Encrusted Cystitis in a Child Without Predisposing Factors: A Case Report and Literature Review
Shohei Yoshimura, Kengo Hattori, Emi Tsuji, Jiro Tsugawa

TL;DR
A six-year-old girl with no known risk factors was diagnosed with rare encrusted cystitis, and her symptoms improved after treatment.
Contribution
This case report highlights bladder and bowel dysfunction as a potential risk factor for encrusted cystitis in children without typical predisposing factors.
Findings
The patient was diagnosed with encrusted cystitis after tests revealed bladder wall calcification and Proteus mirabilis infection.
Symptoms resolved following antibiotic treatment and transurethral resection of bladder calcification.
The case suggests bladder and bowel dysfunction may contribute to encrusted cystitis in children without traditional risk factors.
Abstract
A six-year-old girl was admitted to our hospital with rectal prolapse, urinary frequency, urinary stone drainage, and recurrent febrile urinary tract infections. A urinary culture identified Proteus mirabilis, and an ultrasonography demonstrated mucosal calcification of the bladder wall, leading to the diagnosis of encrusted cystitis. Antibiotic administration and transurethral resection of bladder calcification were performed, and her symptoms gradually disappeared. Encrusted cystitis is extremely rare in childhood and is frequently observed in patients with post-renal transplantation, urological interventions, and immunosuppressive status. She did not have these predisposing factors; thus, bladder and bowel dysfunction may be a potential risk factor for encrusted cystitis.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
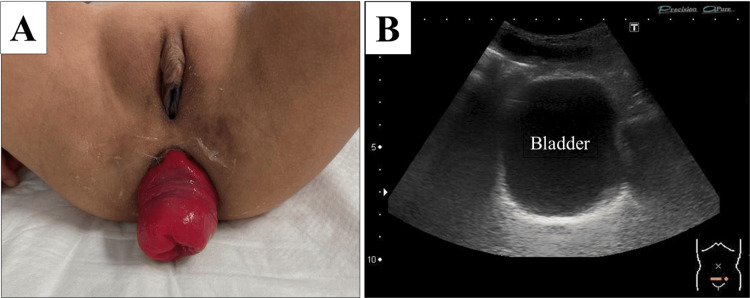 Figure 1
Figure 1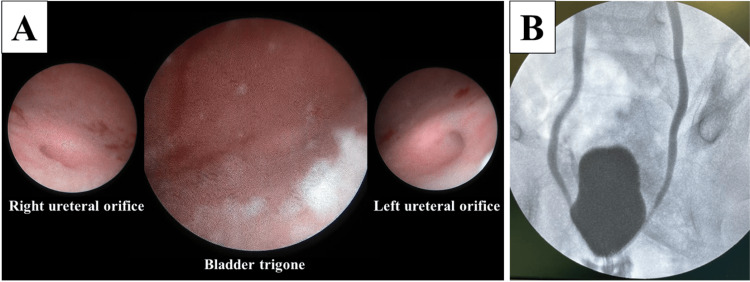 Figure 2
Figure 2| Case | Age | Gender | Background | Microorganism | Antibiotics | Resection | Acidification |
| 1 [ | 8 | M | Post-renal transplantation | C. urealyticum | Yes | Open | Yes |
| 2 [ | 9 | M | Ascending pyelography for ectopic kidney | C. urealyticum | Yes | No | No |
| 3 [ | 9 | M | Bladder neck operation for bladder exstrophy | C. urealyticum | Yes | Transurethral | No |
| 4 [ | 12 | F | Bladder biopsy for Hinman syndrome | C. urealyticum | Yes | Transurethral | No |
| 5 [ | 13 | M | Post-renal transplantation | C. urealyticum | Yes | No | Yes |
| 6 [ | 15 | F | High-dose steroid use for hereditary angioedema | C. urealyticum | Yes | Transurethral | No |
| Present case | 6 | F | Rectal prolapse, no urological intervention | P. mirabilis | Yes | Transurethral | No |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDiphtheria, Corynebacterium, and Tetanus · Urinary Tract Infections Management · Enterobacteriaceae and Cronobacter Research
Introduction
Encrusted cystitis (EC) is a rare chronic inflammatory condition of the bladder, clinically characterized by the formation of struvite calcifications of the bladder mucosa [1]. These calcifications are caused by the action of urea-splitting bacteria, including species such as Corynebacterium, Proteus, Klebsiella, and Pseudomonas [2]. These bacteria produce ammonia through the urea hydrolysis, which disrupts the glycosaminoglycan layer of the bladder, resulting in the formation of struvite stones and calcification of the bladder wall [3].
A history of renal transplantation, previous urological intervention, bladder catheterization, or immunosuppressed status has been identified as a potential risk factor for the development of EC in both adult and pediatric populations [1,4]. Consequently, EC without these predisposing factors is exceedingly rare in the literature, with only one adult case having been previously reported [3]. In this case report, we present a pediatric case of EC that lacks any reported cofactors.
Case presentation
A six-year-old girl with an autism spectrum disorder presented to our outpatient clinic with a two-month history of recurrent rectal prolapse (Figure 1A). Moreover, the patient exhibited symptoms of urinary frequency, suprapubic pain, an unpleasant odor in the urine, and urinary stones. She had no history of immunodeficiency or immunosuppressive treatment and no medication for autism spectrum disorder. Magnesium oxide had been administered for four months to treat constipation. The urinalysis yielded a pH of 9.0, hematuria, and proteinuria in the outpatient clinic. Additionally, the calculus analysis indicated the presence of 83% ammonium magnesium phosphate calculus, also known as struvite stones. Despite the replacement of magnesium oxide with polyethylene glycol, her symptoms persisted for a few months, accompanied by recurrent febrile urinary tract infections (UTIs). A urinary culture obtained during a febrile UTI detected 1 × 10^5^ colony-forming units/mL Proteus mirabilis, which was identified as the causative bacterium. An abdominal ultrasound revealed the presence of calculi deposition on the bladder wall (Figure 1B), which led to the diagnosis of EC.
Physical and ultrasonographic findings.(A) Rectal prolapse in the outpatient clinic. (B) Ultrasound of the bladder showing a 5-mm-thickened calcification of the entire bladder wall.
A cystoscopy under general anesthesia demonstrated calcium deposits concentrated around the bladder trigone and sclerosis of the bilateral ureteral orifices (Figure 2A). Intraoperative cystography confirmed secondary bilateral vesicoureteral reflux (Figure 2B). In addition to intravenous antibiotics administration for Proteus mirabilis for four weeks, transurethral resection of the bladder wall calcification was performed. Her symptoms cleared gradually, and the follow-up urinalysis revealed a normal pH level and no evidence of hematuria or proteinuria. The calcium deposit on the bladder wall observed on the ultrasonography was no longer present eight months later. She had no recurrence of rectal prolapse and UTI for more than one year.
Intraoperative findings.(A) Cystoscopy showing calcium deposits centered on the bladder trigone and sclerosis of the bilateral ureteral orifices. (B) Intraoperative cystography showing secondary bilateral vesicoureteral reflux.
Discussion
EC is a rare chronic UTI associated with bladder wall calcification, first described in 1914 by Francois [5]. It is most prevalent in elderly patients or those with predisposing risk factors, including a history of renal transplantation, urological procedures, or immunosuppressive medications [1,4]. The diagnosis of EC in childhood is exceedingly rare, with only seven pediatric cases (median age at diagnosis: nine years, male-to-female ratio 4:3) having been previously reported in the English literature, including our case (Table 1) [6-9]. Among the seven patients, three (43%) had undergone prior urological interventions, two (29%) had a history of renal transplantation, and one (14%) was on long-term corticosteroid therapy. To the best of our knowledge, this is the only reported pediatric case of EC reported without predisposing factors.
In the present case, rectal prolapse resulting from uncontrolled constipation was considered the primary cause of EC, which indicated a correlation with the pathophysiology of bladder and bowel dysfunction (BBD). BBD is typified by lower urinary symptoms such as dysuria and urinary frequency, in conjunction with bowel complaints as represented by constipation, and is frequently seen in children diagnosed with behavioral and neuropsychiatric disorders, such as autism spectrum disorder [10]. As a mechanism of BBD, rectal distension due to chronic constipation has been demonstrated to exert mechanical and neurological effects on the capacity, contractility, and sensation of the bladder [11]; therefore, in our case, chronic constipation with rectal prolapse affected bladder dysfunction, resulting in the growth of urinary tract bacteria. Corynebacterium urealyticum has been recognized as the most prevalent causative microorganism for EC, and Proteus mirabilis, a urea-splitting bacterium, has also been identified as a causative microorganism for EC. Ammonia produced from urea hydrolysis has been observed to alkalinize and disrupt the glycosaminoglycan layer of the bladder mucosa, thereby facilitating bacterial adhesion [3]. Ultimately, this process leads to the formation of struvite stones and bladder wall calcification, which in turn contribute to the development of EC.
The presence of bowel dysfunction, including constipation and fecal incontinence, has not been described among the seven patients in this study. However, Hinman syndrome is a known disease that can lead to BBD [10]. Therefore, although case 4 had a traumatic event of bladder biopsy one year before the development of EC [8], the patient may have developed EC through a similar mechanism as our case. In the future, an increase in EC cases may reveal an association between EC and BBD. Furthermore, routine evaluation of bowel habits may contribute to the diagnosis, particularly in pediatric patients with recurrent UTIs and lower urinary tract symptoms.
As treatments for EC, the most common approaches are the administration of appropriate antibiotics against microorganisms, the elimination of calcareous incrustation, and urine acidification [2]. Our review of the literature revealed that all patients required antibiotics for the causative bacterium, and 5/7 (71%) underwent transurethral or open resection of the bladder wall calcification. Urine acidification was indicated for only 2/7 (29%) patients, both of whom had both EC and encrusted pyelitis following post-renal transplantation. In one of these patients (case 5), nephrostomy and graft removal were also necessary. However, the prognosis was favorable, with a curable condition in all patients. In our case, optimizing bowel function in addition to antibiotic administration and transurethral resection of the bladder wall calcification was crucial to achieving a cure of EC.
Conclusions
We showed a pediatric EC case without predisposing cofactors such as renal transplantation, urinary interventions, and immunosuppressants. BBD is a possible associated factor for EC in children, and an accumulation of EC cases may reveal an association between EC and BBD in the near future.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Encrusted cystitis and pyelitis J Urol Meria P Desgrippes A Arfi C Le Duc A 3916019989628593 · pubmed ↗
- 2Etiology, pathogenesis, diagnosis and treatment of encrusted cystitis and pyelitis: Review of the problem from a historical perspective Rev Mex Urol Soriano-García F Fernández-Natal I 112842024
- 3Encrusted cystitis secondary to Corynebacterium glucuronolyticum in a 57-year-old man without predisposing factors Lab Med Curry CR Saluja K Das S Thakral B Dangle P Keeler TC Watkin WG 1361394620152591819210.1309/LMXQP 557EINXBXIF · doi ↗ · pubmed ↗
- 4Encrusted uropathy: a comprehensive overview-to the bottom of the crust Front Med (Lausanne) Van de Perre E Reichman G De Geyter D Geers C Wissing KM Letavernier E 609024720203355320510.3389/fmed.2020.609024 PMC 7858656 · doi ↗ · pubmed ↗
- 5La cystite incrustée J Urol Méd Chir Francois J 355251914
- 6Successful treatment of encrusted cystitis and pyelitis with preservation of renal graft Transplantation Lee R Clement MR Carr MC Canning DA Brayman KL 3023037820041528069810.1097/01.tp.0000135140.12454.f 4 · doi ↗ · pubmed ↗
- 7Corynebacterium group D 2 as a cause of alkaline-encrusted cystitis: report of four cases and characterization of the organisms J Clin Microbiol Soriano F Ponte C Santamaria M Aguado JM Wilhelmi I Vela R Delatte LC 788792211985399811110.1128/jcm.21.5.788-792.1985 PMC 271782 · doi ↗ · pubmed ↗
- 8Encrusted cystitis and pyelitis in children: an unusual condition with potentially severe consequences Urology Meria P Margaryan M Haddad E Dore B Lottmann HB 5695736420041535159510.1016/j.urology.2004.04.013 · doi ↗ · pubmed ↗