Unique Presentation of Methylenetetrahydrofolate Reductase Mutation With Recurrent Hypercoagulopathy
Hiep Nguyen, Siddanth Singh, Shriya Veluri

TL;DR
A man with a MTHFR mutation experienced severe blood clotting despite treatment, highlighting the challenges of managing this rare condition.
Contribution
This case report provides new insights into managing hypercoagulopathy in patients with heterozygous MTHFR mutations.
Findings
A 37-year-old male with a heterozygous MTHFR mutation had recurrent blood clots despite anticoagulant therapy.
The case highlights the complexity of managing MTHFR-related hypercoagulopathy due to limited clinical guidelines.
This report contributes to understanding clinical manifestations and acute management strategies for MTHFR mutation patients.
Abstract
Methylenetetrahydrofolate reductase (MTHFR) disease is a disorder in which reduced activity of the MTHFR enzyme disrupts folate and homocysteine metabolism, causing elevated homocysteine levels. Patients with MTHFR mutation suffer many serious lifelong complications. Our case presents a 37-year-old male who was diagnosed with a heterozygous subtype of MTHFR. He suffered multiple life-threatening blood clotting episodes despite being on adequate anticoagulants. His management was challenged by the complexity of his disease progression, as well as limited literature and clinical guidelines on the management of this condition. This unique case report adds to the understanding of clinical manifestations and acute management strategies for patients with heterozygous MTHFR mutations who suffer excessive clotting as a complication.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
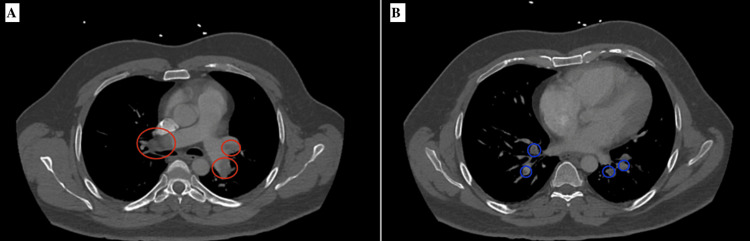 Figure 1
Figure 1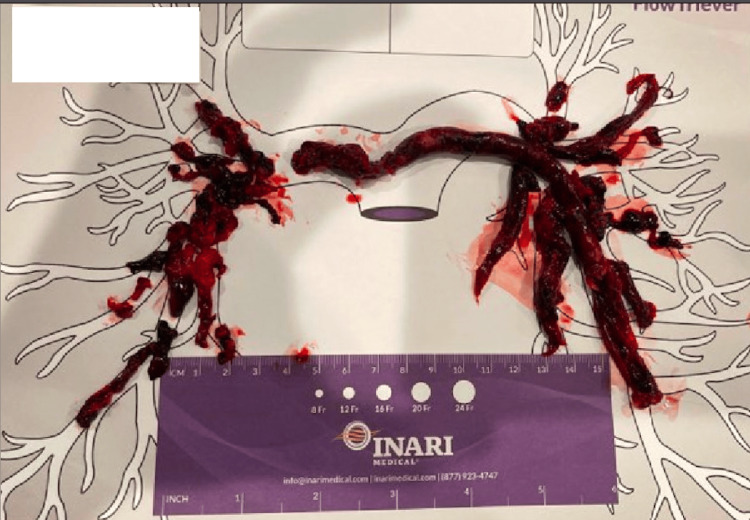 Figure 2
Figure 2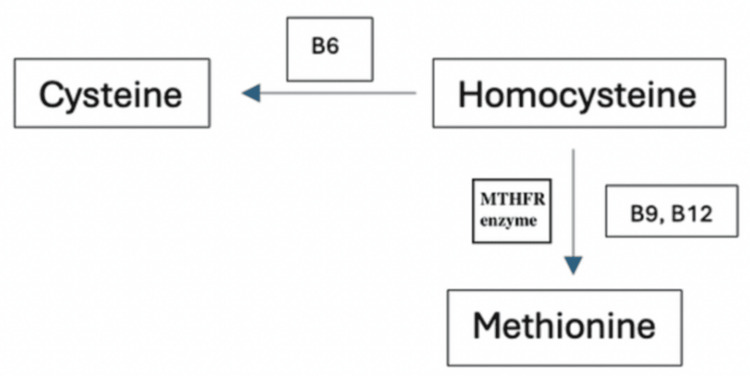 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFolate and B Vitamins Research · Pregnancy and preeclampsia studies · Esophageal and GI Pathology
Introduction
Methylenetetrahydrofolate reductase (MTHFR) disease is a disorder that causes impaired folate and homocysteine metabolism. This is most commonly due to improper transcription of a gene, resulting in reduced enzymatic activity and lower levels of homocysteine. MTHFR is an enzyme responsible for many bodily functions involving vitamin B9, also known as folate. This enzyme converts the inactive form of B9 (folic acid) into the active form of folate and finally 5-methylenetetrahydrofolate (CH3-THF), which is the major form of folate in the human body. CH3-THF, in turn, converts homocysteine to methionine via methionine synthase using vitamin B12 as a cofactor. Improper transcription of the MTHFR gene can lead to various pathologies, including anencephaly, spina bifida, homocystinuria, and other genetic disorders [1]. It has also been shown to increase the risk of specific malignancies, cardiovascular disease, blood clots, and pulmonary embolisms. Here, we present a rare case report of heterozygous MTHFR mutation complicated by recurrent hypercoagulopathy episodes despite appropriate anticoagulation, resulting in a complex hospital course and clinical management.
Case presentation
A 37-year-old Caucasian male with a past medical history of superior mesenteric vein thrombosis currently on apixaban (Eliquis®), deep vein thrombosis, acute lower gastrointestinal (GI) bleeding, anemia, and depression presented to the emergency room with a chief complaint of persistent shortness of breath and right leg pain. The patient stated that walking even a short distance resulted in shortness of breath. Other associated symptoms include dizziness, presyncope episodes, chest tightness, and generalized weakness. The patient denied loss of consciousness, fever, or focal neurological deficits.
In the emergency room, the patient was noted to be afebrile, tachycardic, tachypnic, and saturating 100% on room air, with a body mass index (BMI) of 33. Home medications include apixaban, fluoxetine, hydroxyzine, methocarbamol, pantoprazole, sucralfate, and trazodone. Physical examination showed bilateral leg swelling; the remainder of the exam was unremarkable. Labs were concerning for elevated prothrombin time of 18 seconds (normal: 9.9s-14.9s), high partial thromboplastin time of 42.4 seconds (normal: 25.1s-36.5s), and internationalized normal ratio of 1.5. platelets were also elevated at 510 x 103/µl (normal: 150 x 103/µl - 450 x 103/µl).
Computed tomography angiography (CTA) of the chest during this admission showed repeated massive emboli in the right and left pulmonary arteries, along with scattered thromboembolic burden bilaterally, more pronounced on the right lower lobe pulmonary artery and extending into several segments (Figure 1). Vascular Doppler ultrasound of bilateral lower extremity veins demonstrated thrombosis of the right posterior vein and left popliteal and femoral veins. Further review of the patient's medical record revealed that he was diagnosed with heterozygous MTHFR. Genetic testing was performed at that time and showed a heterozygous mutation of the C677T variant. At the time of his diagnosis, his homocysteine level was in the high normal range at 14 umol/L (normal 0-14) and elevated factor VIII at 315 (50-200).
CT chest showing massive emboli in the right and left pulmonary arteries (Figure 1A, red circles) and scattering emboli in multiple pulmonary arteries (Figure 1B, blue circles).
Prior medical records showed that he was hospitalized 10 days prior for bilateral deep vein thrombosis (DVT) and submassive pulmonary embolism (PE) throughout the entire pulmonary vascular system with right heart strain (Figure 2). He was treated with a thrombectomy and discharged on Eliquis 5 mg twice daily, bridging from heparin. A few days later, the patient was hospitalized again for DVT despite being compliant with anticoagulation and had an inferior vena cava filter placed for pulmonary embolism (PE) prophylaxis.
Extensive emboli clotting the pulmonary arteries removed with thrombectomy.
Cardiology and hematology were consulted for recurrent PE and deep vein thrombosis (DVT). Based on prior outpatient records from his hematologist-oncologist, the patient was negative for protein C or S deficiency, factor V Leiden mutations, the factor II G20210A mutation, antithrombin III levels, antiphospholipid syndrome, malignancy, and disseminated intravascular coagulation. A decision was made to treat the patient with the EkoSonic Endovascular System (EKOS) (Bothell, Washington, United States) catheter infusion of tissue plasminogen activator. The patient reported improving symptoms after the procedure. Repeat CTA chest showed improved PE. He was then placed on a heparin drip as the bridge to warfarin for his long-term coagulation therapy upon discharge once the international normalized ratio (INR) became therapeutic.
Discussion
MTHFR is an uncommon hematologic disease with a vast diversity of complications. There is significant existing literature on the clinical manifestations of homozygous MTHFR mutations, which include hydrocephalus, motor abnormalities, brain atrophy and demyelination, seizures, and motor and other psychiatric conditions [2]. However, very little information has surfaced on the complications and disease course of the heterozygous subtype, leading to difficulty in treating patients like the individual presented in this case. Specifically, his presentation of excessive clotting despite adequate direct oral coagulant highlights the unique manifestation. This case report adds to existing literature by describing a possible clinical presentation and acute clinical management of patients with heterozygous MTHFR mutations, although further research is required to fully understand additional clinical manifestations and long-term disease progression.
MTHFR mutation interrupts the conversion of homocysteine to methionine. The MTHFR enzyme plays an important role in the metabolism of folate, which is an important cofactor for the synthesis of methionine from homocysteine (Figure 3). Elevated homocysteine levels due to an unfunctional MTHFR enzyme result in endothelial dysfunction, which can be linked to cardiovascular disease [3]. The inheritance pattern of this mutation is autosomal recessive, with the most common variants associated with this condition being C677T and A1298C mutations [4]. Studies suggest that 30-40% of the population carries one copy of the mutated gene, given the nature of the autosomal recessive inheritance pattern. This population does not exhibit the phenotypic manifestation, making this disease more difficult to diagnose. The prevalence is not significantly associated with any particular racial or ethnic group.
Homocysteine metabolism pathway. The image is created by the author.
Patients with MTHFR mutation have a significantly increased risk for hypercoagulopathy conditions, such as DVT and PE. It is estimated that homozygous MTHFR variants have a moderate risk for venous thromboembolism (VTE); this risk increases to 50% of cases with compound mutation [5]. Our patient’s factor VIII level was elevated, which could be an effect modifier for his recurrent thrombi formation. Regardless, standard anticoagulation therapy remains the cornerstone of treatment for thromboembolism. Heparin and warfarin, as well as direct oral anticoagulants (DOACs) like rivaroxaban and apixaban, are commonly used. In emergency cases, such as hemodynamic instability, thrombolytic therapy can be used to treat PE [6,7]. Vena cava filters may be inserted in specific situations where anticoagulation is contraindicated or ineffective [8].
As for treating MTHFR, there is very limited data on effective treatment options. One can theorize that there may have been an error for the patient to metabolize his anticoagulation. Treatment failure with apixaban can result from various factors that compromise its efficacy. One significant cause is drug-drug interactions, particularly with medications that affect cytochrome P450 enzymes or P-glycoprotein transporters, which can alter apixaban's plasma concentration. Additionally, patient-specific factors such as renal or hepatic impairment can influence drug metabolism and clearance, leading to subtherapeutic levels. Non-adherence to the prescribed dosing regimen is another critical factor, as missed doses can reduce anticoagulant effects and increase the risk of thromboembolic events. Furthermore, genetic polymorphisms affecting drug-metabolizing enzymes may also contribute to variability in patient response to apixaban [9].
Overall, based on the clinical symptoms and workup as well as the patient’s medical history, a heterozygous MTHFR mutation was determined to be the culprit for increasing this patient's risk of hypercoagulability. He was initially on Eliquis after being treated for his previous DVT and PE; however, this did not prevent additional hypercoagulopathy episodes. Common differential diagnoses to consider alongside MTHFR mutation include factor V Leiden mutation, protein C or S deficiency, antiphospholipid syndrome, or prothrombin deficiency, and other conditions include malignancy, disseminated intravascular coagulation (DIC), obesity, or use of estrogen therapy [10]. Because this patient’s workup was negative for all the above-mentioned conditions, the MTHFR mutation was ultimately established as the underlying cause for the increasing risk of hypercoagulability in this patient.
Conclusions
To the best of our knowledge, this is a unique case presentation that demonstrates a correlation between MTHFR gene mutation and the risk of developing a hyperthrombolic state. Although common risk factors for VTE and PE should be addressed, one should not dismiss the examination for genetic causes, particularly when there is a recurrence. After the likely cause of clotting is identified, further treatment options can be pursued to determine the greatest efficacy. Finally, patient satisfaction and adherence to treatment should improve given an explanation for their signs and symptoms.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Molecular biology of methylenetetrahydrofolate reductase (MTHFR) and overview of mutations/polymorphisms Madame Curie Bioscience Database Leclerc D Sibani S Rozen R Austin Landes Biosciencehttps://www.ncbi.nlm.nih.gov/books/NBK 6561/
- 2Clinical presentation of seven patients with Methylenetetrahydrofolate reductase deficiency Mol Genet Metab Rep Aljassim N Alfadhel M Nashabat M Eyaid W 1006442520203293933910.1016/j.ymgmr.2020.100644 PMC 7479436 · doi ↗ · pubmed ↗
- 3Role of homocysteine in the development of cardiovascular disease Nutr J Ganguly P Alam SF 6142015 https://doi.org/10.1186/1475-2891-14-62557723710.1186/1475-2891-14-6PMC 4326479 · doi ↗ · pubmed ↗
- 4Methylenetetrahydrofolate reductase (MTHFR) C 677T and A 1298 C polymorphisms in breast cancer: a Sardinian preliminary case-control study Int J Med Sci Castiglia P Sanna V Azara A 10891095162019 https://doi.org/10.7150/ijms.321623152317010.7150/ijms.32162 PMC 6743281 · doi ↗ · pubmed ↗
- 5MTHFR A 1298 C and C 677T polymorphisms are associated with increased risk of venous thromboembolism: a retrospective chart review study Acta Haematol Liu F Silva D Malone MV Seetharaman K 20821513820172921206410.1159/000480447 · doi ↗ · pubmed ↗
- 6Deep Vein Thrombosis Waheed SM Kudaravalli P Hotwagner DT Treasure Island (FL)Stat Pearls [Internet]2024 https://www.ncbi.nlm.nih.gov/books/NBK 507708/29939530 · pubmed ↗
- 7A review of the incidence diagnosis and treatment of spontaneous hemorrhage in patients treated with direct oral anticoagulants J Clin Med Gunasekaran K Rajasurya V Devasahayam J 9202010.3390/jcm 9092984 PMC 756383732942757 · doi ↗ · pubmed ↗
- 8Inferior vena cava filters: guidelines, best practice, and expanding indications Semin Intervent Radiol De Young E Minocha J 65703320162724747210.1055/s-0036-1581088 PMC 4862857 · doi ↗ · pubmed ↗