SARS-CoV-2 Coronavirus Disease in Patients with Underlying Congenital Inferior Vena Cava Anomalies
Fadia Salman, Pierfrancesco Antonio Annuvolo, Marta Minucci, Francesco Sposato, Ottavia Borghese, Yamume Tshomba

TL;DR
This paper discusses how a 36-year-old man with a rare heart condition developed severe blood clots after contracting COVID-19.
Contribution
The paper presents a rare case linking congenital cardiovascular anomalies with severe DVT following COVID-19.
Findings
Patients with congenital cardiovascular anomalies may develop extensive DVT after contracting COVID-19.
Anticoagulation treatment must be carefully tailored to balance clot prevention and bleeding risks in these patients.
Abstract
Background: COVID-19-related deep vein thrombosis (DVT) in patients with pre-existing congenital anomalies or genetic diseases of the cardiovascular system has been rarely reported, and a clear definition of best treatment in this setting remains undefined. Methods: We report the rare case of a 36-year-old male patient affected with a congenital cardiovascular anomaly, presenting extensive venous thrombosis following COVID-19-induced coagulopathy. An insight into current treatment strategies in this setting is also reported. Results and Conclusions: COVID-19 disease appears to be a determining factor in the development of extensive DVT in patients with congenital anomalies and genetic disorders. Anticoagulation should be tailored to the individual risk factors, balancing the risk-benefit between prevention of VTE and hemorrhagic complications.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
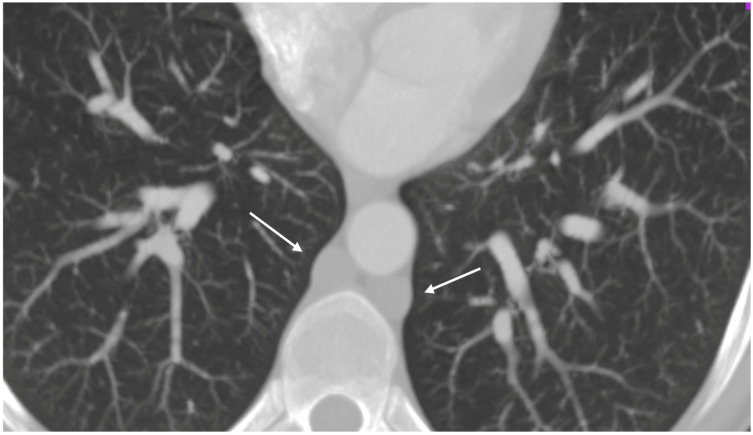 Figure 1
Figure 1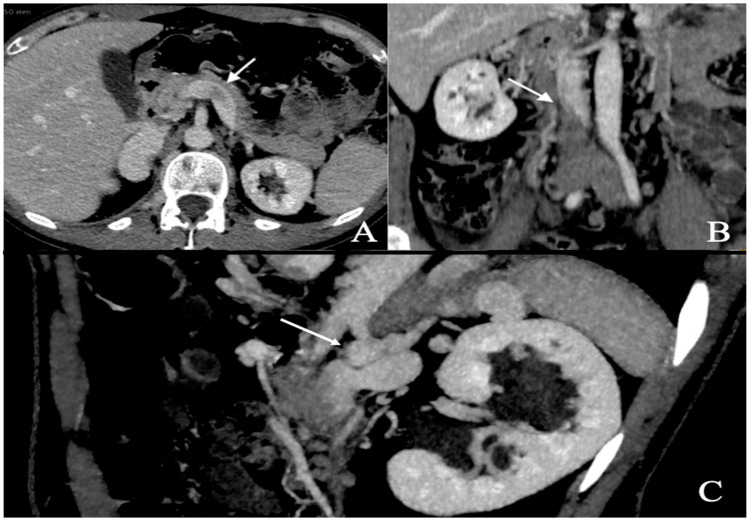 Figure 2
Figure 2| Risk Factors | |
|---|---|
| Individual risk factors | Old age, reduced mobility, obesity, active cancer, history of previous VTE/PE, and congenital anomalies of cardiovascular system [ |
| COVID Severity | Need for admission in ICU. Need for ECMO [ |
| Laboratory tests | Elevated D-dimer (>3 μg/mL), C-reactive protein, ferritin, white blood cell count, and IL-6; Lupus Anticoagulant positivity; fibrinogen > 8 g/L [ |
| Clinical Setting | Treatment |
|---|---|
| Severe COVID-19 (ICU patients)/ventilated patients | Preventive LMWH is recommended [ |
| Patients with specific risk factors for VTE | Thromboprophylaxis should be given during the hospital stay and for 1–2 weeks following discharge and continued for at least three months after VTE [ |
| Patients affected by chronic kidney disease, AKI, or hepatic injury | Caution should be applied in use of anticoagulation as there is an increased risk of bleeding [ |
| Authors, Year | Case |
|---|---|
| Jenab et al., 2022 [ | A 33-year-old man with bilateral DVT and absence of IVC during concurrent COVID-19. |
| Costanzo et al., 2023 [ | An 86-year-old woman with recent hospitalization for severe COVID-19 infection. CT of the abdomen and pelvis revealed a duplicated IVC with a thrombus located in the right IVC. |
| Nam et al., 2022 [ | Sudden massive DVT in a young man with inferior vena cava anomaly 20 h after the second dose of the mRNA vaccine for COVID-19. |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVascular anomalies and interventions · COVID-19 and healthcare impacts · Congenital Heart Disease Studies
1. Introduction
Patients affected with severe or critical COVID-19 may also suffer from cardiovascular complications related to a prothrombotic state [1,2]. Indeed, SARS-CoV-2 acts by binding its spike protein to Angiotensin-Converting Enzyme 2 (ACE2), a membrane-bound aminopeptidase highly expressed in heart and lung cells [3].
This causes endothelial dysfunction aggravated by a dysregulation of the immune system and favors a prothrombotic state with an increased deposition of platelets, circulating inflammatory cells, and protein.
An increased blood viscosity may also lead to venous thromboembolism (VTE) with possible deep vein thrombosis (DVT) and/or pulmonary embolism (PE) [4].
COVID-19-related DVT in patients with pre-existing congenital anomalies or genetic diseases of the cardiovascular system has been rarely reported, and a clear definition of candidates for thrombotic prophylaxis in this setting remains undefined.
Herein, we report the rare case of a 36-year-old male patient affected with a congenital cardiovascular anomaly, presenting extensive venous thrombosis following COVID-19-infection. An insight into current treatment strategies in this setting is also reported.
2. Ethical Statement and Patient Consent
All procedures at our institution are performed following the ethical standards set by institutional and national research committees and the 1975 Helsinki Declaration and its amendments. Our institution does not require ethical approval for reporting individual cases or case series. The patient’s consent was obtained for publication of this report and images.
3. Case Report
A 39-year-old Caucasian male patient presented to the emergency department of our institution with acute back and abdominal pain, and swelling and edema of the lower limbs with cyanosis. He also reported onset of fever, asthenia, rhinorrhea, and odynophagia two weeks earlier and was tested positive for COVID-19 using a nasopharyngeal PCR test. The SARS-CoV-2 test was repeated at admission but yielded a negative result. He had no fever, and O_2_ saturation was >95% in room air.
Blood tests documented increased D-Dimer (752 ng/mL), C-reactive protein (109 mg/L), Interleukin 6 (18.6 pg/mL) and fibrinogen values (435 mg/dL), Interleukin 1, and TNF α, while other inflammatory and coagulative parameters were within the normal range.
A duplex ultrasound of the lower limbs was performed, and deep bilateral vein thrombosis (DVT) of the common femoral and external iliac veins with possible involvement of the inferior vena cava (IVC) was detected.
The patient denied personal and family history of important thrombotic events. The congenital and acquired thrombophilic risk tests were normal.
A respiratory alkalosis was found at the blood gas analysis so in suspicion of PE, Computed Tomography Angiography (CTA) was performed and did not detect any sign of pulmonary thromboembolism but azygos and hemiazygos vein dilatation (Figure 1) and a congenital abnormality of the IVC, in addition to DVT of iliaco-femoral veins with involvement of the IVC, renal veins, and mesenteric vein (Figure 2). Anticoagulation with low molecular weight heparin (LMWH) 1 mg/kg every 12 h subcutaneously was started.
Symptoms rapidly improved during hospital stay, and the patient was discharged home in good clinical conditions. Oral anticoagulation was continued with rivaroxaban 20 mg daily for 3 months.
At the 3-month follow-up visit, the patient’s clinical status was stable, with persistence of mild edema and swelling of the lower limbs but no pain. Duplex ultrasound showed a partial recanalization of common femoral veins with no improvement at the level of the iliac arteries.
The patient was continued on oral anticoagulant therapy for 12 months, and his clinical condition remained stable.
He is still under an ongoing follow-up.
4. Discussion
The coagulopathic profile of COVID-19 has been widely recognized and is largely attributed to a profound dysregulation of the coagulation cascade, primarily driven by an exaggerated inflammatory response known as the “cytokine storm”, with elevated levels of tumor necrosis factor-α (TNF-α), interleukin (IL)-1, IL-6, and other chemokines contributing to endothelial dysfunction, platelet activation, and hypercoagulability [5,6,7,8,9]. This has translated into a high incidence of thrombotic complications among hospitalized patients, including pulmonary embolism (PE) and deep vein thrombosis (DVT), with reported rates of 16.5% and 14.8%, respectively [10].
In the context of viral infections, the thrombogenic potential of SARS-CoV-2 appears particularly pronounced compared to other pathogens such as HIV (1.5% incidence of VTE in non-injecting drug users) [11] or H1N1 influenza (5.9%) [12]. This suggests an intrinsic prothrombotic signature associated with COVID-19, particularly in patients with pre-existing risk factors for venous thromboembolism (VTE), including congenital anomalies of the cardiovascular system (Table 1) [13,14].
Our patient presented with extensive DVT following a recent COVID-19 infection and was subsequently found to have a congenital atresia of the inferior vena cava (IVC). IVC agenesis or atresia is an exceptionally rare condition, with an estimated prevalence of 0.0005–1% in the general population [15]. This anomaly, often underdiagnosed, predisposes to venous stasis and increases the risk of thrombotic events, especially in young patients. While the exact etiology remains uncertain, both congenital malformation and in utero thrombosis have been postulated as causative mechanisms [15,16].
Notably, DVT may occur in patients with IVC anomalies even in the absence of identifiable prothrombotic triggers [17]. However, in the presence of COVID-19-induced coagulopathy, the thrombotic risk may be amplified, suggesting a synergistic interaction between underlying vascular anomalies and systemic inflammatory states.
The recent literature highlights the lack of consensus on optimal prophylactic strategies for VTE in the context of COVID-19. Some studies proposed intensified anticoagulation regimens early in the pandemic, but subsequent trials have emphasized the need for individualized risk stratification based on disease severity, body mass index, renal function, and coagulation markers such as D-dimer [18,19,20,21]. While standard-dose low molecular weight heparin (LMWH) remains the cornerstone for thromboprophylaxis in most hospitalized patients, intermediate or therapeutic dosing should be reserved for selected high-risk populations, such as those with obesity (BMI > 30 kg/m^2^), mechanical ventilation, or markedly elevated D-dimer levels [22,23] (Table 2).
Susen et al. recommend standard LMWH prophylaxis (e.g., enoxaparin 4000 IU daily) for patients with intermediate thrombotic risk, and dose adjustments based on weight or renal insufficiency (e.g., unfractionated heparin for creatinine clearance < 30 mL/min) [23]. Importantly, in the absence of critical illness, therapeutic anticoagulation does not confer added benefit and may increase the risk of bleeding [22,24,25].
Antiplatelet therapy, while explored in the context of long-COVID-related endothelial dysfunction, has not demonstrated efficacy in the acute phase of COVID-19 for VTE prevention [15,17]. Thus, its routine use for prophylaxis in this setting is not supported.
Congenital IVC anomalies are rarely discussed in the COVID-19-related thrombosis literature, but several recent case reports underscore their clinical relevance (Table 3). In one case, a young male developed massive DVT following mRNA vaccination, prompting thrombectomy and lifelong anticoagulation [26]. Other cases were managed conservatively with LMWH followed by oral anticoagulants [27,28].
Given the paucity of robust data, thromboprophylaxis in patients with congenital IVC anomalies should be guided by a thorough evaluation of individual risk factors such as age, immobility, malignancy, and prior thrombotic events. In our case, the patient did not undergo thromboprophylaxis during COVID-19 infection, considering that the anomaly of the vena cava was not yet known and that the COVID-19 infection was not associated with further significant thromboembolic risk factors (age, mildness of the clinical manifestations of the infection, absence of immobility, etc.). The thrombotic event was treated with LMWH in the acute phase, then transitioned to a DOAC despite the atypical localization of the thrombosis, with favorable outcomes.
In summary, congenital IVC anomalies may act as amplifiers of thrombotic risk in the presence of COVID-19-induced coagulopathy. However, the general principles of VTE management in COVID-19 patients—namely, risk stratification, tailored anticoagulation, and cautious duration of therapy—remain applicable. Larger studies are needed to establish specific guidelines for this unique patient subgroup.
5. Results and Conclusions
COVID-19 disease has been shown to induce endothelial cell damage and lead to a hypercoagulable condition even in the absence of pre-existing alterations of the coagulative status, with an increased incidence of DVT or PE in affected patients.
The impact of COVID-19-induced coagulopathy on underlying congenital anomalies and genetic diseases has been rarely reported but appears to be a determining factor in the development of extensive deep vein thrombosis.
There remains great variability in the approach to anticoagulation in COVID-19 which should be customized according to individual risk factors balancing the risk–benefit between the prevention of VTE and hemorrhagic complications.
Further studies are needed to indicate a definitive treatment strategy in this setting.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Wu P. Hao X. Lau E.H.Y. Wong J.Y. Leung K.S.M. Wu J.T. Cowling B.J. Leung G.M. Real-time tentative assessment of the epidemiological characteristics of novel coronavirus infections in Wuhan, China, as at 22 January 2020 Euro Surveill.202025200004410.2807/1560-7917.ES.2020.25.3.200004431992388 PMC 6988272 · doi ↗ · pubmed ↗
- 2Turner A.J. Hiscox J.A. Hooper N.M. ACE 2: From vasopeptidase to SARS virus receptor Trends Pharmacol. Sci.20042529129410.1016/j.tips.2004.04.00115165741 PMC 7119032 · doi ↗ · pubmed ↗
- 3Zheng Y.Y. Ma Y.T. Zhang J.Y. Xie X. COVID-19 and the cardiovascular system Nat. Rev. Cardiol.20201725926010.1038/s 41569-020-0360-532139904 PMC 7095524 · doi ↗ · pubmed ↗
- 4Di Minno A. Ambrosino P. Calcaterra I. Di Minno M.N.D. COVID-19 and Venous Thromboembolism: A Meta-analysis of Literature Studies Semin. Thromb. Hemost.20204676377110.1055/s-0040-171545632882719 PMC 7645842 · doi ↗ · pubmed ↗
- 5Tuck A.A. White H.L. Abdalla B.A. Cartwright G.J. Figg K.R. Murphy E.N. Pyrke B.C. Reynolds M.A. Taha R.M. Haboubi H.N. To scan or not to scan—D-dimers and computed tomography pulmonary angiography in the era of COVID-19Clin. Med.202121 e 155e 16010.7861/clinmed.2020-0664 PMC 800278033593831 · doi ↗ · pubmed ↗
- 6van den Berg M.J.W. Waanders D. Kooistra E.J. Kox M. Pickkers P. The value of D-dimer to predict pulmonary embolism in critically ill COVID-19 patients J. Crit. Care 202164182110.1016/j.jcrc.2021.03.00233770571 PMC 7942150 · doi ↗ · pubmed ↗
- 7Leentjens J. Van Haaps T.F. Wessels P.F. Schutgens R.E.G. Middeldorp S. COVID-19-associated coagulopathy and antithrombotic agents-lessons after 1 year Lancet Haematol.20218 e 524e 53310.1016/S 2352-3026(21)00105-833930350 PMC 8078884 · doi ↗ · pubmed ↗
- 8Harzallah I. Debliquis A. Drénou B. Lupus anticoagulant is frequent in patients with COVID-19J. Thromb. Haemost.2020182064206510.1111/jth.1486732324958 PMC 7264773 · doi ↗ · pubmed ↗