Towards individualised treatment of urinary tract infections
Ellen V. Stadler, Alison Holmes, Danny O’Hare, Timothy M. Rawson

TL;DR
This paper suggests using urine biomarkers and drug levels to personalize antibiotic treatment for urinary tract infections.
Contribution
The novel idea is using existing technologies to monitor biomarkers and drug levels for individualized antibiotic dosing.
Findings
Longitudinal monitoring of urinary biomarkers can support personalized antimicrobial therapy.
Linking biomarkers with drug levels enables real-time pharmacokinetic-pharmacodynamic optimization.
Existing technologies can be used for individualized PK-PD optimization in UTIs.
Abstract
Monitoring host- and pathogen-specific biomarkers alongside drug levels at the site of infection offers promise for personalised antimicrobial therapy. Here, we highlight the potential of longitudinally monitoring biomarkers in urine using existing technologies to enable individualised PK-PD optimisation in urinary tract infections. Stadler et al. propose using existing technologies to link urinary biomarkers and antimicrobial drug levels for personalised treatment of urinary tract infections. This approach aims to enable real-time pharmacokinetic-pharmacodynamic monitoring and optimise individual antibiotic dosing.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
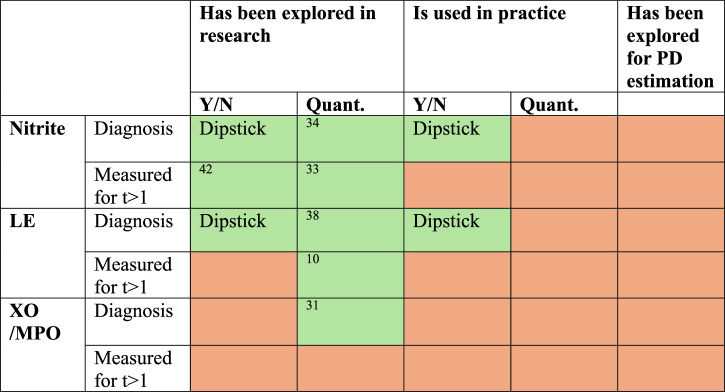 Figure 1
Figure 1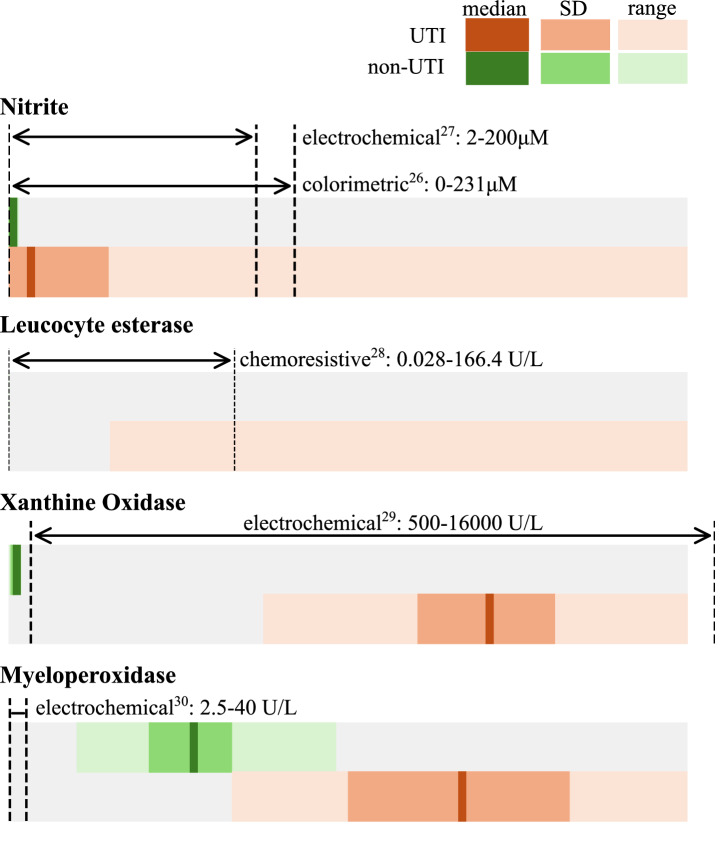 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsUrinary Tract Infections Management · Antibiotics Pharmacokinetics and Efficacy · Bacterial Identification and Susceptibility Testing
Introduction
Antimicrobial drugs are used to treat bacterial infections and have revolutionised modern medicine. However, the inappropriate use and dosage of antimicrobials increases the risk of treatment failure, toxicity to the patient, and the development of drug resistance, rendering antimicrobials ineffective and putting medicine and global health at risk^1^. Bacterial urinary tract infection (UTI) affects 150 million people globally each year. On average, one in two adult women will experience a UTI during their lifetime^2^. Treating UTIs with empirical antibiotics when patients report symptoms results in overuse of antimicrobials, as more than half of the gold standard urine culture results of symptomatic females do not confirm a UTI^3^. Developing novel antimicrobials, enhancing diagnostic precision, and optimising the use of current treatments are approaches that can be used to mitigate the impact of drug resistance and maintain access to effective antimicrobial drugs^1^.
Both bacteria-specific and immune response biomarkers directly measured from the urine are frequently used to diagnose UTI, as the direct quantification of bacterial load in urine through culture is slow^4^. Their diagnostic value has been extensively explored, specifically compared to the gold standard culture and count. It is generally agreed that conventional biomarkers tested with urinary dipstick tests, such as nitrite and leucocyte esterase, have limited accuracy in the diagnosis of UTIs^5–7^. Only a few of these biomarkers have been explored longitudinally in the literature, such as neutrophil gelatinase-associated lipocalin or leucocyte esterase^8–10^. Similar to the diagnosis of UTIs through biomarker detection, the need for rapid susceptibility testing has also been addressed in the literature^11^. In vitro models mimic the urinary environment to understand the action and find the optimal dose of antimicrobial drugs^12^. But pharmacokinetic optimisation has not been explored in-vivo. Real-time monitoring of known biomarkers used for UTI diagnosis alongside drug concentration in urine has not yet been explored and could enable real-time estimation of treatment success.
In this Comment, we aim to present the unexplored potential of using current and emerging technologies to monitor biomarkers alongside urinary antimicrobial drug concentration in UTI to gain an understanding of the relationship between drug exposure linked with host and pathogen response. We argue this could be used towards real-time pharmacokinetic-pharmacodynamic (PK-PD) monitoring and support truly individualized approaches to the antimicrobial treatment of UTI.
Challenges and opportunities in individualised antimicrobial dosing for urinary tract infections
There are significant variations in how antimicrobials are absorbed, distributed, metabolised, and excreted between patients (pharmacokinetics; PK). Additionally, the effect of an antimicrobial may vary based on organism and patient factors (pharmacodynamics; PD). Therapeutic drug monitoring (TDM) is a method of measuring drug concentration to achieve predefined PK-PD targets associated with clinical efficacy and to minimise the development of toxicity^13^. PD values, such as minimum inhibitory concentration (MIC), are assessed in-vitro or estimated using infection biomarkers such as C-reactive protein^14^. Delivery of individualised antimicrobial dosing through TDM is recommended in critical care settings for beta-lactam, glycopeptide, aminoglycoside, and oxazolidinone antibiotic classes^15^.
Individualised antimicrobial dosing using current TDM approaches can be challenging. Randomised clinical trials have shown no significant difference in mortality and microbiological cure rate between critically ill patients who undergo TDM and those who do not^16,17^. Important limitations of current approaches to TDM include the reliance on daily blood measurements of drug concentration and reliance on in-vitro PD values, such as MIC, that may not reflect drug concentration or antimicrobial PD at site of infection. To address these limitations, we need to consider technology for near real-time monitoring of individual PK-PD that can be performed closer to the site of infection and enable delivery of real-time dose adjustment.
UTI biomarkers are used for diagnosis, and the potential to use the temporal change of these biomarkers to monitor response to treatment in UTI has been discussed^18^ but not widely explored. TDM in urine has been reported to support dose optimisation in other infectious diagnoses, but not specifically for UTI management^19^.
Supporting individualised dosing by quantifying host-bacteria-drug interactions
Adjusting antimicrobial dosing to improve PK-PD target attainment, using indices such as C_max_ to MIC ratio, results in improved treatment outcomes for patients with UTI^12^. Current PK-PD targets are based on population PK in serum and in-vitro MIC values. They do not consider variations in host factors such as immune response, site of infection, or local changes in pH, which affect both the infectious organism and the drug. For example, nitrofurantoin, a common first line treatment for UTI, demonstrates significantly increased bactericidal activity against common urinary pathogens at lower pH levels^20^. In-vivo PD estimation in urine has limited evidence of applicability to traditional antimicrobial susceptibility testing that is commonly used to guide antimicrobial selection^12^.
TDM has been used to optimise dosing in UTI by measuring drug concentrations in blood^21^, even though drug levels of antimicrobials in urine are typically considerably higher than in serum^22^. For example, amoxicillin, a beta-lactam antibiotic, has been demonstrated to achieve significantly greater peak urinary concentrations following standard dosing compared to serum. Local urinary concentration will often exceed traditional MIC breakpoints used for antimicrobial susceptibility reporting and may explain observed treatment success in the face of isolates that are reported as resistant^23^
The idea of connecting infection-specific biomarkers to antimicrobial PK to evaluate drug PD is well described. Galactomannan levels have been used to describe voriconazole PD in invasive aspergillosis in children^24^. Urinary biomarkers are frequently used to diagnose UTI, and the quantitative time-course of biomarkers, for example urinary leukocytes, has been shown to predict treatment outcome^10^.
We propose that the origin of well-described UTI biomarkers currently reported is either bacteria- or host-response-specific. Bacteria- and host-response biomarkers measured in urine could facilitate PD estimates for UTI if linked to observed drug exposure during treatment. This renders urine a promising area for the development of simple, non-invasive, longitudinal methods of monitoring and optimising antimicrobial PK-PD in real-time.
The unexplored potential of longitudinal monitoring of drug exposure, host-response, and infection biomarkers in urine
Dipstick tests are frequently used to detect biomarkers qualitatively to support UTI diagnosis^25^. Below, we categorise biomarkers frequently used in dipstick tests, and recently described as promising for UTI diagnosis, into host-response and bacteria-specific biomarkers. The detected ranges of these biomarkers are shown in Table 1.Table 1. Biomarker levels in non UTI and UTI patientsNon-UTIUTIMeanSDRangeMeanSDRangeNitrite^34^ [µM]0.890.860.11–7.815.2650.21–548LE^38^ [U/L]N/AN/AN/AN/AN/A75–500XO^31^ [U/L]104.5749.2817–27110,820.21543.75780–15,370MPO^31^ [U/L]414.0993.31156–7451025.8251.3510–1546Reported ranges of commonly used biomarkers for UTI diagnosis.LE Leucocyte esterase, XO Xanthine Oxidase, MPO Myeloperoxidase.
Despite the development of quantitative point-of-care technologies for nitrite^18,26,27^, leucocyte esterase^28^ (LE), xanthine oxidase (XO)^29^ and myeloperoxidase (MPO)^30^ in urine, these biomarkers are frequently reported in a yes or no fashion. The sensitivity and specificity of XO and MPO for diagnosing UTIs show promising diagnostic values (100% and 87% sensitivity for XO and MPO, 100% specificity for both)^31^. Sensitivity and specificity of a positive nitrite and LE test vary depending on UTI prevalence and the bacterial count threshold used to define a UTI. Sensitivities in different studies range from 36–57% for nitrite and 72–95% for LE, and specificities 78–98% for nitrite and 9–59% for LE^32^.
Few studies have evaluated biomarker concentration at more than one time point during UTI^10,33^, and the possibility of using quantitative measurements serially to estimate PD remains unexplored (Fig. 1). Longitudinal, quantitative monitoring of biomarkers in UTI using point-of-care technologies, alongside drug measurement, could facilitate novel approaches to real-time PK-PD monitoring and individualised antimicrobial dosing (Fig. 2).Fig. 1. Overview of how UTI biomarkers are used in research and practice.UTI biomarkers are used for identification of UTIs, but their use for PD estimation is unexplored. Green: data available. Red: no data available. Y/N Qualitative, yes or no outcome, Quant Quantitative, LE Leucocyte esterase, XO Xanthine Oxidase, MPO Myeloperoxidase.Fig. 2. Detection range of point-of-care technologies and expected biomarker levels.Quantitative point-of-care sensors with detection range suitable to distinguish between UTI and non-UTI patients exist for Nitrite, Xanthine Oxidase and Myeloperoxidase. Length of bars corresponds to the range of values in Table 1. SD Standard deviation.
Nitrite measurement is related to bacterial activity and is therefore a bacteria-specific biomarker. Maximum reported nitrite levels in UTI patients are 548 µM, and 7.8 µM in non-UTI patients^34^. Enterobacteriaceae, including Escherichia coli, which is responsible for most UTIs, use dietary nitrate as a secondary electron acceptor in oxygen-depleted urine and convert it to nitrite^35^. Limitations for nitrites use as an indicator of UTI include that nitrate to nitrite conversion can take up to 30 h to reach saturation, and not all bacteria that cause UTIs, such as Enterococcus species and Staphylococcus saprophyticus, exhibit nitrate-reducing activity^36^. Nitrite production over time in in-vitro broth culture of Escherichia coli and other bacteria has been explored^35^, but has not been assessed in patient samples.
Leucocyte esterase is an enzyme produced by neutrophils recruited during infection and is used as an indicator of urinary tract inflammation^37^. Leucocyte esterase can potentially indicate host response during UTI. The diagnostic value of nitrite and leucocyte varies between studies, which is believed to be due to different patient populations with varying pretest probabilities of a UTI^25^. Precise, sequential leucocyte esterase levels during antibiotic therapy in UTI can be used to predict antimicrobial outcome^10^, and should be explored in combination with bacteria-specific biomarkers such as nitrite. LE levels in UTI patients are reported up to 500 U/L^38^.
Xanthine Oxidase (XO) and Myeloperoxidase (MPO**)** have recently attracted attention as biomarkers exhibiting promising diagnostic properties for UTI^31^. XO is an enzyme responsible for the conversion of hypoxanthine to xanthine and uric acid. The origin of elevated XO during UTI is unclear but is likely a host-specific inflammation marker with mean levels of 10,820 U/L in UTI patients compared to 105 U/L in the urine of patients without UTI^39^. MPO is a host-specific biomarker with mean level of 1026 U/L observed in UTI samples compared to 414 U/L in non-UTI samples^31^.
Concluding remarks
Sensitive, rapid, and inexpensive quantitative sensing technologies are needed for real-time PK-PD monitoring and dose adjustments. Various methods to detect nitrite quantitatively have been developed and tested in human urine, such as adaptation of the colorimetric Griess test for quantitative read-out^18,26^ or electrochemical detection^27^.
Whilst studies looking at detecting MPO and XO are sparse, as they are recently identified markers of UTI, proof-of-concept of their electrochemical detection in a point-of-care fashion to diagnose UTI exist^29,30^.
In the literature, the application of developed technologies to monitor UTI biomarkers longitudinally is discussed, but has not been directly explored. Table 1 summarises the observed range of organism and host-specific biomarkers in individuals with and without UTI. For nitrite, LE and XO, point-of-care technologies exist to quantitatively detect their concentration in the range of interest (Fig. 2). The electrochemical detection of MPO shows a narrow detection range (2.5–400 U/L)^40^, and the expansion of this range to monitor UTIs has not been discussed (Fig. 2). Drug concentration monitoring in UTI has been explored, but interestingly drug levels were assessed in serum and not in urine^21^.
To achieve truly individualised approaches to antimicrobial treatment of UTI, research must focus on evaluating longitudinal drug exposure and host- and organism-specific biomarkers measured in urine. Demonstrating the utility of longitudinal monitoring and linking drug exposure and host- and organism specific biomarkers to treatment outcome will support the development of point-of-care technologies for real-time antimicrobial optimisation for patients with UTI.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Rawson, T. M. et al. Optimizing antimicrobial use: challenges, advances and opportunities. Nat. Rev. Microbiol.19, 747–758 (2021).10.1038/s 41579-021-00578-934158654 · doi ↗ · pubmed ↗
- 2Karlsen, H. & Dong, T. Biomarkers of urinary tract infections: State of the art, and promising applications for rapid strip-based chemical sensors. Analytical Methods 7, 7961–7975 (2015).
- 3Edwards, G. et al. What is the diagnostic accuracy of novel urine biomarkers for urinary tract infection? Biomarker Insights 18, 10.1177/11772719221144459 (2023).10.1177/11772719221144459 PMC 990289836761839 · doi ↗ · pubmed ↗
- 4Mattoo, T. K. & Spencer, J. D. Biomarkers for urinary tract infection: present and future perspectives. Pediatric Nephrol.39 2833–2844 (2024).10.1007/s 00467-024-06321-938483594 · doi ↗ · pubmed ↗
- 5Davenport, M. et al. New and developing diagnostic technologies for urinary tract infections. Nat. Rev. Urol.14 298–310 (2017).10.1038/nrurol.2017.20PMC 547329128248946 · doi ↗ · pubmed ↗
- 6Abbott, I. J., Roberts, J. A., Meletiadis, J. & Peleg, A. Y. Antimicrobial pharmacokinetics and preclinical in vitro models to support optimized treatment approaches for uncomplicated lower urinary tract infections. Expert Rev. Anti Infective Therapy 19 271–295 (2021).10.1080/14787210.2020.181356732820686 · doi ↗ · pubmed ↗
- 7Jayakumar, I., Mathaiyan, J., Mandal, J., Deepanjali, S. & Sreenivasan, S. K. Impact of therapeutic drug monitoring on once-daily regimen of amikacin in patients with urinary tract infection: a prospective observational study, www.drug-monitoring (2020).10.1097/FTD.000000000000080032947556 · doi ↗ · pubmed ↗
- 8Wijma, R. A., Fransen, F., Muller, A. E. & Mouton, J. W. Optimizing dosing of nitrofurantoin from a PK/PD point of view: What do we need to know? Drug Resistance Updates 43 1–9 (2019).10.1016/j.drup.2019.03.00130947111 · doi ↗ · pubmed ↗