Thyroid Storm Triggered by Partial Hydatidiform Mole: A Rare and Life-Threatening Complication
Hailey Cox, Maggie Wong, Jena Preszler, Nikolina Docheva, Nauman Khurshid

TL;DR
A rare case of thyroid storm caused by a partial hydatidiform mole in a pregnant woman is reported, highlighting the need for specialized care.
Contribution
This case report documents a rare life-threatening complication of partial hydatidiform mole: thyroid storm.
Findings
A 26-year-old woman presented with thyroid storm and preeclampsia due to a partial molar pregnancy.
Elevated beta hCG and suppressed TSH confirmed the diagnosis of thyroid storm.
The case underscores the importance of managing such complications in a tertiary care center.
Abstract
A 26-year-old woman, gravida 1 para 0 at 14 weeks' 1-day gestation, presented with vaginal spotting and systemic symptoms, including palpitations, shortness of breath, heat intolerance, nausea, and vomiting for 2 weeks. Workup revealed maternal tachycardia, severe-range blood pressure, elevated beta human chorionic gonadotropin of 2,442,400 mIU/mL, suppressed thyroid stimulating hormone, and elevated T4, consistent with thyroid storm with possible preeclampsia with severe features. 1 A transvaginal ultrasound suggested a partial molar pregnancy; this was later confirmed by surgical pathology. This case highlights the rare yet serious complications of hydatidiform mole, in particular, a partial molar pregnancy, including thyroid storm and superimposed preeclampsia, emphasizing the importance of management at a tertiary care center with a multidisciplinary team to optimize maternal…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Fig. 1
Fig. 1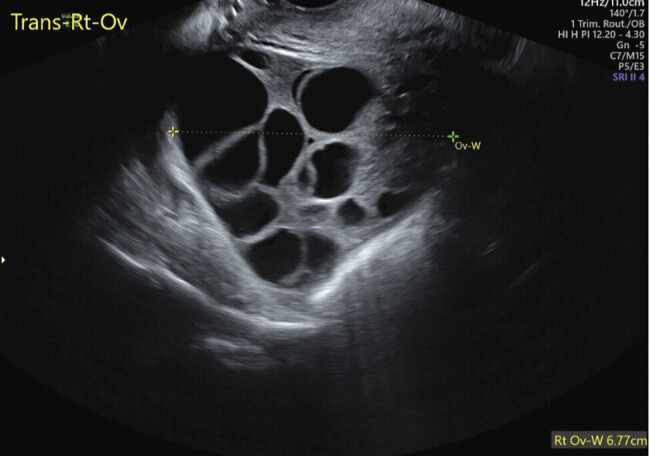 Fig. 2
Fig. 2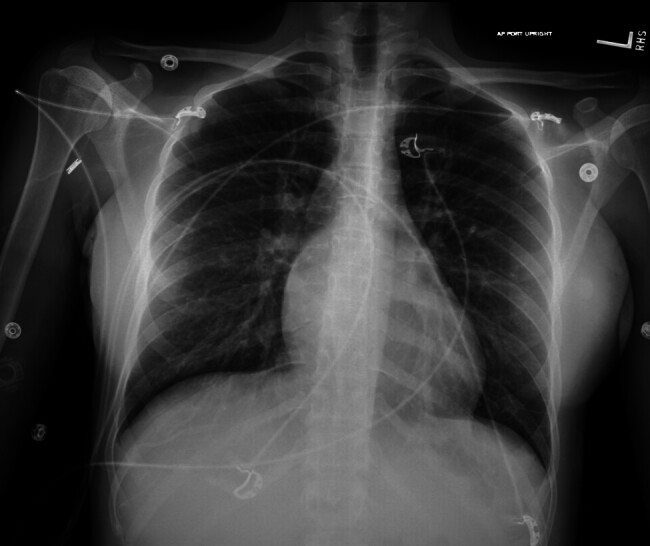 Fig. 3
Fig. 3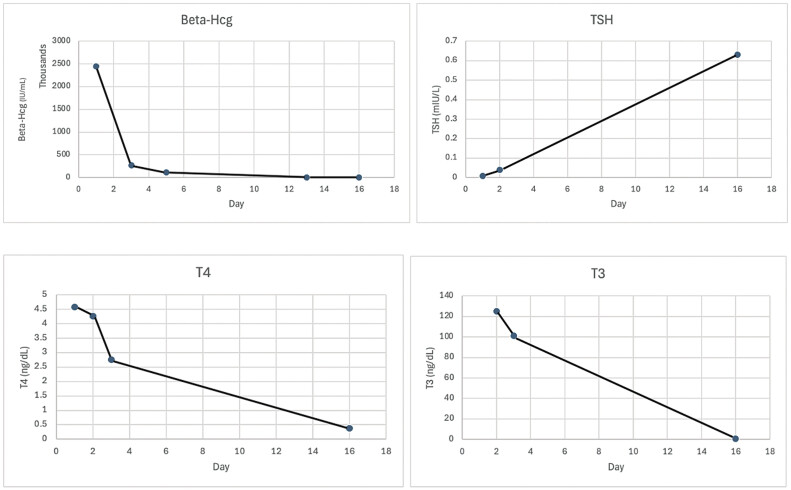 Fig. 4
Fig. 4| Clinical focus | Actions and intervention |
|---|---|
| Initial evaluation | • Vital signs: heart rate, blood pressure, temperature, respiratory rate |
| Diagnosis | • Partial molar pregnancy |
| Available services | • Transfer to a tertiary center |
| Medical management | Thyroid storm |
| Surgical management | Dilation and evacuation |
| Postoperative care | • SICU monitoring |
| Surveillance and follow-up | • Weekly β-hCG until undetectable, then monthly ×6 mo |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGestational Trophoblastic Disease Studies · Prenatal Screening and Diagnostics
Case Report
A 26-year-old woman, gravida 1 para 0 at 14 weeks' 1-day gestation (based on her last menstrual period and confirmed by an 8-week, 1-day ultrasound), presented to a community hospital emergency department with new-onset vaginal spotting. She had been experiencing intermittent heart palpitations, shortness of breath, night sweats, hot flashes, nausea, and vomiting for 2 weeks. Her medical, surgical, and family history were unremarkable. She was taking only a prenatal vitamin, had no known allergies, and denied the use of tobacco, alcohol, or illicit drugs. She had received regular prenatal care, including a normal first-trimester ultrasound.
On arrival at the outside hospital, her vital signs were as follows: heart rate = 170s beats/min, blood pressure = 146/63 mm Hg, respiratory rate = 18 breaths/min, temperature = 36.8°C, SpO2 = 99% on room air. Initial notable laboratory values were beta-human chorionic gonadotropin (β-hCG) = 2,442,400 mIU/mL, thyroid stimulating hormone < 0.02 mIU/mL, T4 >24.9 ug/dL, hemoglobin (Hgb) = 9.8 g/dL. Other notable laboratory values included new-onset proteinuria with a urine protein–creatinine ratio of 0.34.
A transvaginal ultrasound revealed a gestational sac with a fetal pole measuring 80 mm (14w0d), a fetal heart rate of 137 beats/min, posterior placenta with echogenicity suggesting a snowstorm appearance, most consistent with partial molar pregnancy ( Fig. 1 ). Theca lutein cysts were also noted bilaterally on full surveillance of the pelvis ( Fig. 2 ).
Transvaginal ultrasound of partial hydatidiform mole with classic “snowstorm” appearance.
Transvaginal ultrasound of theca lutein cysts within ovary at the time of partial hydatidiform mole diagnosis.
The patient was diagnosed with suspected partial molar pregnancy complicated by thyroid storm and hypertensive emergency. 4 5 6 7 She was transferred to a tertiary care center for management. She was given propranolol for heart rate control prior to transport.
The patient received care from a multidisciplinary team, including obstetrics and gynecology, maternal–fetal medicine, critical care, endocrinology, and gynecologic oncology specialists. Her notable vital signs on arrival were a heart rate of 110 beats/min and blood pressure of 155/82 mm Hg. Her case was immediately discussed with maternal–fetal medicine and the critical care team. She was placed on continuous telemetry and pulse oximetry monitoring and initially had hourly blood pressure monitoring. A chest X-ray demonstrated no acute findings ( Fig. 3 ). Her electrocardiogram revealed sinus tachycardia and an echocardiogram showed a normal ejection fraction, mild-to-moderate mitral regurgitation, and probable patent foramen ovale.
Negative chest X-ray at the time of partial hydatidiform mole diagnosis.
The patient had multiple sustained severe-range blood pressures with a high suspicion for superimposed preeclampsia with severe features. She was started on intravenous (IV) magnesium for seizure prophylaxis. Her blood pressures were initially treated with IV antihypertensive agents followed by long-acting oral agents, including labetalol and nifedipine XL, which were slowly titrated up throughout her hospital stay. For the management of thyroid storm, she was started on propylthiouracil (PTU) 1,000 mg orally followed by 200 mg orally every 6 hours, hydrocortisone 100 mg IV every 8 hours for three doses, and potassium iodide 0.25 mL orally every 8 hours (2 hours following PTU).
Given the partial molar pregnancy, thyroid storm, and concern for preeclampsia with severe features, the decision was made to proceed with medical termination with dilation and evacuation due to the high risk of maternal morbidity and mortality. 4 Preoperative preparation for surgery included laminaria placement the night before and preparation for possible postpartum hemorrhage during the procedure.
Dilation and evacuation under ultrasound guidance were performed. She received 200 mg orally doxycycline for surgical prophylaxis. Her quantitative blood loss was 1,200 mL. She received TXA 1 g IV, misoprostol 1,000 µg rectally, and 2 units of packed red blood cells intraoperatively. Otherwise, the procedure was uncomplicated. Her Hgb remained stable at 8.7 g/dL and higher for the remainder of her admission. She was transferred to the SICU following the procedure for close monitoring. Endocrinology and gynecologic oncology were consulted.
She was continued on PTU 200 mg orally every 4 hours and hydrocortisone 100 mg IV every 8 hours for thyroid storm management along with labetalol 300 mg orally every 8 hours and nifedipine XL 30 mg orally every 12 hours for blood pressure management. Due to persistently elevated blood pressures, oral antihypertensive agents were titrated accordingly. Magnesium sulfate was discontinued after 24 hours.
On postoperative day 1, the patient's laboratories was downtrending appropriately ( Fig. 4 ). IV hydrocortisone and orally PTU were discontinued and she was started on methimazole 15 mg daily. The patient was discharged on POD 3 once her tachycardia had resolved, blood pressures were < 150/< 100 mm Hg, and she was meeting all other postoperative milestones. She was discharged on methimazole 15 mg orally daily, labetalol 600 mg orally every 8 hours, and nifedipine XL 30 mg orally every 12 hours. Repeat β-hCG laboratories were being trended weekly until undetectable, then monthly for 6 months to monitor for progression to gestational trophoblastic neoplasia. 9 The pathology returned in 1 week and demonstrated hydropic villi tissue mixed with chorionic villi, decidua, and male fetus, consistent with partial hydatidiform mole. The patient received a Nexplanon for reliable contraception at her postoperative visit.
Trend of β-hCG and TSH profile before and after management of partial hydatidiform mole. β-hCG, beta human chorionic gonadotropin; TSH, thyroid stimulating hormone.
Conclusion
This case highlights the complexity of a partial molar pregnancy and its rare, potentially fatal complications, including thyroid storm and superimposed preeclampsia, emphasizing the importance of early recognition and multidisciplinary team coordination to optimize maternal outcomes. 1 Similar to complete hydatidiform moles, partial molar pregnancies can manifest a thyroid storm if β-hCG levels are high enough. 8 Early intervention and expertise from a multidisciplinary team at a tertiary care center were crucial to the successful recovery of this patient. Treatment with antithyroid medications, corticosteroids, antihypertensive agents, and expedient surgical management was critical in optimizing outcomes. 7 Postoperative surveillance is essential, including β-hCG monitoring, effective contraception, blood pressure control, and appropriate follow-up care with specialists. 9 The clinical management of this case is summarized in Table 1 .
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1De Guzman E Shakeel H Jain R Thyrotoxicosis: a rare presentation of molar pregnancy BMJ Case Rep 20211407 e 24213110.1136/bcr-2021-242131 PMC 825854034226253 · doi ↗ · pubmed ↗
- 2Samra T Kaur R Sharma N Chaudhary L Peri-operative concerns in a patient with thyroid storm secondary to molar pregnancy Indian J Anaesth 2015591173974226755840 10.4103/0019-5049.170035 PMC 4697247 · doi ↗ · pubmed ↗
- 3Sharma S Sharma S Gandrabur L Amin B Rehmani R Singh A Molar pregnancy complicated by impending thyroid storm Cureus 20211311 e 1965634976452 10.7759/cureus.19656 PMC 8679175 · doi ↗ · pubmed ↗
- 4de Almeida C E Curi E Fde Almeida C R Vieira D F Thyrotoxic crisis associated with gestational trophoblastic disease Rev Bras Anestesiol 20116105604609, 331–33321920210 10.1016/S 0034-7094(11)70071-X · doi ↗ · pubmed ↗
- 5Mansour M Almasri R Amin N Atypical presentation of hyperthyroidism complicated complete hydatidiform mole in a 24-year-old female: a case report Ann Med Surg (Lond)202385126173617738098552 10.1097/MS 9.0000000000001381 PMC 10718378 · doi ↗ · pubmed ↗
- 6Pereira J V Lim T Hyperthyroidism in gestational trophoblastic disease - a literature review Thyroid Res 20211401133446242 10.1186/s 13044-021-00092-3PMC 7807451 · doi ↗ · pubmed ↗
- 7Wie J H Kwon J Y Ko H S Lee Y Shin J C Park I Y Thyroid storm and early-onset proteinuric hypertension caused by a partial molar pregnancy J Obstet Gynaecol 2016360335135226977975 10.3109/01443615.2015.1065229 · doi ↗ · pubmed ↗
- 8Chale-Matsau B Mokoena S Kemp T Pillay T S Hyperthyroidism in molar pregnancy: β-HCG levels do not always reflect severity Clin Chim Acta 2020511242732980362 10.1016/j.cca.2020.09.028 · doi ↗ · pubmed ↗