Vertebral Metastasis With Syringomyelia Secondary to Breast Adenocarcinoma: A Case Report and Literature Review
Ahmed Reda Abdelhalim, Hossam Tharwat Ali, Bishoy Adel Kamel Zakher, Yara Ashour

TL;DR
A 34-year-old woman with breast cancer developed syringomyelia and spinal issues after treatment, highlighting the need for neurological monitoring in cancer patients.
Contribution
This case report adds to the literature on syringomyelia as a rare complication of vertebral metastasis and cancer treatment.
Findings
A patient with breast cancer and vertebral metastasis developed syringomyelia and myelopathy.
Neurological symptoms following cancer treatment may indicate complications like syringomyelia.
Further clinical awareness and documentation of such cases are recommended.
Abstract
Syringomyelia has several possible causes, commonly including Chiari malformation, spinal cord tumors and injuries, and damage caused by lesions around the spinal cord. A 34‐year‐old female was diagnosed with primary breast cancer and vertebral metastasis and was initiated on an extensive regimen of chemotherapy and radiotherapy. A few months later, she developed numbness and weakness in her lower limbs, and she was concluded to have syringomyelia with surrounding atrophic myelopathy along with vertebral metastasis. Patients developing neurological symptoms following radiotherapy or chemotherapy should be thoroughly evaluated, and further cases should be reported in the literature.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 FIGURE 1
FIGURE 1 FIGURE 2
FIGURE 2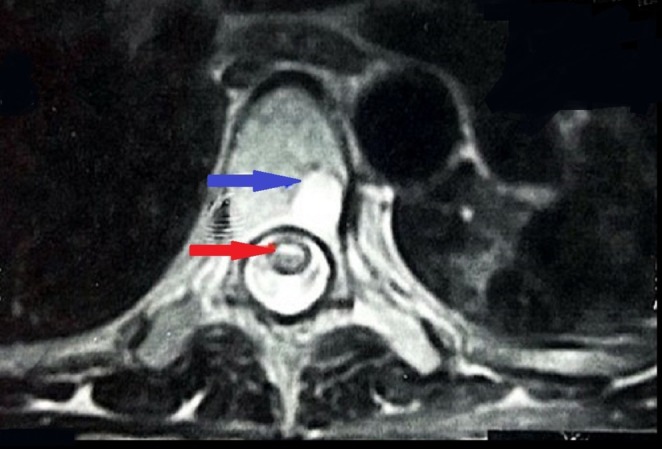 FIGURE 3
FIGURE 3| References | Sex, age (years) | Diagnosis of cancer | Cancer management | Site of syringomyelia | Management of syringomyelia | Follow‐up and special notes |
|---|---|---|---|---|---|---|
| The present case | Female, 34 |
Primary breast cancer (invasive ductal carcinoma Grade 2) Vertebral metastasis |
Chemotherapy involved three doses of doxorubicin (adriamycin) (304.48 mg in total) and eight doses of paclitaxel (taxol) along with five doses of trasuzumab (herceptin) and one dose (Ogivri) Radiotherapy: ten sessions | T4–T10 | None # | The patient deteriorated rapidly and died within 48 h of intensive care unit admission |
| Foster et al. [ | Male, 66 |
Stage “C” colonic adenocarcinoma Widespread metastases including thoracic vertebral body and intramedullary metastasis |
Anterior resection for the colonic tumor | Upper cervical region | Not explicitly detailed | The patient died due to widespread metastasis |
| Foster et al. [ | Female, 55 |
Breast adenocarcinoma, poorly differentiated Intramedullary metastasis in the spinal cord |
Local radiotherapy and oral tamoxifen. After deterioration, a decompressive laminectomy at D6 was performed, revealing a metastatic deposit, which was macroscopically removed. Postoperatively, a second course of radiotherapy was given, followed by rehabilitation | C6–T10 | Decompressive laminectomy. Subsequent imaging showed rostral extension of the syrinx, leading to a second surgery where a shunt was inserted into the syrinx, providing some symptomatic improvement | Patient died a few weeks later due to cerebral secondaries |
| Ostler et al. [ | Male, 37 |
Poorly differentiated squamous cell carcinoma (oropharyngeal carcinoma) |
Primary chemotherapy involved two cycles of carboplatin and 5‐fluorouracil + radical external beam radiotherapy + surgical intervention followed by Iridium‐192 wire brachytherapy | C2–C5 | Syrinx was deemed not suitable for surgical intervention | Although the management of oropharyngeal tumor was completed, the neurological deficit attributed to syringomyelia significantly impacted the patient's quality of life, leading to medical retirement. The patient was a heavy alcoholic |
| Shindo et al. [ | Male, 70 |
Right upper lung adenocarcinoma |
Radiation therapy (48 Gy) on neck and mediastinum | T2–T5 | Not explicitly detailed | The patient developed neurological symptoms eight years after the radiation therapy |
| Poggi et al. [ | Male, 68 |
Undifferentiated small‐cell lung cancer Metastasis to T1 vertebral body a week later |
Chemotherapy (not detailed) | T3–T6 | None # | The patient's neurological manifestations improved. Palliative radiotherapy to the spinal cord was considered but ultimately deferred since the syringohydromyelia did not appear to have a malignant etiology and there was no evidence of cord compression due to the cancer |
| Phuphanich et al. [ | Male, 42 |
Well‐differentiated small‐cell lung adenocarcinoma Metastasis to cerebellopontine angle, brain, and then intramedullary |
Specific treatment for lung adenocarcinoma is not detailed Metastasis: whole‐brain and spinal cord radiation therapy course of 3000 cGy | C4–T10 | None # | The patient passed away two months later |
| Ashawesh et al. [ | Male, 68 |
Small‐cell cancer of the left lung Intramedullary spinal cord metastasis and syringomyelia 4 months later |
Palliative chemotherapy and radiotherapy for the primary lung cancer Urgent radiotherapy applied to spinal cord metastasis | C2–T1 | None # | Spinal cord radiotherapy led to an improvement in the neurological manifestations and the quality of life |
| Zhou et al. [ | Male, 79 |
Primary colorectal diffuse large B‐cell lymphoma Cerebellar metastasis one year later Metastatic spinal intramedullary malignant lymphoma 6 months later |
Ileocecal tumor resection and postoperative chemotherapy with cyclophosphamide, doxorubicin, vincristine, and prednisone (CHOP) plan for 13 cycles For cerebellar metastasis, another 6 cycles of systemic chemotherapy and underwent several courses of local radiotherapy | T2–L3 | Spinal cord radiotherapy and systemic chemotherapy with intrathecal injections of methotrexate | Patient died of multiple organ failure 3 months later |
| van Uum et al. [ | Female, 20 |
Malignant prolactinoma Metastasis to the leptomeninges extending from the brainstem to L5 with thoracic syringomyelia 30 years later |
Occipito‐cervical decompression High‐dose cabergoline therapy | T7–T8 | Thoracic laminectomy at T7 with the insertion of a syringo‐subarachnoidal cerebrospinal fluid (CSF) shunt to alleviate the blockage of CSF flow | Although the tumor load decreased despite these interventions, the patient's walking difficulties and sensory disturbances did not improve post‐surgery, and she remained wheelchair dependent |
| Phuphanich et al. [ | Female, 44 |
Cervical cord astrocytoma |
4500 cGy of local radiation therapy to the cervical cord (C1–C5) followed by surgery to remove the tumor. Post‐surgery, the patient underwent chemotherapy and interferon treatment with the development of what was thought to be a recurrent tumor. This was later confirmed not to be a recurrent tumor but rather radiation necrosis with evidence of multiple sclerosis | T4–T10 | Chemotherapy was initiated as the syrinx was thought to be a cyst of tumor origin; however, it was diagnosed as radiation necrosis with cyst formation on autopsy | The patient died due to respiratory failure |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSpinal Dysraphism and Malformations · Spinal Hematomas and Complications · Nerve Injury and Rehabilitation
Summary
- Although syringomyelia with non‐neurological malignancies is not common, patients developing neurological symptoms following radiotherapy or chemotherapy, even for non‐neurological malignancies, should be thoroughly evaluated for the presence of syringomyelia.
- Tailored management options should be sought.
Introduction
1
Syringomyelia is a neurological disorder in which a fluid‐filled cyst (syrinx) forms within the spinal cord, which can expand enough to damage the spinal cord, causing atrophic myelopathy. Syringomyelia has several possible causes, commonly including Chiari malformation, spinal cord tumors and injuries, and damage caused by lesions around the spinal cord [1, 2]. Additionally, it has been associated with intramedullary metastasis of malignancies of different primary origins [3, 4]. The management of syringomyelia requires a multidisciplinary approach where a thorough evaluation of the patient's risk factors, history, clinical manifestations, and surgical fitness are combined [2, 5].
Some authors suggested that extensive regimens of chemotherapy and radiotherapy can be a cause as well [6, 7]. Yet, there is not enough evidence in the literature to fully conclude radiotherapy and/or chemotherapy as causes of syringomyelia. Similarly, metastatic lytic lesions of the vertebrae have not been strongly linked to the occurrence of syringomyelia [8]. Herein, we report the first case of a young female who had received chemotherapy along with radiotherapy for breast cancer that metastasized to the vertebrae and developed syringomyelia. Furthermore, we have done a review of similar published cases in the literature discussing the common and different points among them [9].
Case History
2
A 34‐year‐old female was diagnosed with primary breast cancer (invasive ductal carcinoma Grade 2) and vertebral metastasis. Computed tomography (CT) showed a lytic bony lesion at the eighth thoracic vertebra (T8) and a bone scan showed increased activity at the seventh thoracic vertebra (T7). Chemotherapy and radiotherapy were initiated. The patient received the first doxorubicin (adriamycin) dose followed by 10 radiotherapy sessions. Two days after the last radiotherapy session, she received the second doxorubicin dose. Shortly after, she developed radiation‐induced gastritis and oral candidiasis. The patient then finished the third dose of doxorubicin (304.48 mg in total). Afterward, she finished eight doses of paclitaxel (taxol) along with five doses of trastuzumab (Herceptin) and one dose (Ogivri). After a few months, she developed numbness and weakness in her lower limbs.
Methods and Investigations
3
She underwent magnetic resonance imaging (MRI) of the cervical, lumber, and dorsal spine. The cervical and lumber MRI were unremarkable; on the other hand, the dorsal MRI showed an appreciable central dilated spinal canal within the spinal cord with reduced remaining spinal cord parenchyma between the fourth and tenth thoracic vertebrae (T4–T10) (Figure 1). It was concluded as syringomyelia with surrounding spinal cord atrophic myelopathy that ended up with paraplegia. Additionally, the MRI showed lytic lesions on the sixth to eighth thoracic vertebrae (T6, T7, and T8) (Figures 2 and 3).
The patient's magnetic resonance imaging, sagittal view of the thoracic vertebrae; the arrows indicate the levels of syringomyelia between the fourth and tenth thoracic vertebrae.
The patient's magnetic resonance imaging, sagittal view of the thoracic vertebrae; the arrows refer to the sixth, seventh, and eight vertebrae with lytic lesions.
The patient's magnetic resonance imaging, transverse view of the sixth thoracic vertebra, showing both syringomyelia (red arrow) and the body lytic lesion (blue arrow).
Results and Outcomes
4
Shortly afterward, the clinical status deteriorated with abnormal laboratory results. Complete blood count (CBC) showed pancytopenia. Liver function tests (AST and ALT) and renal function tests (urea and creatinine) were elevated. Intensive care unit (ICU) admission was required. She died 48 h after the ICU admission.
Discussion
5
Syringomyelia, a longitudinal fluid‐filled cavity inside the spinal cord, can have variable etiologies and underlying mechanisms [2, 5]. It is commonly associated with spinal tumors or structural lesions from the level of foramen magnum [6]. Intramedullary metastasis, although not common, is a possible cause, with lung, breast, colorectal, lymphoma, and melanoma being the common sites for origin [3, 10]. To identify previously reported similar cases of syringomyelia in the context of tumors outside the nervous system, a literature search was carried out on the PubMed database using the following string of keywords: (“Syrinx” OR “syringomyelia” OR “hydromyelia” OR “syringobulbia” OR “syringopontia” OR “syringomesencephaly” OR “syringocephalus”) AND (“chemotherapy” OR “drug” OR “antineoplastic” OR “anticancer” OR “anticancerous” OR “radiotherapy” OR “irradiation” OR “radiation” OR “cancer” OR “neoplasia” OR “neoplasm” OR “Carcinoma” OR “malignant” OR “malignancy” OR “tumor”). A total of 781 results were recruited and screened by two authors independently. Only nine articles describing ten cases were deemed relevant and were described in Table 1.
Of the tabled cases, five were associated with intramedullary metastasis due to lung cancer (two cases) [10, 11], colon cancer (one case) [4], breast cancer (one case) [4], and lymphoma (one case) [12]. In such cases, syrinx involved the level of the cervical and/or thoracic spine. Not only intramedullary metastasis but also vertebral and leptomeningeal metastases that syrinx were reported within previous cases [8, 13]. The present case encompassed a syrinx between the level of the fourth and tenth thoracic vertebrae along with lytic lesions, mostly metastatic lesions from the breast cancer, at the sixth, seventh, and eighth thoracic vertebra. Similarly, a previous case of lung cancer developed vertebral metastasis at the first thoracic vertebra along with a syrinx between the third and sixth thoracic vertebrae [8]. Interestingly, van Uum et al. [13] reported a case with prolactinoma that metastasized to the leptomeninges extending from the brainstem to the fifth lumbar vertebra and associated with a syrinx at the level of the seventh and eighth thoracic vertebrae. While the present case is considered an unusual site for breast cancer metastasis, it is advisable to consider unusual sites of metastasis, especially in complicated cases with an unusual course of disease, and the report of such cases should always be encouraged [9, 15, 16] as well as advanced imaging and screening programs for early detection and better survival of cancer cases, especially in countries where certain cancers are prevalent [17, 18].
Despite the clinical manifestations of the syrinxes, in most cases, seven cases including the present one, there was not a specific treatment or intervention to improve the syrinx or alleviate the associated symptoms. Two cases showed symptomatic improvement following decompressive laminectomy and insertion of syringo‐subarachnoidal cerebrospinal fluid (CSF) shunts [4, 13]. Chemotherapy was tried in two cases [12, 14], while spinal radiotherapy was done in only one case [12].
Although local radiotherapy has been suggested as a treatment option for syringomyelia, some authors argue that syringomyelia can occur as a radiotherapy‐related complication [6]. It is noteworthy that radiotherapy was initiated for malignancies in seven cases including ours [4, 6, 7, 10, 11, 14]. In the case reported by Phuphanich et al. [14], a postmortem examination revealed the syrinx as radiation necrosis rather than a cyst of neoplastic origin. In two cases who had malignancies of primary non‐neurological origins, lung and oropharyngeal carcinomas, with no evidence of either intramedullary or vertebral metastases, the patients developed syringomyelia and neurological symptoms [6, 7]. In one case, chemotherapy and radiotherapy were initiated [6], while only radiotherapy was done for the other [7] as treatment for the primary malignancy.
Notably, only in two case [4, 13], surgical options were attempted in terms of decompressive laminectomy with shunt insertion which provided symptomatic relief. In the case reported by Phuphanich et al. [14], chemotherapy was initiated as the physicians believed it was a cyst of neoplastic origin which later were correctly diagnosed as radiation necrosis in autopsy. Similarly, Zhou et al. [12] reported using spinal cord radiotherapy, intrathecal chemotherapy along with the systemic chemotherapy, most probably as they believed the spinal lesion was a cancerous lesion. The rest of cases did not attempt specific management for syringomyelia. It is essential to consider that the reported cases exhibit complicated cases with rare complication of the syringomyelia which can be challenging to provide comprehensive and timely management.
While the exact mechanism for syringomyelia occurrence is not clear, with some suggested hypotheses for common congenital cases [1, 19], the underlying pathogenesis related to chemotherapy and radiotherapy needs to be extensively studied. For instance, radiation can cause wide changes in the spinal cord, including reactive gliosis, parenchymal necrosis, and disruption of the blood–spinal cord barrier, which all can predispose to CSF circulation disruption and formation of the syrinx [19, 20]. The addition of chemotherapy can increase the possibility of parenchymal necrosis due to multiple metabolic apoptotic pathways [21, 22]. Animal studies also showed that chemotherapy can induce vascular permeability change in the blood–spinal cord barrier [22, 23]. It is noted that in our case, although there was evidence for vertebral metastasis, the role of radiotherapy and chemotherapy in the pathogenesis of syringomyelia cannot be excluded and yet cannot be established definitively. More cases and studies are encouraged to report a definitive link between syringomyelia and the management of non‐neurological cancers.
In conclusion, syringomyelia can have variable etiologies and underlying mechanisms. The present case represents a young female who developed syringomyelia and vertebral metastasis secondary to breast adenocarcinoma. We believe there is no sufficient evidence of syringomyelia with non‐neurological malignancies to fully understand the pathogenesis of syringomyelia in such cases. Patients developing neurological symptoms following radiotherapy or chemotherapy should be thoroughly evaluated and further cases should be reported in the literature.
Author Contributions
Ahmed Reda Abdelhalim: conceptualization, investigation, methodology, writing – original draft. Hossam Tharwat Ali: data curation, methodology, writing – review and editing. Bishoy Adel Kamel Zakher: data curation, writing – original draft. Yara Ashour: data curation, writing – original draft.
Ethics Statement
The study was done in accordance with the ethical standards of the 1964 Helsinki Declaration. Ethics approval was waived by the local committee because no personal data or image was used.
Consent
Informed consent was taken from the patient's husband for this study. Written informed consent was obtained from the patient's husband to publish this case report.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1V. S. Shenoy and S. R. Syringomyelia , Stat Pearls (Stat Pearls Publishing, 2024) Accessed February 17, 2024, http://www.ncbi.nlm.nih.gov/books/NBK 537110/.
- 2W. J. Gardner and J. Angel , “The Mechanism of Syringomyelia and Its Surgical Correction,” Clinical Neurosurgery 6, no. Suppl 1 (1958): 131–140, 10.1093/neurosurgery/6.cn_suppl_1.131.13826542 · doi ↗ · pubmed ↗
- 3R. N. Edelson , M. D. Deck , and J. B. Posner , “Intramedullary Spinal Cord Metastases. Clinical and Radiographic Findings in Nine Cases,” Neurology 22, no. 12 (1972): 1222–1231, 10.1212/wnl.22.12.1222.4346871 · doi ↗ · pubmed ↗
- 4O. Foster , H. A. Crockard , and M. P. Powell , “Syrinx Associated With Intramedullary Metastasis,” Journal of Neurology, Neurosurgery, and Psychiatry 50, no. 8 (1987): 1067–1070, 10.1136/jnnp.50.8.1067.3655816 PMC 1032241 · doi ↗ · pubmed ↗
- 5B. Williams , “The Distending Force in the Production of “Communicating Syringomyelia”,” Lancet 2, no. 7613 (1969): 189–193, 10.1016/s 0140-6736(69)91427-5.4183140 · doi ↗ · pubmed ↗
- 6P. J. Ostler , N. Patel , H. R. Grant , and M. N. Gaze , “Syringomyelia After Chemotherapy and Radiotherapy for Advanced Oropharyngeal Carcinoma: Cause or Coincidence?,” Clinical Oncology (Royal College of Radiologists) 10, no. 5 (1998): 324–326, 10.1016/s 0936-6555(98)80088-5.9848335 · doi ↗ · pubmed ↗
- 7K. Shindo , K. Nitta , A. Amino , T. Nagasaka , and Z. Shiozawa , “A Case of Chronic Progressive Radiation Myelopathy With Cavity Formation in the Thoracic Spinal Cord,” Rinshō Shinkeigaku 35, no. 9 (1995): 1012–1015.8565337 · pubmed ↗
- 8M. M. Poggi and J. Stockel , “Medical Problems in Patients With Malignancy: Case 1. Syringohydromyelia Masquerading as Malignant Cord Compression in a Patient With Small‐Cell Lung Cancer,” Journal of Clinical Oncology 22, no. 19 (2004): 4019–4020, 10.1200/JCO.2004.12.071.15459226 · doi ↗ · pubmed ↗