Ilizarov-assisted periosteal distraction for refractory arteriovenous malformation ulcers: first clinical report in Asia
Xiangyi Wu, Ren Cai, Mao Ye, Xitao Yang, Dachuan Sun, Yifeng Han, Xindong Fan, Jiaxue Zhu

TL;DR
This paper reports the first use of Ilizarov-assisted periosteal distraction in Asia to successfully treat a difficult-to-heal foot ulcer caused by an arteriovenous malformation.
Contribution
The study introduces a novel clinical application of Ilizarov-based neovascular stimulation for AVM-related ulcers in Asia.
Findings
Ilizarov-assisted periosteal distraction improved wound healing and resolved infection in a patient with a non-healing AVM ulcer.
75% of the wound epithelialized within 4 weeks, with granulation tissue covering the remaining area.
Abstract
Refractory ulcers caused by high-flow arteriovenous malformations (AVMs) pose significant therapeutic challenges due to persistent tissue ischemia and shear stress-induced graft failure. Traditional embolization or flap reconstruction strategies often yield suboptimal outcomes, particularly in weight-bearing regions. We present a 28-year-old female with a non-healing dorsal foot AVM ulcer despite multiple embolizations and radical toe amputations. Genetic testing revealed a KRAS mutation, confirming a somatic etiology of AVM. After a debridement and local flap repair, we employed Ilizarov-assisted periosteal distraction to improve local perfusion. 75% of the wound epithelialized and the infection resolved within 4 weeks postoperatively, with granulation tissue covering the remainder. This case highlights the mechanobiological advantages of Ilizarov-based neovascular stimulation in…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
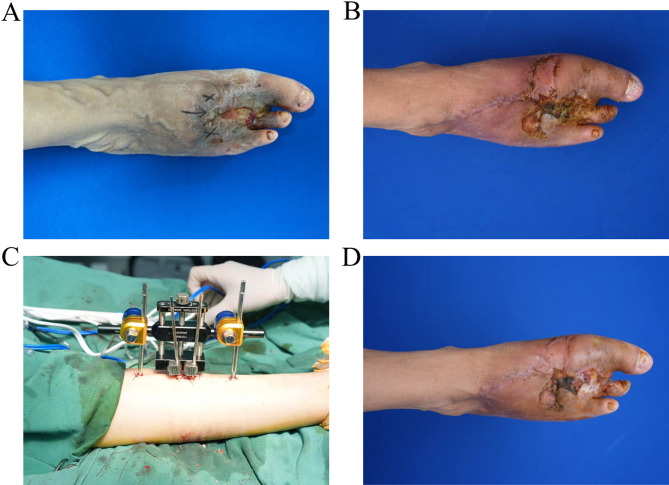 Figure 1
Figure 1- —https://doi.org/10.13039/501100001809National Natural Science Foundation of China
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVascular Malformations Diagnosis and Treatment · Vascular Malformations and Hemangiomas · Vascular Anomalies and Treatments
Introduction
Extremity AVMs account for 15–20% of congenital vascular anomalies [1], with nearly one-third progressing to chronic ulceration due to persistent arteriovenous shunting and resultant tissue hypoxia [2]. In addition to local ischemia, turbulent flow and shear stress within affected vascular beds contribute to poor graft take and wound recurrence, especially in the foot [3]. Although superselective embolization and tissue flap coverage are mainstays, their efficacy is often limited in weight-bearing zones or when nidus involvement is extensive [4].
Mechanobiological interventions, such as Ilizarov-based periosteal distraction, offer an innovative strategy to overcome microcirculatory deficits [5]. Inspired by distraction osteogenesis [6], this technique uses gradual mechanical tension to stimulate angiogenesis via VEGF upregulation and periosteal stem cell activation. We report the first case of Ilizarov-assisted wound healing in an AVM-related ulcer with a known KRAS6 mutation.
Report
A 28-year-old female presented to our hospital with a non-healing 5 × 4 cm ulcer on the dorsal aspect of the right foot. The lesion was overlying a diffuse, infiltrative Shobinger stage III AVM confirmed by angiography. Genetic analysis demonstrated a somatic KRAS mutation, supporting the diagnosis of congenital AVM.
Before admission, the patient underwent three sessions of Onyx embolization over the past decade, followed by repeated coil extrusion and skin breakdown episodes. In 2021, due to persistent ischemia and ulceration with exposed embolic material, she underwent radical amputation of the second and fourth toes. Despite temporary wound stabilization, new ulcerations developed over the dorsum and medial midfoot within 6 months postoperatively, complicated by methicillin-sensitive Staphylococcus aureus (MSSA) infection (Fig. 1A). Reluctant to undergo a full foot amputation, the patient sought further evaluation at our institution. On arrival, clinical examination revealed active drainage, poor perfusion, and exposed tendon without bone involvement. Following thorough debridement and local transposition flap coverage (Fig. 1B), we planned staged revascularization using the Ilizarov technique.
Fig. 1. Clinical presentation and intraoperative findings. (A) Preoperative photograph showing a chronic ulcer on the dorsum of the right foot measuring approximately 5 × 4 cm. The surrounding skin is pale and poorly perfused. (B) Wound after initial debridement and flap grafting. (C) Placement of the Ilizarov ring fixator and insertion of percutaneous Kirschner wires in the proximal and distal tibia for periosteal traction. (D) Four-week postoperative follow-up showing significant epithelialization and granulation tissue formation throughout the wound bed
Four 1.8 mm tensioned Kirschner wires were inserted into the proximal and distal tibia, secured via a circular fixator (Fig. 1C). Starting on postoperative day 5, periosteal distraction was initiated at 0.25 mm twice daily for 20 days. At 4 weeks, 75% of the area was re-epithelialized and granulation tissue covered the entire wound base. The skin surrounding the wound appeared erythematous with adequate perfusion (Fig. 1D). In addition, infection was controlled without the need for systemic antibiotic. At the 12-month follow-up, the patient resumed independent ambulation with no ulcer recurrence, reported minimal pain, and returned to normal daily activities.
Discussion
Chronic ulcers associated with AVMs are notoriously difficult to treat due to the complex interplay of ischemia, high-flow shunting, and mechanical stress [7]. KRAS mutations, now recognized as key somatic drivers of AVM pathogenesis, further implicate aberrant endothelial proliferation and vessel remodeling in disease progression [8, 9]. These molecular aberrations contribute to unstable vasculature, limited healing, and recurrent ulceration, as demonstrated in our patient [10].
Ilizarov periosteal distraction represents a novel mechanotherapeutic approach, particularly suited to ischemia-related wounds [11, 12]. Unlike standard revascularization or graft-based solutions, it leverages the body’s own regenerative pathways. Mechanical tension promotes upregulation of angiogenic factors (e.g., VEGF, PDGF), recruits mesenchymal stem cells, and enhances capillary sprouting from the inner periosteum [13, 14]. Moreover, the external fixator offloads pressure from the ulcer bed, reducing mechanical shear, a critical factor in our patient’s failure of previous grafts.
Compared with microvascular flap reconstruction, which provides immediate tissue coverage, the Ilizarov method is less invasive and better suited for compromised vascular beds. Flap-based interventions frequently fail in AVM-afflicted limbs due to inadequate perfusion and turbulent flow within the nidus [15]. Similarly, negative pressure wound therapy (NPWT) may enhance granulation and manage exudate, yet remains limited in the absence of underlying vascular restoration [16]. In contrast, the Ilizarov technique directly addresses the ischemic pathophysiology through localized angiogenesis and mechanical offloading, making it particularly advantageous for weight-bearing or previously embolized regions.
This case reinforces the feasibility and effectiveness of Ilizarov-assisted vascular stimulation in the management of AVM ulcers. Periosteal distraction may serve as a bridging therapy to avoid major amputation and promote durable closure in otherwise refractory wounds.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Coulie, J.; Seront, E.; Vikkula, M.; Boon, L. M., Extracranial arteriovenous malformations: towards etiology-based therapeutic management. J Clin Invest 2025, 135 (6), e 172837. 10.1172/jci 172837.10.1172/JCI 172837 PMC 1191020940091828 · doi ↗ · pubmed ↗
- 2Ben Abdallah, I.; Cerceau, P., Challenging Resection of a Massive Ulcerated Arteriovenous Malformation Within the Latissimus Dorsi Muscle. Eur J Vasc Endovasc Surg 2023, 66 (1), 118. 10.1016/j.ejvs.2023.05.001.10.1016/j.ejvs.2023.05.00137150476 · doi ↗ · pubmed ↗
- 3Huang, C. Y.; Liao, C. C.; Lin, P. C.; Yen, H. T.; Hsieh, C. H., Successful Treatment of a Chronic Venous Ulcer Caused by an Undiagnosed Arteriovenous Fistula: A Case Report. Ann Plast Surg 2025, 94 (6), 676–679. 10.1097/sap.0000000000004323.10.1097/SAP.000000000000432340358963 · doi ↗ · pubmed ↗
- 4Ma, J. X.; Xiao, X. D.; Shen, W. W.; Xia, Y. C., The clinical application of buried-suture method in the treatment of superficial arteriovenous malformations. J Plast Reconstr Aesthet Surg 2025, 104, 26–32. 10.1016/j.bjps.2025.02.017.10.1016/j.bjps.2025.02.01740101352 · doi ↗ · pubmed ↗
- 5Ryu, K. J.; Kim, B. H.; Hwang, J. H.; Kim, H. W.; Lee, D. H., Reamed Intramedullary Nailing has an Adverse Effect on Bone Regeneration During the Distraction Phase in Tibial Lengthening. Clin Orthop Relat Res 2016, 474 (3), 816–824. 10.1007/s 11999-015-4613-2.10.1007/s 11999-015-4613-2PMC 474617226507338 · doi ↗ · pubmed ↗
- 6Frierson, M.; Ibrahim, K.; Boles, M.; Boté, H.; Ganey, T., Distraction osteogenesis. A comparison of corticotomy techniques. Clin Orthop Relat Res 1994, (301), 19–24.8156672 · pubmed ↗
- 7Palić, B.; Mandić, A.; Prskalo, Z.; Fazlibegović, E., 32-year-old Traumatic Arteriovenous Fistula Presenting With Leg Ulcer and High-output Heart Failure. Vasc Endovascular Surg 2024, 58 (5), 544–547. 10.1177/15385744231225886.10.1177/1538574423122588638158801 · doi ↗ · pubmed ↗
- 8Al-Olabi, L.; Polubothu, S.; Dowsett, K.; Andrews, K. A.; Stadnik, P.; Joseph, A. P.; Knox, R.; Pittman, A.; Clark, G.; Baird, W.; Bulstrode, N.; Glover, M.; Gordon, K.; Hargrave, D.; Huson, S. M.; Jacques, T. S.; James, G.; Kondolf, H.; Kangesu, L.; Keppler-Noreuil, K. M.; Khan, A.; Lindhurst, M. J.; Lipson, M.; Mansour, S.; O’Hara, J.; Mahon, C.; Mosica, A.; Moss, C.; Murthy, A.; Ong, J.; Parker, V. E.; Rivière, J. B.; Sapp, J. C.; Sebire, N. J.; Shah, R.; Sivakumar, B.; Thomas, A.; Virasami, · doi ↗ · pubmed ↗