Medically Attended Outpatient Parainfluenza Virus Infections in Young Children from a Single Site in Machala, Ecuador
Manika Suryadevara, Dongliang Wang, Freddy Pizarro Fajardo, Jorge Luis Carrillo Aponte, Froilan Heras, Cinthya Cueva Aponte, Irene Torres, Joseph Domachowske

TL;DR
This study examines parainfluenza virus infections in young children in Ecuador, revealing their seasonal patterns and health impacts.
Contribution
The study provides new insights into the seasonality and clinical features of PIV infections in coastal Ecuador.
Findings
Parainfluenza viruses were detected in 9% of enrolled children under 5 years old.
PIV infections were most common between March and July, with no shift post-SARS-CoV-2 pandemic.
Clinical manifestations included upper respiratory illness, laryngotracheitis, and bronchiolitis.
Abstract
Parainfluenza virus (PIV) infections contribute to the overall childhood morbidity from acute respiratory illness, yet virus-specific epidemiologic data are lacking across many regions globally. Here, we describe the clinical manifestations, seasonality, and meteorologic associations with PIV infections in Ecuadorian children. Between July 2018 and July 2023, we documented demographic and clinical information from children younger than 5 years seen in a single public health clinic with signs and symptoms consistent with an acute respiratory infection. Nasopharyngeal swabs collected at study enrollment underwent multiplex polymerase chain reaction-based diagnostic testing (Biofire FilmArray v. 1.7™). Regional meteorological data from the same period were provided by Ecuador’s Instituto Nacional de Meteorologia e Hidrologia. Parainfluenza viruses were detected in 9% of the 1251 enrolled…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
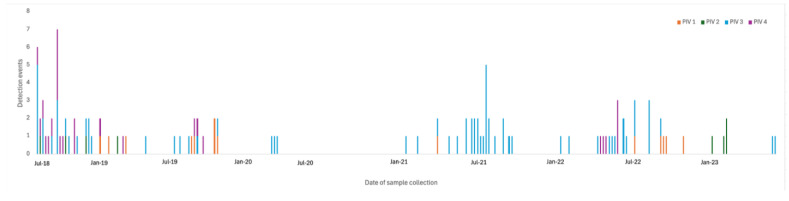 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRespiratory viral infections research · Viral Infections and Vectors · Influenza Virus Research Studies
1. Introduction
Parainfluenza viruses (PIVs) are among the leading causes of lower respiratory tract infections globally, second only to respiratory syncytial virus (RSV), with seasonality of infection varying by virus subtype and geographic region [1,2]. Associated with both upper and lower respiratory tract disease, PIV infections can manifest as otitis media, pharyngitis, laryngotracheobronchitis, bronchiolitis, and/or pneumonia, leading to a large number of medically attended visits and hospitalizations and significantly adding to the economic burden of families, communities, health systems, and national income [1,2].
In the United States, it is estimated that PIVs account for approximately 17% of outpatient viral respiratory disease and 7% of hospitalizations for febrile or respiratory illness in children younger than 5 years. Such infections lead to healthcare costs exceeding 200 million USD annually [2]. Given limited diagnostic testing and reporting of PIV infections throughout much of the world, there are very limited data regarding PIV epidemiology, seasonality, and disease burden globally [3]. A better understanding of regional epidemiology is necessary to optimize the implementation of disease prevention measures, improve the evaluation of resources required for the delivery of needed health care, address and assess healthcare utilization, and promote judicious and appropriate use of antibiotics in the setting of acute respiratory tract illness [3].
Machala is a coastal equatorial city located in the upper middle-income country of Ecuador. Despite existing reports that lower respiratory tract infections are a leading cause of communicable disease and mortality in Ecuador, detailed respiratory virus-specific epidemiologic data from this region are lacking [4,5]. In this study, we describe the epidemiology and clinical manifestations of PIV infections and assess possible meteorological influences on these infections among young children living in coastal Ecuador for periods of time before and after the onset of the SARS-CoV-2 pandemic.
2. Materials and Methods
This study is part of a 5-year cross-sectional surveillance parent study of the etiology and clinical presentation of medically attended outpatient respiratory tract infections among Ecuadorian children less than 5 years of age. The methods for study recruitment and procedures were previously described [6,7]. Subjects were recruited from a single public outpatient clinic in Machala, Ecuador between July 2018 and July 2023. Study enrollment was temporarily paused between March and August 2020 due to restrictions imposed in response to the SARS-CoV-2 pandemic. Data obtained prior to the pause in enrollment are referred to as ‘before the onset of the SARS-CoV-2 pandemic’, while data obtained after enrollment re-started are referred to as ‘after the onset of the SARS-CoV-2 pandemic’. This project is approved by the State University of New York Upstate Medical University Institutional Review Board (IRB number 1102402) and by the Ministry of Health of Ecuador.
2.1. Subject Enrollment
Children younger than 5 years age who were evaluated at a study-designated public outpatient clinic for signs and symptoms consistent with an acute respiratory tract infection (ARTI) were eligible for enrollment. An ARTI was defined by the presence or parental report of two or more of the following symptoms for fewer than 8 days: temperature ≥ 38 °C, nasal congestion or discharge, cough, tachypnea, wheezing, rales, hypoxia, or apnea. Subjects were excluded from enrollment if they were in foster care, had parents who were unable or unwilling to provide consent, or were hospitalized or treated with antibiotics within the last 30 days.
The study team obtained informed consent, then collected and recorded demographic (age, gender, and visit date) and clinical data (symptoms, symptom duration, primary medical diagnosis code, treatment plans, and influenza and pertussis vaccination status). For study purposes, upper respiratory tract infections (URTI) included primary medical diagnoses of nasopharyngitis and laryngotracheitis. Lower respiratory tract infections (LRTI) included diagnoses of bronchitis, bronchiolitis, and pneumonia.
A nasopharyngeal sample was obtained, placed in 3 mL of universal transport, processed and analyzed for the presence of respiratory pathogen nucleic acids using the multiplex PCR-based BioFire Film Array™ Respiratory Panel v1.7 (BioFire Diagnostics LLC, Salt Lake City, UT, USA). This multiplex panel is designed to detect adenoviruses, coronaviruses (HKU1, NL63, 229E, and OC43), human metapneumovirus (hMPV), rhinovirus/enterovirus, influenza viruses (A-H1N1, A-H3N1, B), parainfluenza viruses (PIV) (types 1–4), respiratory syncytial virus, Bordetella pertussis, Chlamydophila pneumoniae, and Mycoplasma pneumoniae.
2.2. Meteorologic Data Collection
Data downloaded from weather towers maintained by Ecuador’s Instituto Nacional de Meteorologia e Hidrologia provided the meteorologic data including temperature (°C), relative humidity (%), barometric pressure (W/m2), and precipitation (mm) for this analysis. The weather tower instruments were calibrated every 3 months and immediately following any necessary repairs. Meteorologic data were collected every minute, continuously, and then summarized as daily, weekly, and/or monthly averages. Means, medians, and ranges were calculated for each week. From the measured data, dew points were calculated using the following formula:
where T = air temperature in °C; RH = relative humidity in percent (%); B = intermediate value (no units) and D = dewpoint in °C.
2.3. Statistical Analysis
Descriptive statistics were used. Continuous data were compared by t-test and categorical data were compared using the Fisher exact or chi-square test, as appropriate. Significance was set a priori to a p value of <0.05. Receiver operating characteristics (ROC) analyses were performed to evaluate the performance of the potential classification factors/models by calculating the sensitivities (true positive rates) and specificities (true negative rates) at each classification threshold. The area under the ROC curve represents an overall measure of the classification accuracy and a bootstrap-based test was performed to assess whether the AUC was different from 0.5, the AUC of a noninformative classification model. Furthermore, the optimal threshold was chosen to maximize the sum of sensitivity and specificity. All factors with significant differences between the two groups were included in multiple logistic regression to derive a composite score for classification, as a weighted average of individual factors. The differences between different logistic models were tested by Rao’s score test.
3. Results
3.1. All Enrolled Subjects
There was a total of 1251 subjects, with a mean age of 19 months, enrolled in this study. Of the enrolled subjects, 117 (9%) samples tested positive for the detection of a parainfluenza virus (Table 1). Of these, 12% were PIV type 1, 7% were PIV type 2, 61% were PIV type 3, and 21% were PIV type 4. Subjects whose nasopharyngeal samples were positive for the detection of PIV were more likely than those whose samples did not detect PIV to report wheezing (20/117 (17%) vs. 73/1134 (6%), p < 0.0001). There were no other statistical associations between demographic and clinical data and PIV detection, specifically no difference in PIV detection by age, gender, diagnosis, and receipt of antibiotics (Table 1).
3.2. Subjects Whose Nasopharyngeal Samples Were Positive for the Detection of PIV
The nasopharyngeal samples from 117 subjects were positive for the detection of a PIV. The mean age of subjects with documented PIV infection was 18 months (range of 1 to 60 months). 57 (49%) of the subjects who tested positive for PIV were younger than 1 year of age, while 60 (51%) were between the ages of 1 and 5 years. Subjects between the ages of 1 and 5 years were more likely than those younger than 1 year of age to report fever with their respiratory illness (54/60 (90%) vs. 41/57 (72%), p = 0.01) and were more likely to have been vaccinated against influenza virus if age eligible (55/60 (92%) vs. 8/31 (26%), p < 0.0001) and pertussis (58/60 (97%) vs. 48/57 (84%), p 0.03). There were no other significant differences between subject age, symptoms, symptom duration, or primary medical diagnosis.
Of the 117 subjects whose nasopharyngeal samples were positive for the detection of a PIV, 14 (12%) detected PIV type 1, 8 (7%) detected PIV type 2, 71 (61%) detected PIV type 3, and 25 (21%) detected PIV type 4 (Table 2). PIV 1 and PIV 4 were more likely to be associated with reports of wheezing with acute respiratory illness and a diagnosis of lower respiratory tract infection compared to PIV 2 and PIV 3 (p < 0.05) (Table 2). There were no other statistical associations between PIV type, age, or gender.
Of the 117 parainfluenza virus positive samples, 29 (25%) also detected at least one other pathogen: 18 (62%) rhinovirus/enterovirus, 5 (17%) RSV, 3 (10%) influenza virus, and 1 (3%) each of human coronavirus, adenovirus, and atypical bacteria. While most of these samples detected 2 co-pathogens, 2 samples detected 3 pathogens (PIV 3 with rhinovirus/enterovirus and RSV; PIV 1 with human metapneumovirus and adenovirus). There were no significant differences between subjects with pathogen co-detection or just detection of a parainfluenza virus with regards to age (mean 17.2 months vs. 17.7 months, p = 0.9), fevers (24/29 (83%) vs. 71/88 (81%), p = 0.8), nasal congestion (28/29 (97%) vs. 82/88 (93%), p = 0.7), cough (19/29 (66%) vs. 51/88 (58%), p = 0.5), wheeze (8/29 (28%) vs. 12/88 (14%), p = 0.08), or symptom duration (mean 3.6 days vs. 3.2 days, p = 0.3).
Among the 117 nasopharyngeal samples that tested positive for the detection of PIV, 57 (49%) were collected prior to the onset of the SARS-CoV-2 pandemic (Table 3). Subjects testing positive for PIV who were enrolled after pandemic onset were more likely to report fever (58 (97%) vs. 37 (65%), p < 0.00001) and less likely to report cough (25 (42%) vs. 45 (79%), p < 0.0001) with their illness. Similarly, those enrolled after pandemic onset were more likely to be diagnosed with an upper respiratory tract infection (59 (98%) vs. 37 (65%), p < 0.001) and less likely to be diagnosed with a lower respiratory tract infection (2 (3%) vs. 14 (25%), p < 0.001).
3.3. PIV Seasonality
Of the 1251 nasopharyngeal samples obtained over a period of 221 weeks, the 117 samples that detected PIV were collected over 72 (33%) different calendar weeks (Figure 1). Most of the PIV activity occurred between March and July. There were no significant changes in general or type-specific PIV seasonality following pandemic onset.
Shown is the study timeline (x-axis) from July 2018 through July 2023 indicating parainfluenza virus (PIV) detection events by type (y-axis).
3.4. Meteorologic Associations
Over the course of the study period, there was evidence of seasonal variation in outdoor air temperature with the highest temperatures occurring during March (mean 28 °C, maximum 34 °C) and the lowest occurring during August (mean 23 °C, minimum 20 °C). Mean relative humidity was found to increase from 71% in January (range 8% to 100%) gradually throughout the year to a high of 85% in November (range 10% to 100%), while mean barometric pressure remained between 1010 W/m^2^ and 1012 W/m^2^.
PIV detection events were associated with periods of lower mean outdoor air temperature (with a temperature threshold of 25 °C), larger humidity range, and higher mean barometric pressure (Table 4). After both univariate and multivariate logistic regression analysis was performed, only mean temperature and humidity range remained associated with PIV detection (Table 5). PIV detection was also associated with rainfall less than 1.15 mm per week, with a 5-week lag (AUC = 0.68; 95% CI 0.60–0.76, p < 0.001). PIV 3, specifically, was detected at a higher frequency during the dry months of June through August than the rainy months of January through April (43/314 (14%) vs. 11/399 (3%), p < 0.0001).
4. Discussion
Over the 5-year study period, we found that PIV 3 was the most frequently detected of the 4 parainfluenza virus types. PIV 3 was more likely than the other virus subtypes to manifest as an upper respiratory infection and was more frequently detected during the dry months than the rainy months. Overall, PIV detection was associated with lower mean outdoor air temperature and larger daily humidity range.
We detected PIV in 9% of subjects seeking medical attention for an acute respiratory infection, a rate higher than what has been previously reported [8,9]. Azziz-Baumgartner found that 6% of children ages 1–4 years with a medically attended acute respiratory tract infection in northwest Ecuador tested positive for parainfluenza virus [8]. A respiratory pathogen surveillance study found that 1.5% of tested samples were positive for parainfluenza virus in Ecuador’s coastal region [9]. Differences in diagnostic testing likely account for the increase in PIV detection in our study with the use of multiplex-PCR assays, which are more sensitive for virus detection than the direct immunofluorescence assays used in the prior studies. Improved diagnostic testing methods lead to a truer understanding of virus-specific epidemiology, data which can be used to guide both prevention and treatment measures. One study published in 2017 found that 57/406 (14%) of children under 5 years of age admitted to the hospital in Quito, Ecuador, for severe pneumonia tested positive for a parainfluenza virus [10]. It is important to note, however, the difference in the study population as Jonnalagadda’s study focused on hospitalized children and our study on children seeking ambulatory medical care.
Participants with nasopharyngeal samples positive for the detection of PIV were more likely to report wheeze than those whose samples did not detect this virus. In addition, 11% of participants with PIV detected in their nasopharyngeal specimen were diagnosed with bronchiolitis. While RSV is the most common cause of viral bronchiolitis, these data support the previously described contribution of PIV to the disease burden of bronchiolitis in young children [11].
Individuals with nasopharyngeal samples positive for the detection of PIV who were enrolled prior to the onset of the SARS-CoV-2 pandemic were more likely to report cough and more likely to be diagnosed with a lower respiratory tract infection, while those enrolled after the pandemic onset were more likely to report fever and more likely to be diagnosed with an upper respiratory tract infection. Similarly, we previously reported in the parent study, that participants whose nasopharyngeal samples detected RSV prior to the onset of the pandemic were more likely to report cough or wheeze and be diagnosed with a lower respiratory tract infection, while those infected with RSV after pandemic onset were more likely to report fever and be diagnosed with an upper respiratory tract infection [7]. We hypothesize that reduced exposure to these viruses may have resulted in a change in clinical manifestations before and after pandemic onset.
Despite this difference in clinical manifestations, there were no differences in the age of infected participants or in the seasonal patterns of PIV circulation following pandemic onset. Non-pharmaceutical interventions put in place to reduce risk of transmission of SARS-CoV-2 led to a reduction in circulation of other respiratory pathogens, such as RSV, with a resurgence of infection (particularly in children older than 1 year of age) seen when restrictions were lifted [12,13]. Data regarding changes in PIV circulation as a result of the use of non-pharmacologic interventions show mixed results. Li et al. and Cho et al. both describe a disappearance of PIV circulation with pandemic onset, followed by a large out of season PIV epidemic shortly after relaxation of non-pharmaceutical interventions [12,13]. Contrary to this finding, and more consistent with our data, Zhao reports that while seasonal prevalence patterns of most respiratory viruses changed with the lifting of the SARS-CoV-2 restriction measures, PIV epidemiology was not substantially impacted by these changes [14]. These observed differences in epidemiology highlight the importance of monitoring regional virus circulation and avoiding extrapolation or overgeneralization of distinct, albeit similar, reported epidemiological patterns.
We found that PIV detection was negatively associated with rainfall, and PIV 3, specifically, was detected with higher frequency during the dry months compared to the rainy months. This is contrary to previous reports that show either no correlation or a positive association between PIV detection and precipitation [15,16,17,18]. It is important to note that the dry months with the highest frequency of PIV cases also were there the cooler months of the year. PIV detection was also associated with lower ambient temperature, a finding that held true through both univariate and multivariate logistic regression analyses, suggesting that temperature was among the main factors influencing PIV circulation and detection. While most of the prior reports show either no association or a positive association between PIV detection and mean temperature, Ciu et al. did find that PIV detection was negatively associated with average temperatures [19]. It is difficult to identify reasons for the varying meteorologic associations with PIV infection across the globe given the scarcity of available data.
Limitations to this study include a sample size that may not be large enough to detect differences in meteorologic factors associated with PIV circulation. Further, this study was conducted at a single site in a city with a climate that differs from the remaining regions of the country, as the coastal areas tend to experience a tropical climate, the nearby mountains have a temperate climate, while the Amazon region has a rainforest climate. The differences in daily temperatures, humidity, and rainfall can impact PIV epidemiology across the country. These factors limit generalizability of the data to other regions, however, are important to report to understand PIV epidemiology in this community. In this study, we included subjects whose nasopharyngeal samples co-detected other pathogens in addition to PIV. We also did not collect information related to past medical history or perinatal complications and therefore are unable to account for potential confounding factors, such as a history of asthma, low birth weight, or prematurity.
5. Conclusions
Parainfluenza viruses contribute to the disease burden of medically attended acute respiratory infections, including bronchiolitis, among young children in Machala, Ecuador. PIV 3, the most frequent of the virus types detected, was most prevalent during months with the coolest temperatures and the least rainfall. These findings can contribute to public health guidance regarding implementation of disease prevention measures, improving evaluation of healthcare delivery resources, and promote judicious use of antibiotics for acute outpatient respiratory tract illnesses.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Rocha-Filho C.R. Ramalho G.S. Martins J.W.L. Lucchetta R.C. Pinto A.C.P.N. da Rocha A.P. Trevisani G.F.M. Reis F.S.d.A. Ferla L.J. Mastroianni P.d.C. Economic burden of respiratory syncytial and parainfluenza viruses in children of upper-middle-income countries: A systematic review J. Pediatr.20239953754510.1016/j.jped.2023.05.00337247828 PMC 10594008 · doi ↗ · pubmed ↗
- 2Branche A.R. Falsey A.R. Parainfluenza virus infection Semin. Respir. Crit. Care Med.20163753855410.1055/s-0036-158479827486735 PMC 7171724 · doi ↗ · pubmed ↗
- 3Li Y. Reeves R.M. Wang X. Bassat Q. Brooks W.A. Cohen C. Moore D.P. Nunes M. Rath B. Campbell H. Global patterns in monthly activity of influenza virus, respiratory syncytial virus, parainfluenza virus, and metapneumovirus: A systematic analysis Lancet Glob. Health 20197 e 1031 e 104510.1016/S 2214-109X(19)30264-531303294 · doi ↗ · pubmed ↗
- 4Institute for Health Metrics and Evaluation: Ecuador Available online: https://www.healthdata.org/research-analysis/health-by-location/profiles/ecuador(accessed on 30 January 2025)
- 5Ecuadorian National Institute for Statistics and Census Available online: https://www.ecuadorencifras.gob.ec/documentos/web-inec/Sitios/Defunciones/(accessed on 30 January 2025)
- 6Sippy R. Prado E.O. Fajardo F.P. Hidalgo I. Aguilar G.V. Bonville C.A. Aponte C.C. Gómez M.S. Aponte J.L.C. Cordova M.B. Medically attended outpatient coronavirus infections in Ecuadorean children during the 20 months preceding countrywide lockdown related to SARS-Co V-2 pandemic of 2020 Pediatr. Infect. Dis. J.202039 e 291e 29610.1097/INF.000000000000284032773657 · doi ↗ · pubmed ↗
- 7Suryadevara M. Wang D. Fajardo F.P. Carrillo Aponte J.L. Heras F. Aponte C.C. Torres I. Domachowske J.B. Clinical, meteorological, and air quality factors associated with ambulatory pediatric respiratory syncytial virus infection in Machala, Ecuador, 2018–2023 Int. J. Environ. Res. Public Health 20252227210.3390/ijerph 2202027240003497 PMC 11855190 · doi ↗ · pubmed ↗
- 8Azziz-Baumgartner E. Bruno A. Daughtery M. Chico M.E. Lopez A. Arriola C.S. de Mora D. Ropero A.M. Davis W.W. Mc Morrow M. Incidence and seasonality of respiratory viruses among medically attended children with acute respiratory infections in an Ecuador birth cohort, 2011–2014 Influenza Other Respir. Viruses 202216243310.1111/irv.1288734432362 PMC 8692806 · doi ↗ · pubmed ↗