home, with antibody levels changing as the disease progressed.
Contribution
This case demonstrates the feasibility of home-based care for severe bullous pemphigoid and the importance of reevaluating antibody status.
Findings
The patient's anti-BP180-NC16a antibody turned positive as disease severity increased.
Home-based multidisciplinary management was effective for a severe case of bullous pemphigoid.
Delayed seropositive conversion of anti-BP180-NC16a antibody was observed in a bedridden patient.
Abstract
We report the case of an 82‐year‐old male with a history of multiple cerebral infarctions who developed bullous pemphigoid while receiving home‐based care. Anti‐BP180‐NC16a antibody was initially negative, but later became positive as the disease severity worsened. The patient was successfully managed at home through a collaborative effort between a home‐visiting physician (general practitioner), dermatologist, nursing staff, and pharmacists. This case highlights the value of reevaluating anti‐BP180‐NC16a antibody levels and the feasibility of home‐based care for severe bullous pemphigoid in bedridden patients. We present the case of an elderly male with bullous pemphigoid, initially negative for the anti‐BP180‐NC16a antibody, which later became positive as disease activity progressed. The patient was successfully managed at home through multidisciplinary collaboration, including a…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 FIGURE 1
FIGURE 1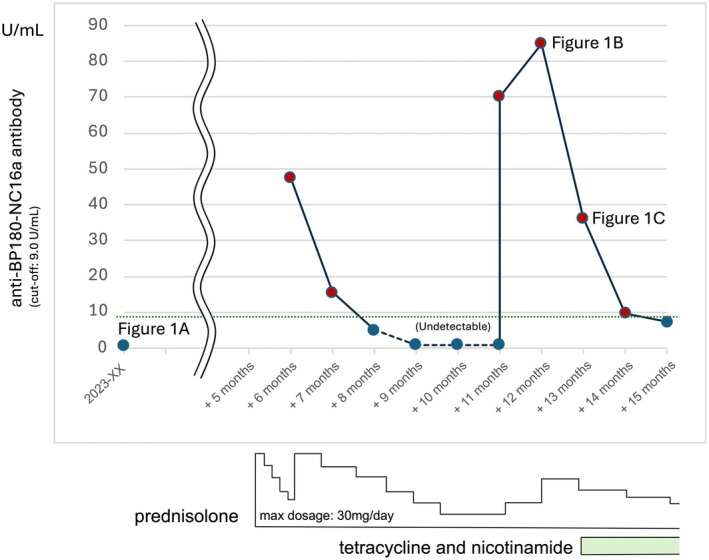 FIGURE 2
FIGURE 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAutoimmune Bullous Skin Diseases · Coagulation, Bradykinin, Polyphosphates, and Angioedema · Urticaria and Related Conditions
BACKGROUND
1
Bullous pemphigoid is an autoimmune disease commonly affecting elderly patients that is characterized by subepidermal blisters caused by autoantibodies against hemidesmosomal constituent proteins (BP180 and BP230).1, 2 This is typically managed by hospitalization and systemic corticosteroid therapy.2 Since false negatives may arise from measuring anti‐BP180‐NC16a antibody levels, with a sensitivity of 72%–89%, a skin biopsy is usually done for diagnosis.1 Although the anti‐BP180‐NC16a antibody reflects disease activity, delayed seropositivity with worsening symptoms has not been reported.3, 4 Herein, we present a case of bullous pemphigoid in a multimorbid, bedridden patient who initially tested negative for anti‐BP180‐NC16a antibody, which later turned positive with increasing disease activity. Despite the severity of the disease, collaborative home‐based care enabled its successful management at home.
CASE PRESENTATION
2
An 82‐year‐old male presented with tense blisters on the posterior neck (largest diameter: 10 mm), first identified by a home‐visiting nurse. The patient had multiple comorbidities, such as heart failure, seizure, and multiple cerebral infarctions, which necessitated a gastrostomy and limited his verbal communication. He required full assistance with activities of daily living (ADLs) and received home‐based medical care. His current medications included edoxaban, vonoprazan, valproic acid, and risperidone.
Upon physical examination, tense blisters were observed on the posterior neck, negative for the Nikolsky sign, suggesting bullous pemphigoid (Figure 1A). However, the patient was negative for anti‐BP180‐NC16a antibody. Given the mild presentation, the home‐visiting physician opted for observation. Five months later, multiple tense blisters and erosion developed across the trunk and limbs, accompanied by erythema and limb edema. As a result of his limitations in ADLs, a hospital outpatient visit was not feasible. Instead, a dermatologist was consulted for a home visit. Drug eruption was initially suspected, leading to the discontinuation of antiepileptics and antipsychotics and the initiation of systemic corticosteroid therapy (prednisolone 30 mg) via the gastrostomy tube. Although the corticosteroid dosage was tapered weekly, the eruption did not resolve adequately, prompting the dermatologist to reconsider the diagnosis. Approximately 1 month after initiating corticosteroid therapy, a repeat test for the anti‐BP180‐NC16a antibody, as recommended by the dermatologist, returned positive (Figure 2). While a skin biopsy is typically performed in a hospital setting, the dermatologist performed the biopsy of a blister from the left lower leg at the patient's home. The histopathological examination revealed subepidermal blisters and lymphocytic infiltration in the upper dermis, confirming the diagnosis of bullous pemphigoid.
Clinical images of the patient's skin lesions. (A) A blister on the posterior neck; (B) Multiple blisters and erosion on the right arm; (C) Healed blisters and erosion on the arm without scarring.
Course of anti‐BP180‐NC16a antibody levels and treatment. The graph illustrates the course of the anti‐BP180‐NC16a antibody levels (U/mL) over time, with corresponding treatment interventions.
Since the patient's family wanted to avoid hospitalization, collaborative home‐based care was provided. The general practitioner managed the potential side effects of the corticosteroid, while the dermatologist adjusted its dosage. Home‐visiting nurses assisted the patient's caregiver with skincare and the application of topical treatments, including diflorasone diacetate (a high‐potency corticosteroid used as adjunctive therapy for moderate‐to‐severe bullous pemphigoid to enhance the effects of systemic corticosteroid therapy) and ozenoxacin lotion (an antibiotic for the suppression of localized bacterial infections). Meanwhile, home‐visiting pharmacists adjusted the forms of medication. Gradually, the erythema, blisters, and erosions subsided, and the anti‐BP180‐NC16a antibody levels decreased (Figure 2). While tapering the corticosteroid, the nurses noted the recurrence of erythema, tense blisters, and erosion on the limbs and trunk. The anti‐BP180‐NC16a antibody levels had risen again, prompting the dermatologist to adjust the corticosteroid dosage. The visiting nurses provided 14 consecutive days of care (except weekends), with each session lasting up to 90 minutes. Disease resolution was seen within 1 month (Figure 1B,C). Currently, the patient has achieved clinical remission, maintained on 10 mg/day of prednisolone, alongside tetracycline and nicotinamide. The anti‐BP180‐NC16a antibody levels became negative again.
DISCUSSION
3
In this case, the initial anti‐BP180‐NC16a antibody test was negative. However, the diagnosis of bullous pemphigoid was supported by the positive antibody levels on repeat testing and skin biopsy. The patient was successfully treated through home‐based care. This case report has two significant implications. First, in home care settings, repeated antibody testing may be considered if the disease severity increases, especially since the initial tests can yield false negatives. Second, bullous pemphigoid can be managed at home through collaborative practice.
No previous reports have discussed NC16A reactivity that developed later in the disease.4 In most patients, NC16A is recognized by the humoral immune system early in the disease, whereas epitope spreading to NC16A rarely occurs in patients without anti‐NC16A IgG.4 Our case suggests that reactivity to NC16A can emerge later, but the mechanism behind this delayed seroconversion remains unknown.3, 4 In a previous study, most patients with bullous pemphigoid who tested negative for anti‐BP180‐NC16a antibodies did not exhibit erythema and had relatively mild phenotypes.3 Therefore, the antibody levels may have lower sensitivity in patients presenting with blisters early in the disease, such as in this case. Thus, the antibody levels should be rechecked in patients who are initially negative but later develop erythema and worsening disease severity, especially when access to dermatologists is limited. Notably, the anti‐BP180 antibody levels correlate with the disease severity of bullous pemphigoid,3 allowing for disease monitoring and corticosteroid dosage adjustments based on antibody titers.
Skin biopsy is often recommended for cases of suspected bullous pemphigoid, but this may be challenging for patients who are unable to visit the hospital. Bullous pemphigoid is associated with neurological diseases such as stroke,5 and older adults, who are more susceptible to this condition, may face significant barriers to hospital care. General practitioners can perform skin biopsies in some countries, but this varies.6, 7 Skin biopsy is not a standard procedure in the Japanese training curriculum for general practice, making it uncommon among these doctors. Thus, interdisciplinary collaboration is crucial between general practitioners and dermatologists, particularly in home‐based care.
This patient was successfully managed at home through multidisciplinary collaboration, despite the typical approach involving hospitalization.2 A key component was the nursing visits lasting 90 minutes per session, which included cleaning the erosions and applying ointment. Japanese medical insurance allows for up to 14 consecutive days of home care visits, with each visit lasting up to 90 minutes under a physician's direction. The nurses also played a crucial role in the early detection and response to deteriorating conditions.8 Additionally, the pharmacist contributed by ensuring the safe adjustment of medications administered via the gastrostomy tube.9 Using their expertise, the pharmacist evaluated whether specific medications were compatible with administration through the tube (e.g., ensuring doxycycline could be dissolved in water). Considering factors such as the patient's family environment and preferences, as well as caregiver‐ or healthcare‐related issues (e.g., limited medical or nursing support),10 it may be feasible to manage severe bullous pemphigoid in a home‐based setting.
CONCLUSION
4
In bullous pemphigoid, the anti‐BP180‐NC16a antibody may exhibit a delayed seropositive conversion as the disease activity progresses. Reassessing antibody levels in cases of worsening disease severity is recommended since this could offer valuable insights for guiding ongoing management.
AUTHOR CONTRIBUTIONS
Hiromitsu Yamashita: Writing – original draft. Takayuki Ando: Writing – review and editing. Hirohisa Fujikawa: Writing – review and editing. Masayoshi Shiota: Supervision; writing – review and editing.
CONFLICT OF INTEREST STATEMENT
The authors declare that there are no conflicts of interest.
ETHICS STATEMENT
Ethics approval statement: Ethics committee approval was not required as this is a single‐patient case report without experimental intervention.
Patient consent statement: Written informed consent was obtained from the patient and his wife for the publication of this case report and any accompanying images.
Clinical trial registration: None.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ujiie H , Iwata H , Yamagami J , Nakama T , Aoyama Y , Ikeda S , et al. Japanese guidelines for the management of pemphigoid (including epidermolysis bullosa acquisita). J Dermatol. 2019;46(12):1102–1135.31646663 10.1111/1346-8138.15111 · doi ↗ · pubmed ↗
- 2Borradori L , Van Beek N , Feliciani C , Tedbirt B , Antiga E , Bergman R , et al. Updated S 2 K guidelines for the management of bullous pemphigoid initiated by the European academy of dermatology and venereology (EADV). J Eur Acad Dermatol Venereol. 2022;36(10):1689–1704.35766904 10.1111/jdv.18220 · doi ↗ · pubmed ↗
- 3Nakama K , Koga H , Ishii N . Clinical and immunological profiles of 14 patients with bullous pemphigoid without Ig G autoantibodies to the BP 180 NC 16A domain. JAMA Dermatol. 2018;154(3):347–350.29299596 10.1001/jamadermatol.2017.5465 PMC 5885813 · doi ↗ · pubmed ↗
- 4Di Zenzo G , Thoma‐Uszynski S , Calabresi V , Fontao L , Hofmann SC , Lacour JP , et al. Demonstration of epitope‐spreading phenomena in bullous pemphigoid: results of a prospective multicenter study. J Invest Dermatol. 2011;131(11):2271–2280.21697892 10.1038/jid.2011.180 · doi ↗ · pubmed ↗
- 5Lai YC , Yew YW , Lambert WC . Bullous pemphigoid and its association with neurological diseases: a systematic review and meta‐analysis. J Eur Acad Dermatol Venereol. 2016;30(12):2007–2015.27599898 10.1111/jdv.13660 · doi ↗ · pubmed ↗
- 6Stevenson P , Rodins K . Skin biopsies [Internet]. Aust J Gen Pract. 2016;74:1–80. Available from: https://www 1.racgp.org.au/ajgp/2018/april/skin‐biopsies 10.31128/AFP-10-17-437629621863 · doi ↗ · pubmed ↗
- 7Newman AR , Heidelbaugh JJ , Klemenhagen K , Michelfelder AJ , Power DV , Hougas JE III . Current procedural practices of family medicine teaching physicians. Fam Med. 2024;56(3):156–162.38241746 10.22454/Fam Med.2024.197714 PMC 11136631 · doi ↗ · pubmed ↗
- 8Mashida Y , Fukahori H , Ikezaki S , Fukui S . Patterns of visiting nurse services for older adults in Japanese residential facilities: a latent class analysis. Geriatr Gerontol Int. 2023;23(5):326–333.36948890 10.1111/ggi.14570 PMC 11503641 · doi ↗ · pubmed ↗