Analysis of risk factors associated with Lymph Node Metastasis and Recurrence Post Thyroid Carcinoma Surgery
Shengchao Wang, Zhongxu Bai, Huijuan Yan, Chunmei Yan, Junhui Wang

TL;DR
This study identifies key risk factors for lymph node metastasis and recurrence after thyroid cancer surgery, which could help improve patient outcomes.
Contribution
The study identifies specific independent risk factors for lymph node metastasis and recurrence in thyroid carcinoma patients post-surgery.
Findings
27% of patients experienced lymph node metastasis or recurrence after thyroid carcinoma surgery.
Univariate analysis identified nine factors influencing metastasis and recurrence (P<0.05).
Logistic regression confirmed five independent risk factors: gender, age, hyperthyroidism history, tumor classification/stage, and lesion laterality.
Abstract
To investigate the risk factors associated with postoperative lymph node metastasis and recurrence in patients with thyroid carcinoma. Retrospective analysis of clinical data of one hundred patients with thyroid carcinoma who underwent first surgery at the Yellow River Sanmenxia Hospital from June 2019 to July 2023. Record postoperative lymph node metastasis, recurrence, and disease-free survival time. Kaplan Meier survival analysis was used to evaluate the recurrence free survival rate after surgery. Compared the differences between groups with and without lymph node metastasis. Analysis of risk factors for postoperative lymph node metastasis and recurrence in patients with thyroid carcinoma. In study, 27 out of 100 patients experienced lymph node metastasis and recurrence, with an overall recurrence rate of 27.00%. There were nine cases of intrathyroid recurrence, 15 cases of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
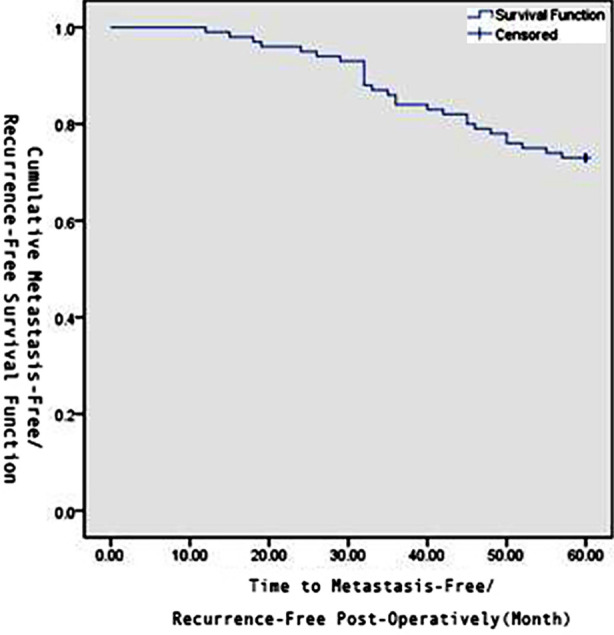 Fig.1
Fig.1| Variable | Recurrence/ Metastasis Group | Non-Recurrence/ Metastasis Group | χ2 | P |
|---|---|---|---|---|
| Gender | 5.233 | 0.022 | ||
| Male | 3 (11.11) | 25 (34.25) | ||
| Female | 24 (88.89) | 48 (65.75) | ||
| Age (years) | 4.619 | 0.032 | ||
| ≥45 | 18 (66.67) | 31 (42.47) | ||
| <45 | 9 (33.33) | 42 (57.53) | ||
| Body Mass Index (kg/m2) | 0.457 | 0.499 | ||
| ≥24 | 15 (55.56) | 35 (47.95) | ||
| <24 | 12 (44.44) | 38 (52.05) | ||
| History of hyperthyroidism | 4.822 | 0.028 | ||
| Yes | 17 (62.96) | 28 (38.36) | ||
| No | 10 (37.04) | 45 (61.64) | ||
| Tumor Type | 8.280 | 0.041 | ||
| Medullary carcinoma | 9 (33.33) | 10 (13.70) | ||
| Papillary carcinoma | 14 (51.86) | 55 (75.34) | ||
| Follicular carcinoma | 3 (11.11) | 8 (10.96) | ||
| Undifferentiated carcinoma | 1 (3.70) | 0 (0.00) | ||
| Tumor stage | 12.412 | 0.004 | ||
| Stage I | 4 (14.81) | 29 (39.73) | ||
| Stage II | 4 (14.81) | 22 (30.14) | ||
| Stage III | 12 (44.45) | 15 (20.54) | ||
| Stage IV | 7 (25.93) | 7 (9.59) | ||
| Tumor diameter (cm) | 3.989 | 0.046 | ||
| ≥2 | 16 (59.26) | 27 (36.99) | ||
| <2 | 11 (40.74) | 46 (63.01) | ||
| Number of cancer foci | 8.126 | 0.004 | ||
| Single | 10 (37.04) | 50 (68.49) | ||
| Multiple | 17 (62.96) | 23 (31.51) | ||
| Unilateral or bilateral lesions | 4.261 | 0.039 | ||
| Unilateral | 12 (44.44) | 49 (67.12) | ||
| Bilateral | 15 (55.56) | 24 (32.88) | ||
| 131I treatment | 5.463 | 0.019 | ||
| Yes | 15 (55.56) | 22 (30.14) | ||
| No | 12 (44.44) | 51 (69.86) | ||
| Surgical method | 5.716 | 0.017 | ||
| Total thyroidectomy | 11 (40.74) | 49 (67.12) | ||
| Subtotal thyroidectomy | 16 (59.26) | 24 (32.88) |
| Factor | Regression Coefficient | Standard Error | Wald c2 | P | OR | 95%CI |
|---|---|---|---|---|---|---|
| Gender | -8.551 | 2.929 | 8.523 | 0.004 | 0.000 | 6.209E-7-0.060 |
| Age | 3.967 | 1.569 | 6.397 | 0.011 | 52.851 | 2.443-1143.535 |
| History of hyperthyroidism | 3.109 | 1.325 | 5.507 | 0.019 | 22.397 | 1.669-300.524 |
| Tumor type | -12.264 | 2.866 | 18.313 | 0.000 | 4.719E-6 | 1.716E-8-0.001 |
| Tumor stage | -4.337 | 1.876 | 5.344 | 0.021 | 0.013 | 0.000-0.517 |
| Unilateral or bilateral lesions | -2.729 | 1.358 | 4.036 | 0.045 | 0.0065 | 10.005-0.935 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsThyroid Cancer Diagnosis and Treatment
INTRODUCTION
Thyroid carcinoma, a prevalent endocrine and malignant thyroid tumor in clinical settings, has seen an increasing incidence rate over the years1, particularly among women. In developed regions such as China, Japan, and South Korea, the incidence of thyroid carcinoma has multiplied in recent decades.2 In 2012, China accounted for 15.6% of the world’s new thyroid carcinoma cases and 13.8% of deaths.3 The incidence rate of thyroid carcinoma in China in 2016 was 10.58 per 100,000, with a male-to-female ratio of 1:3.2, placing thyroid carcinoma as the third most common cancer among women.4 Data indicated that the 20-years survival rate for thyroid carcinoma patients in the United States reached 97%, the five-years survival rate in Europe was 86.5%, while the five-years survival rate in China was 84.3%, showing a disparity with developed countries.5
The etiology of thyroid carcinoma remains unclear. Although it can occur at any age, it predominantly affects young and middle-aged adults. Once diagnosed, aggressive surgical resection is the primary treatment method, yet the risk of metastasis and recurrence post-surgery persists. Patients and their families are deeply concerned about surgical outcomes, postoperative prognosis, and survival. Unfavorable surgical results or postoperative metastasis/recurrence can cause significant distress to patients and their families. Studies have verified that gender, age, and thyroid nodules are risk factors for thyroid carcinoma6, yet the factors influencing lymph node metastasis and recurrence post-surgery remain controversial. Some research indicates that male gender, age, tumor size, and lymph node metastasis are independent risk factors for postoperative recurrence of thyroid carcinoma7, while other studies suggest gender is not a risk factor.8 Current knowledge on the factors affecting cervical lymph node metastasis and postoperative recurrence of thyroid carcinoma primarily comes from international studies, with limited domestic research. Hence, this study’s primary goal is to clarify the factors influencing cervical lymph node metastasis and postoperative recurrence of thyroid carcinoma in the Chinese population, which holds significant importance for guiding the treatment of thyroid carcinoma in China.
METHODS
A retrospective analysis was conducted on the clinical data of one hundred patients diagnosed with thyroid carcinoma and undergoing initial surgery at Yellow River Sanmenxia Hospital from June 2018 to July 2023. Lymph node metastasis was confirmed by routine pathology or clinical diagnosis of distant bone or lung metastasis. Recurrence was confirmed by biopsy or pathological examination of the reappearing tumor site. Patient information was collected from the hospital’s medical record system, including gender, age, history of hyperthyroidism, tumor classification, tumor staging, tumor diameter, number of cancer foci, unilateral or bilateral lesions, surgical methods, and ^131^I treatment. Patients were followed up for five-years through outpatient reexaminations, WeChat, or telephone contact.
A total of one hundred thyroid cancer patients were screened from June 2018 to June 2023 according to inclusion and exclusion criteria, including 28 males and 72 females, aged 32-78 years. Among them, there were 88 cases of papillary carcinoma, six cases of follicular carcinoma, four cases of medullary carcinoma, and two cases of undifferentiated carcinoma. During the follow-up period, 27 cases experienced recurrence and metastasis, while 73 cases did not. Specifically, there were nine cases of intrathyroidal recurrence, 15 cases of cervical lymph node metastasis, two cases of intrathyroidal recurrence with cervical lymph node metastasis, and one case of distant metastasis (lung metastasis). From the date of surgery to the end of follow-up on July 30, 2023, the follow-up period ranged from one to 60 months, during which 27 patients(27.00%) experienced recurrence.
Ethics Approval:
The study was approved by the Institutional Ethics Committee of Yellow River Sanmenxia Hospital (No.: 2021-0901; date: September 01,2021), and written informed consent was obtained from all participants.
Inclusion criteria:
- Patients who underwent initial thyroidectomy and were diagnosed with thyroid carcinoma at our hospital from June 2018 to July 2023.
- Complete clinical data available to determine whether the patient had metastasis and recurrence.
- Effective control of metastasis after treatment if it occurred.
Exclusion criteria:
- Patients with other malignant tumors.
- Patients with severe heart, lung, or kidney dysfunction.
Observation and evaluation indicators:
During the follow-up period, lymph node metastasis and recurrence were recorded. Based on relevant literature, this study selected factors such as gender, age, body mass index, history of hyperthyroidism, tumor classification, tumor staging, tumor diameter, number of cancer foci, unilateral or bilateral lesions, surgical methods, and ^131^I treatment to analyze the influencing factors of cervical lymph node metastasis and postoperative recurrence of thyroid carcinoma.
Statistical analysis:
All data were statistically analyzed using the SPSS 21.0 software (SPSS Inc., Chicago, IL, USA). Measurement data were expressed as mean ± standard deviation (X¯±S), and t-tests were used for comparisons between groups. Enumeration data were expressed as numbers and percentages[n (%)], and comparisons between groups were made using χ2 test or Fisher’s exact probability method. Logistic regression analysis was used to identify influencing factors. P-value <0.05 was considered a statistically significant difference.
RESULTS
The Kaplan-Meier method was used to derive the one year, three years, and five years recurrence-free survival curves for thyroid cancer patients postoperatively, as shown in Fig.1. Univariate analysis was conducted on various factors that might influence lymph node metastasis and postoperative recurrence in thyroid cancer patients. The results showed that gender, age, history of hyperthyroidism, tumor type, tumor stage, tumor diameter, number of cancer foci, unilateral or bilateral lesions, ^131^I treatment, and surgical method were all influencing factors for lymph node metastasis and postoperative recurrence in thyroid cancer patients(P<0.05), Table-I. Based on the results of univariate analysis, gender, age, history of hyperthyroidism, tumor type, tumor stage, tumor diameter, number of cancer foci, unilateral or bilateral lesions, ^131^I treatment, and surgical method were identified as risk factors for lymph node metastasis and postoperative recurrence in thyroid carcinoma patients. To exclude the mutual influence of these risk factors and further identify independent risk factors, the above 11 risk factors were included in the Logistic regression model for multivariate analysis. The results showed that gender, age, history of hyperthyroidism, tumor type, tumor stage, and unilateral or bilateral lesions were independent risk factors for lymph node metastasis and postoperative recurrence in thyroid carcinoma patients (P<0.05), Table-II.
Cumulative Recurrence-Free Survival Function Post Thyroid Carcinoma Surgery.
DISCUSSION
In this study, the postoperative cervical lymph node metastasis and recurrence in female patients was significantly higher than in male patients, making it an independent risk factor for postoperative cervical lymph node metastasis and recurrence(P<0.05). Based on the literature, we believe that this phenomenon is related to the presence of estrogen receptor genes in thyroid carcinoma, which exhibit polymorphism. The expression level of estrogen receptor genes in females is higher than in males, which may explain the gender differences in the incidence of thyroid carcinoma. This also suggests that hormonal and reproductive factors are risk factors for postoperative cervical lymph node metastasis and recurrence in females. However, some studies have shown that the recurrence rate in males is higher than in females9,10, while other studies have shown that gender differences are not related to cervical lymph node metastasis and recurrence after thyroidectomy.11
The results of this study indicated that the postoperative cervical lymph node metastasis and recurrence rate in patients aged ≥4 five-years is significantly higher than in those aged <4 five-years (P<0.05), making it an independent risk factor for postoperative cervical lymph node metastasis and recurrence (P<0.05). Currently, there is still controversy regarding the age cutoff for TNM staging of thyroid carcinoma. Some studies suggest that age is an important factor influencing the prognosis of thyroid carcinoma within the age range of 25-5 five years, regardless of the age used as the grouping cutoff.12 Other studies have shown13 that the age at first diagnosis is a factor influencing cervical lymph node metastasis and recurrence after thyroidectomy, with ≥4 five-years being a risk factor for postoperative cervical lymph node metastasis and recurrence. However, some studies have shown that age is not related to cervical lymph node metastasis and recurrence after thyroidectomy.14
Studies have shown that some patients with hyperthyroidism may develop thyroid carcinoma.15 The relationship between hyperthyroidism and thyroid carcinoma remains controversial, and its pathogenesis is still unclear. Current research suggests that hyperthyroidism may influence the occurrence of thyroid carcinoma. This is because long-term excessive use of antithyroid drugs in hyperthyroid patients can lead to elevated thyroid-stimulating hormone (TSH) levels, which is a promoting factor for the development of thyroid carcinoma.16 Our study results indicate that among 27 patients with postoperative metastasis/recurrence of thyroid carcinoma, 17 had a history of hyperthyroidism. Both univariate and multivariate analyses showed that hyperthyroidism was statistically significant (P<0.05) as a risk factor for postoperative metastasis/recurrence of thyroid carcinoma.
Therefore, for patients with thyroid carcinoma combined with hyperthyroidism, reasonable postoperative treatment, regular check-ups, and follow-ups are necessary to prevent postoperative metastasis/recurrence of thyroid carcinoma. Staging and classification of thyroid carcinoma play a significant role in predicting postoperative prognosis, metastasis, and recurrence in thyroid carcinoma patients. Previous studies have confirmed17 that the later the TNM stage, the higher the rate of postoperative metastasis/recurrence. Our study results show that among the 27 patients with metastasis/recurrence, 12 were in Stage-III and seven in Stage-IV. Univariate and multivariate analyses indicated that the TNM stage of thyroid tumors was statistically significant (P<0.05) as an independent risk factor for postoperative metastasis/recurrence, consistent with previous research findings.18 The pathological type of thyroid carcinoma not only guides treatment but also predicts patient prognosis. Studies have shown that different pathological types of thyroid carcinoma have varying impacts on prognosis.19 High-grade thyroid carcinomas (such as medullary carcinoma and anaplastic carcinoma) are associated with a significantly increased risk of postoperative metastasis/recurrence due to their higher invasiveness and metastatic potential. Our study’s univariate and multivariate analyses revealed that the pathological type of thyroid carcinoma was statistically significant (P<0.05) as an independent risk factor for postoperative metastasis/recurrence, consistent with previous studies.20
Additionally, whether the tumor is unilateral or bilateral is also an important factor in predicting postoperative metastasis/recurrence of thyroid carcinoma. Studies have found^21^ that the presence of bilateral primary tumors is associated with an increased risk of postoperative metastasis/recurrence. This may be due to the greater extent of tumor spread and lymph node involvement in bilateral lesions compared to unilateral lesions, as well as differences in treatment approaches, which directly affect treatment outcomes and prognosis. Our study’s univariate and multivariate analyses showed that unilateral or bilateral lesions were statistically significant (P<0.05) as independent risk factors for postoperative metastasis/recurrence of thyroid carcinoma.
Limitations:
It includes a small number of observed cases and limited follow-up factors. Future studies should expand the sample size and increase follow-up factors to further analyze the factors influencing postoperative metastasis/recurrence of thyroid carcinoma.
CONCLUSIONS
Postoperative metastasis/recurrence of thyroid carcinoma is a critical issue that needs attention in the treatment of thyroid carcinoma. Factors such as gender, age, history of hyperthyroidism, tumor classification, tumor staging, and unilateral or bilateral lesions are major risk factors associated with postoperative metastasis/recurrence of thyroid carcinoma. In-depth research and understanding of these factors are crucial for improving the treatment outcomes and prognosis of thyroid carcinoma.
Authors’ Contributions:
SW: Carried out the studies, participated in collecting data, and drafted the manuscript, and is responsible and accountable for the accuracy or integrity of the work.
ZB, HY, CY and JW: Study design**,** Performed the statistical analysis and critical review.
All authors have read and approved the final manuscript.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Wang LL Li HQ Chang QG Li S Yin DT Clinical pathology and incidence trend of thyroid cancer based on 21980 cases Zhonghua Yi Xue Za Zhi 20201001410721076 doi:10.3760/cma.j.cn 112137-20190905-019723229486910.3760/cma.j.cn 112137-20190905-01972 · doi ↗ · pubmed ↗
- 2Siano M Alfieri S Granata R Calareso G Orlandi E Bergamini C Locati LD The dilemma of metastatic medullary thyroid carcinoma:when to start systemic treatment Tumori 20191056 NP 28NP 31doi:10.1177/03008916198295713078210310.1177/0300891619829571 · doi ↗ · pubmed ↗
- 3Amin SN Shinn JR Naguib MM Netterville JL Rohde SL Risk Factors and Outcomes of Postoperative Recurrent Well-Differentiated Thyroid Cancer:A Single Institution's 1five-years'Experience Otolaryngol Head Neck Surg 20201624469475 doi:10.1177/01945998209049233206918410.1177/0194599820904923 · doi ↗ · pubmed ↗
- 4Shah AA Jain PP Dubey AS Panjwani GN Shah HAA study of clinicopathological characteristics of thyroid carcinoma at a Tertiary Care Center J Cancer Res Ther 2018142357360 doi:10.4103/0973-1482.1806112951691910.4103/0973-1482.180611 · doi ↗ · pubmed ↗
- 5Liu J Liu X Guo Z Lv X Mao W Xu D Ultrasound-guided fine needle aspiration cytology of Para-aortic lymph node metastasis in uterine cervical cancer:diagnostic accuracy and impact on clinical decision making BMC Cancer 2021211964 doi:10.1186/s 12885-021-08492-23445260910.1186/s 12885-021-08492-2PMC 8393715 · doi ↗ · pubmed ↗
- 6Lim ST Jeon YW Gwak H Suh YJ Incidence, Risk Factors, and Clinical Implications of Delayed Hypoparathyroidism on Postoperative Day two Following Total Thyroidectomy for Papillary Thyroid Carcinoma Endocr Pract 2020267768776 doi:10.4158/EP-2019-05443347164610.4158/EP-2019-0544 · doi ↗ · pubmed ↗
- 7De Jong MC Gaze MN Szychot E Rozalén García V Brain C Dattani M Treating papillary and follicular thyroid cancer in children and young people:Single UK-center experience between, 2003 and 2018 J Pediatr Surg 2021563534539 doi:10.1016/j.jpedsurg.2020.07.0343283897510.1016/j.jpedsurg.2020.07.034 · doi ↗ · pubmed ↗
- 8Luo J Li H Deziel NC Huang H Zhao N Ma S Genetic susceptibility may modify the association between cell phone use and thyroid cancer:A population-based case-control study in Connecticut Environ Res 2020182109013 doi:10.1016/j.envres.2019.1090133191831010.1016/j.envres.2019.109013 PMC 7061309 · doi ↗ · pubmed ↗